CHAPTER 20. Soft tissue (mesenchymal) neoplasms
BENIGN TUMOURS
Neurofibromas
These uncommon tumours arise from nerve sheaths. They form smooth, painless lumps in the mouth. When seen in the mouth, neurofibromatosis should be suspected.
Histologically, neurofibromas are cellular with plump nuclei separated by fine, sinuous collagen fibres among which mast cells can usually be found. Excision is curative.
Neurilemmomas
Neurilemmomas arise from axon sheaths and are also uncommon. They also form painless smooth swellings.
Histologically, the appearance is distinctive with multiple rounded masses of elongated spindle cells with palisaded nuclei (Antoni A tissue –Fig. 20.1). There is also a variable amount of unorganised loose connective tissue with scanty cells, sometimes with pleomorphic nuclei (Antoni B tissue). Excision is curative.
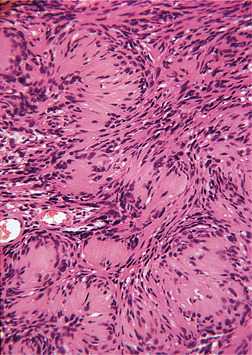 |
| Fig. 20.1
Neurilemmoma. Antoni A tissue showing striking palisading of nuclei.
|
Lipoma and fibrolipoma
Lipomas can occasionally grow, particularly from the buccal fat pad, as soft, sometimes yellowish, swellings, which may be pedunculated (Fig. 20.2). They grow slowly and cause no symptoms unless bitten, or become conspicuous because of their size.
 |
| Fig. 20.2
Lipoma of the cheek. The tumour forms a pale, very soft yellowish swelling.
|
Histologically, lipomas consist of apparently normal fat (Fig. 20.3) comprising adipocytes with single large cytoplasmic fat vacuoles. The fat cells are supported by thin fibrous tissue septa and usually surrounded by a variable thin fibrous capsule (Fig. 20.4). When fibrous tissue forms a large part of the tumour it is called a fibrolipoma. Lipomas should be excised.
 |
| Fig. 20.3
Lipoma. The lobular structure of the fat is visible.
|
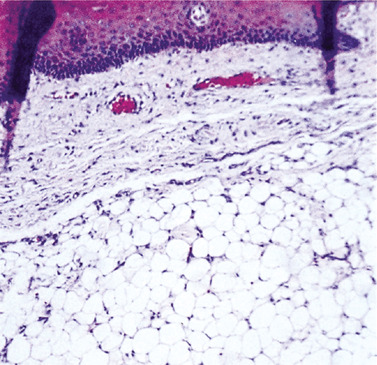 |
| Fig. 20.4
Lipoma. The fat cells are closely packed between septa of fibrous tissue and often only partially encapsulated at the margin.
|
Granular cell tumour
Clinically, granular cell tumours typically form painless smooth swellings. The tongue is the most common site.
Histologically, large granular cells form the bulk of the lesion. Electron microscopy suggests that the granular cells originate from Schwann cells. However, in the light microscope, all stages of apparent transition between striated muscle cells and granular cells are found at the periphery and are a striking histological feature (Fig. 20.5). Centrally, the granular cells are large, with clearly defined cell membranes and filled with eosinophilic granules that are lysosomes, with cell debris, mitochondria and degenerate cell membrane.
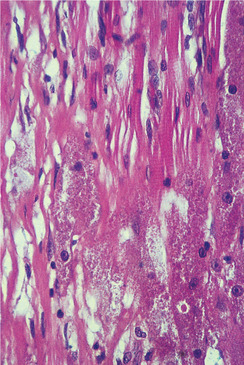 |
| Fig. 20.5
Granular cell tumour. At high power, the granular cells apparently merging with muscle fibres are characteristic and indicate the diagnosis.
|
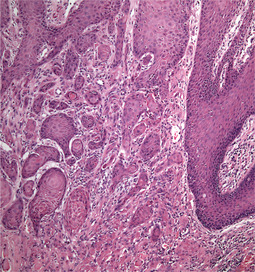
The granular cell tumour can induce striking pseudoepitheliomatous (pseudocarcinomatous) hyperplasia of the overlying epithelium (Figs 20.6 and 20.7). Though only present in a minority, this may be florid such that granular cell tumours have been mistaken histologically for carcinomas with resulting overtreatment. Simple excision should, however, be curative.
