Chapter 25 Precision and Semi-Precision Attachments
Relevance of Precision and Semi-Precision Attachments to Esthetic Dentistry
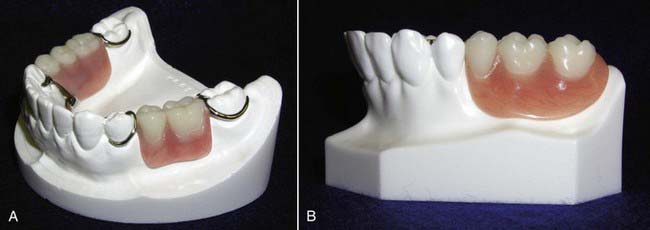
Precision and semi-precision attachment dentistry allows for esthetic removable partial dentures that do not display the metal clasps that can make traditional removable clasped cast partial dentures unesthetic. The attachment itself becomes the clasp, rest, reciprocating and stabilizing element and is hidden inside the partial denture, which renders it invisible. The attachment also provides the retentive element necessary to retain the partial in the mouth at rest and during masticatory function (Figure 25-1). Attachments are also used in segmented fixed partial denture and overdenture prosthetics on natural roots and implants. There are two parts to the attachment: a male and a female. In planning a removable partial denture, one part is incorporated into the casting or root on the crown, bridge, or splint, and the other part is incorporated into the removable partial framework or acrylic. As a result, the partial denture becomes highly esthetic and appealing to patients. Esthetically speaking, from a patient’s perspective, they smile with confidence, knowing that they have functioning, beautiful, natural-looking teeth.
Brief History of the Clinical Development and Evolution of the Procedure
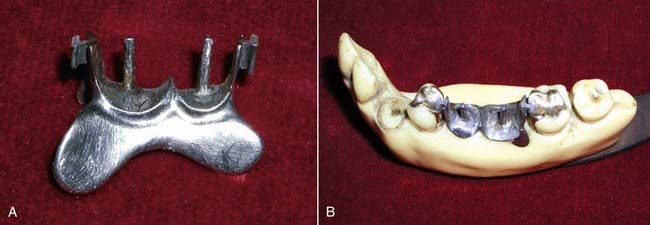
The use of attachments as connectors was popularized in the twentieth century by Dr Herman E.S. Chayes. He fabricated dental bridgework in segments that were connected by a key and keyway attachment (Figure 25-2). The attachments allow for micro-movement between segments and provide stress relief to the connected abutment teeth. His philosophy was to provide a physiologic tooth movement similar to that of natural teeth by using dental attachments in treatment planning prosthetics. This concept eventually led to the development of various rigid or resilient stress-relieving or stress-breaking attachments. Acting as a fixed bridge, Dr Chayes’s slot type of dental attachment was quite rigid and provided for removability and cleanseability. Over the years, attachments were fabricated to accommodate a wider range of controlled micro-movements and are now selected on a case-by-case basis, according to how the final prosthesis is planned to function on the remaining supporting elements.
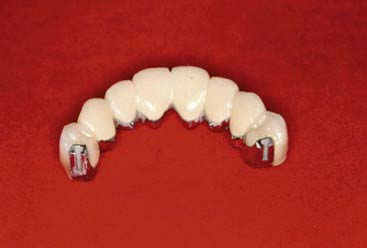
Various types of attachments have been developed. The precision attachments are very precise, and are milled out of alloy. The male and female parts fit together with tolerances of about 10 microns. They are purchased as a finished product and are soldered or cast to the final prosthesis (Figure 25-3). They are incorporated within the contours of the crown or splint and direct the forces of occlusion down the long axis of the tooth. They are generally rigid attachments in that the prosthesis is able to transfer most of the occlusal force to the teeth in which the attachments are incorporated, and less to the tissue-bearing areas.
The semi-precision attachments are much less precise in their fit and usually have much more resiliency than their precision attachment counterparts. These attachments are cast from refractory patterns, and the male or female parts may be made of nylon, polymer, or metal. These attachments can allow up to 15 degrees (or more) of rotational movement and up to 600 microns (or more) of vertical movement. Some offer hinge and/or lateral resiliency. In removable partial denture cases, they are cast with the crown or splint and are placed outside the contours of the teeth (Figure 25-4). In overdenture prosthetics, they are either cast on top of copings, incorporated onto posts which are cemented into the roots or abutment teeth or incorporated into overdenture implant abutments. Their resiliency allows the prosthesis to transfer most of the occlusal load to the tissues and away from the abutment teeth to which they are connected.

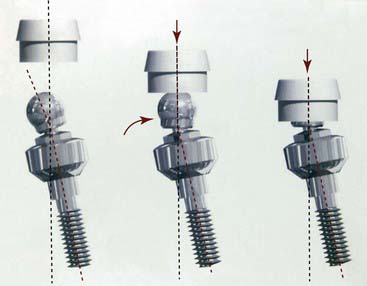
Relating Function and Esthetics
The treatment planning process often places both dentists and patients in a dilemma between function and esthetics. Removable cast partial dentures are fabricated with clasps, rests, and reciprocating elements that can create visibly unpleasant esthetics as well as wear and torque on the abutment teeth. Overdentures can be fabricated directly over cast copings or implant healing caps. Wthout the use of attachments however, the retentive and protective elements that attachments provide are lost. As a result, undue stress can be placed on the remaining roots or implants. Long-span fixed bridgework, fabricated in one piece, can be difficult to cast and fit properly. Attachments that will allow fixed bridges to be segmented can solve these problems. Diverse root or implant angulations may not be able to be corrected easily unless a segmenting attachment is used.(Figure 25-5). The use of dental attachments can obviate many of these problems as well as provide the desired esthetics. The typical Kennedy class 1, 2, or 4 clasped partial denture relies on teeth and soft tissues for stability and support. The use of Class 2 clasped lever designs with properly placed and designed clasps direct occlusal forces along the axial length of the supporting teeth and minimize torque to the abutment teeth. Clasps do not provide a resilient mechanism for forces to be redistributed to other areas of the mouth without causing movement or wear to the connected abutment teeth or supporting tissues.
Clinical Considerations
Indications
• Minimization of trauma to soft tissue
• Control of loading and rotational forces
• Non-parallel abutments–segmenting
Attachments are classified according to how they function in prosthetic designs:
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


