24
Class III malocclusion
Table 24.1 Factors determining the management of Class III malocclusion.
| Factor | Notes |
| Patient concerns | Dental concerns can be managed with orthodontics alone. Facial andlor functional concerns will often require orthognathic surgery |
| Motivation for treatment | Good dental health and motivation are required for complex treatment |
| Severity of skeletal discrepancy | A mild/moderate skeletal discrepancy may be treated with orthodontic camouflage particularly if the patient can achieve incisor edge-to-edge occlusion. A severe discrepancy can only be treated comprehensively with orthodontics and orthognatric surgery |
| Remaining growth | A malocclusion at the borerline of orthodontic corretion before the pubertal growth spurt is likely to deteriorate with differential mandibular growth |
| Degree of dento-alveolar compensation | Pre-existing dento-alveolar compensation limits the amount of further compensation achievable by orthodontic camouflage |
| Ability to achieve edge-to-edge bite | An ability to achieve edge-to-edge favours orthodontic camouflage as it indicates that less incisor movement is required for correction than suggested by the size of reverse overjet in centric occlusion |
| Depth of overbite | A deep overbite offers scope for camouflage by downwards and backwards rotation of the mandible (e.g. facemask) and improves stability of anterior crossbite correction |
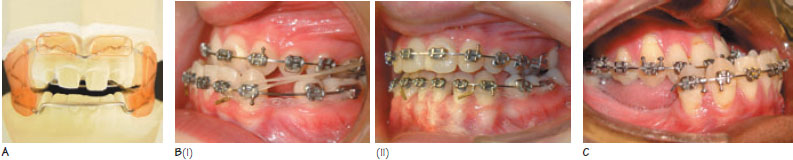
Figure 24.1 (A) The functional regulator III appliance. (B) An example of orthodontic camouflage, (i) Note use of Class III intermaxillary elastics to retract the lower incisors using the upper arch as anchorage (ii) after anterior crossbite correction. (C) Patient treated by alignment only as there were no facial concerns.
Class III is the term used to describe a malocclusion where two or more of the lower incisal edges occlude anterior to the cingulum plateau of the upper incisors (British Standards Institute incisor classification). The overjet (OJ) is reduced or reversed and there may be an anterior mandibular displacement. The molar relationship is often Class III.
The prevalence of Class III malocclusion shows ethnic variation. It is less common in Caucasians (prevalence 3%) than in the Japanese (5–10%).
Aetiology of Class III malocclusion
Skeletal factors
Class III malocclusion is commonly accompanied by a skeletal III pattern due to many possible factors including:
- increased mandibular length;
- forward positioning of the glenoid fossa;
- reduced maxillary length;
- short cranial base;
- reduced cranial base angle (Figures 3.1D and 3.1E);
- a combination of the above factors.
Rarely, this malocclusion can occur in association with a skeletal I or II pattern if the soft tissue environment is unfavourable. With favourable soft tissues, a skeletal III discrepancy may be compensated by upper incisor proclination and lower incisor retroclination (dentoalveolar compensation). In such cases, the OJ will not truly reflect the skeletal discrepancy. T/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


