CHAPTER 22. Anaemias, leukaemias and lymphomas
Box 22.1
Important effects of haematological diseases
• Anaesthetic complications
• Oral infections
• Prolonged bleeding
• Mucosal lesions
Haemoglobin estimation and routine indices are informative and should be carried out when any patient has suspicious signs in the mouth or has to undergo oral surgery.
ANAEMIA
Causes and important types are summarised in Table 22.1.
| *Alcoholism should always be excluded when macrocytosis in the absence of anaemia is found – it is a characteristic sign of alcoholism. |
|
| Type of anaemia | Causes or effects |
|---|---|
|
1. Iron deficiency (microcytic, hypochromic anaemia)
|
Usually due to chronic blood loss |
|
2. Folate deficiency (macrocytic)
|
Pregnancy, malabsorption, alcohol*, phenytoin-induced etc. |
|
3. Vitamin B 12 deficiency (macrocytic anaemia)
|
Usually due to pernicious anaemia, occasionally to malabsorption |
|
4. Leukaemia and aplastic anaemia (normochromic normocytic)
|
Raised susceptibility to infection and bleeding tendency often associated |
|
5. Sickle cell disease (normocytic anaemia)
|
Genetic. Sickle cells seen in special preparations
|
|
6. Beta-thalassaemia (hypochromic, microcytic)
|
Genetic. Many misshapen red cells
|
|
7. Chronic inflammatory disease (normochromic, normocytic)
|
Rheumatoid arthritis is a common cause |
|
8. Liver disease (usually normocytic)
|
Haemorrhagic tendency may be associated |
Iron deficiency (microcytic) anaemia is the most common type and usually results from chronic menstrual blood loss. Women of child-bearing age or over, or men with peptic ulcer or haemorrhoids are mainly affected.
Pernicious anaemia chiefly affects women of middle age or over and is the main cause of macrocytic anaemia. Unlike other anaemias, it can cause neurological disease, particularly subacute combined degeneration of the spinal cord.
Folate deficiency also causes a macrocytic anaemia, often in younger patients, particularly in pregnancy. It must be firmly differentiated from pernicious anaemia because administration of folate to the latter can worsen neurological disease.
Leukaemia is an uncommon but frequently lethal cause of normocytic anaemia, but should be suspected in an anaemic child.
Sickle cell trait is most common in immigrants from the West Indies. Sickle cell anaemia is relatively uncommon.
Thalassaemia is mainly seen in immigrants from the Mediterranean area.
Clinical features
Anaemia, irrespective of cause, produces essentially the same clinical features (Box 22.2), particularly if severe, but some anaemias have distinctive features.
Box 22.2
General clinical features of anaemia
• Pallor
• Fatigue and lassitude
• Breathlessness
• Tachycardia and palpitations
• Glossitis or other mucosal lesions
The complexion is a poor indicator of pallor. The conjunctiva of the lower eyelid, the nail beds and, sometimes, the oral mucosa, are more reliable. Cardiovascular signs (tachycardia or oedema of the ankles) result from severe anaemia. Glossitis and other mucosal diseases (Box 22.3) by contrast, can be the earliest signs as discussed below.
Box 22.3
Features of anaemia important in dentistry
Mucosal disease
• Glossitis
• Angular stomatitis
• Recurrent aphthae
• Infection, particularly candidosis
Risks from general anaesthesia
• Shortage of oxygen can be dangerous
Lowered resistance to infection
• Apart from candidosis, this is seen only in severe anaemia or when due to leukaemia
Mucosal disease
Glossitis
Anaemia is the most important, though not the most common, cause of a sore tongue. Soreness can precede a fall in haemoglobin levels, particularly when resulting from vitamin B 12 or folate deficiency, and can be their first sign. Later, there may be obvious inflammation and atrophy of the filiform papillae (Fig. 22.1). Variants of sore tongue have been discussed in Chapter 14, but it is emphasised again that this symptom always requires careful haematological investigation, initially by means of a haemoglobin level and routine indices. Serum iron, ferritin and red cell folate levels may be required. Even though the haemoglobin may be within normal limits, enlarged erythrocytes (mean corpuscular volume [MCV] .96 fl) frequently indicate pernicious anaemia. If any deficiency is found, the underlying cause, such as gastrointestinal disease, must be investigated.
 |
| Fig. 22.1
Iron deficiency anaemia. The tongue is slightly reddened, smooth and depapillated. There is also angular cheilitis as a result of candidal infection.
|
Recurrent aphthae
Aphthae are sometimes secondary to haematological deficiency, particularly of vitamin B 12 or folate, in patients whose aphthae start or worsen late in life.