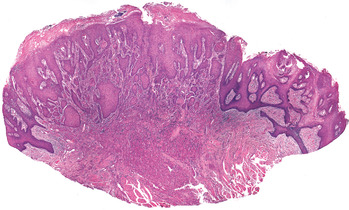 |
| Fig. 20.6
Granular cell tumour. The irregular proliferation of the overlying epithelium (pseudoepitheliomatous hyperplasia), which is very florid in this example, may mimic a squamous carcinoma in superficial biopsy specimens.
|
 |
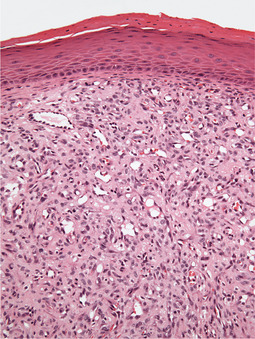
| Fig. 20.7
High power of a superficial area in Figure 20.6 showing the small irregular islands of epithelium that appear to invade the fibrous tissue and superficial muscle. Some show keratin formation similar to keratin pearls in squamous carcinoma. Granular cells are only present along the lower edge of the figure.
|
Congenital (granular cell) epulis
The rare congenital epulis is typically present at birth as a smooth but prominent soft nodule usually on the alveolar ridge (Fig. 20.8). Females are predominantly affected and, occasionally, the mass is so large as to obstruct respiration.
 |
| Fig. 20.8
Congenital epulis. A firm pink non-ulcerated nodule on the alveolar ridge of a neonate is the typical presentation.
|
Histologically, large pale granular cells with sharply defined cell membranes are covered by epithelium with lacks pseudoepitheliomatous hyperplasia. Immunohistochemistry suggests that the origin is myogenous. Excision is curative but spontaneous regression is also seen.
Haemangiomas → Summary p. 337
Haemangiomas are mostly vascular malformations. Vascular neoplasms (apart from Kaposi’s sarcoma) are rare.
Haemangiomas may be localised, but are occasionally diffuse and associated with similarly affected areas of the face. Rarely, the meninges are also involved, causing epilepsy and mental defect (Sturge–Weber syndrome). Isolated haemangiomas form purple, flat or nodular lesions which blanch on pressure (Fig. 20.9). Histologically, haemangiomas comprise either capillary, cavernous or both types of vessels. The capillary type consists of innumerable minute blood vessels and vasoformative tissue – mere rosettes of endothelial cells (Fig. 20.10). The cavernous type consists of large blood-filled sinusoids.
 |
| Fig. 20.9
Cavernous haemangioma of the cheek. The colour is deep purple and the structure, a mass of thin-walled blood sinuses, is visible through the thin epithelium. A mass engorged with blood and as prominent as this is liable to be bitten and bleed profusely.
|
 |
| Fig. 20.10
Capillary haemangioma. Numerous large and small closely packed capillary vessels extend from the epithelium into the deeper tissues.
|
Excision of mucosal haemangiomas should be avoided unless trauma causes repeated episodes of bleeding. Cryosurgery may allow removal of a haemangioma without excessive bleeding.
Lymphangioma
These uncommon tumours usually form pale, translucent, smooth or nodular elevations of the mucosa. However, they may be noticed because they suddenly swell and become dark purple due to bleeding into the lymphatic spaces. Rarely, lymphangiomas are diffuse and extensive and cause generalised enlargement of the tongue (macroglossia) or lip.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