Candidosis and angular stomatitis
Iron deficiency, in particular, is a predisposing factor for candidosis (Ch. 12). Angular stomatitis is also a classical sign of iron deficiency anaemia and due to candidosis.
Dangers of general anaesthesia
Any reduction of oxygenation can precipitate irreparable brain damage or myocardial infarction when there is significant anaemia. General anaesthesia should therefore be given in hospital. The dangers are particularly great in sickle cell disease, as discussed later.
Lowered resistance to infection
Oral candidosis is the main example but, in the past particularly, osteomyelitis could follow extractions in severe anaemia (Fig. 22.2). Currently, sickle cell disease is more important in this context.
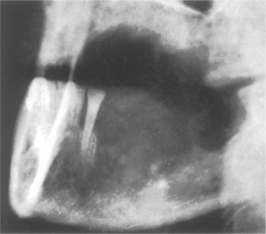 |
| Fig. 22.2
Acute osteomyelitis in an anaemic patient. Widespread bone destruction followed straightforward extraction of the posterior teeth. The patient was found to have a haemoglobin level of 4 g/dl.
|
SICKLE CELL DISEASE AND SICKLE CELL TRAIT
Sickle cell anaemia mainly affects people of African, Afro-Caribbean, Indian, Mediterranean or Middle Eastern origin. About 5000 persons in Britain are estimated to have sickle cell disease (homozygotes), but many more have sickle cell trait (heterozygotes). The defect in sickle cell disease is an abnormal haemoglobin (HbS) with the risk of haemolysis, anaemia and other effects. In heterozygotes, sufficient normal haemoglobin (HbA) is formed to allow normal life with only rare complications.
Sickle cell disease
The complications arise from polymerisation of deoxygenated HbS, which is less soluble than HbA. This forms long fibres which deform the red cells into sickle shapes and makes them vulnerable to haemolysis. Chronic haemolysis causes chronic anaemia, but patients, under normal circumstances, typically feel well, as HbS more readily releases its oxygen content to the tissues than HbA. Exacerbation of sickling raises blood viscosity, causing blocking of capillaries and sickling crises (Boxes 22.4 and 22.5).
Box 22.4
Factors that can precipitate sickling crises
• Hypoxia, particularly from poorly conducted anaesthesia
• Dehydration
• Infections (including dental)
• Acidosis and fever
Box 22.5
The main types of sickling crises
• Painful crises
• Aplastic crises
• Sequestration crises
These patients are also abnormally susceptible to infection, particularly pneumococcal or meningococcal, and osteomyelitis.
Painful crises are caused by blockage of blood vessels and bone marrow infarcts. Painful crises can affect the jaws, particularly the mandible, and mimic acute osteomyelitis clinically and radiographically. The infarcted tissue forms a focus susceptible to infection, and Salmonella osteomyelitis is a recognised hazard.
Aplastic crises are caused by human parvovirus B19 infection and require immediate transfusion.
Sequestration crises result from sickle cells pooling in the spleen, liver or lungs. An acute chest syndrome, with pain, fever and leucocytosis, is the most common cause of death.
Dental aspects of sickle cell trait and disease
Sickling trait should be suspected, particularly in those of Afro-Caribbean origin, and investigated if anaesthesia is anticipated. If the haemoglobin is less than 10 g/dl, the patient is probably a homozygote with sickle cell disease. Screening tests depend on the lower solubility of HbS which produces turbidity when a reducing agent is added. Confirmation is by electrophoresis.
In those with sickle cell trait, the main precaution is that general anaesthesia should be carried out with full oxygenation. In sickle cell disease, the oral mucosa may be pale or yellowish due to haemolytic jaundice. Radiographic changes can be seen in the skull and sometimes the jaws (Ch. 10).
Occasionally, crises may be precipitated by dental infections such as acute pericoronitis. Prompt antibiotic treatment is therefore important. Painful bone infarcts should be treated with non-steroidal anti-inflammatory analgesics and fluid intake should be increased. Admission to hospital is required for severe painful crises not responsive to analgesics. Rigorous routine dental care is necessary because of the susceptibility to infection.
THE THALASSAEMIAS
Alpha-thalassaemias mainly affect Asians, Africans and Afro-Caribbeans, while beta-thalassaemias mainly affect those from the Mediterranean littoral such as Greeks (thalassaemia – literally, ‘sea in the blood’).
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


