CHAPTER 2
Recognising the Problem
Is an Attractive Smile Important?
Facial attractiveness impacts on how an individual is seen by others, and a good display of well-aligned teeth is important for psychological well-being. The smile line is important; the incisal edges of the upper incisors should follow the lower lip, with almost the full crown displayed to give good facial balance. In addition, the dental arch should be broad with the first and perhaps the second premolars showing.
Specific angles or measurements cannot be prescribed for facial aesthetics as we are all different, but in general good facial aesthetics is dictated by:
- symmetry;
- harmony;
- balance.
The overall facial attractiveness depends on the skeletal relationship of the maxilla and mandible, and the tone and movement of the soft tissues.
From a clinical perspective it is important to remember that the position of the teeth is reliant on the position of the jaws within the facial skeleton, the effects of the soft tissue forces of the tongue intraorally and the cheeks and lips extraorally, and the relative sizes of the jaws. It is also important to consider racial and sexual differences in the position of the dentition.
During the initial assessment of a patient it is important to have an overall impression of facial form and head posture. The facial form of the child is likely to be similar to that of other members of the family, so an assessment of siblings and both parents will be very helpful in determining the likely growth pattern of the child. A full medical and dental history should always be taken to highlight any factors that could impact on the growth or treatment of the child. The physical growth status of the child should be assessed to determine if their chronological and developmental ages are consistent. Clinical examination is everything (Figure 2.1).
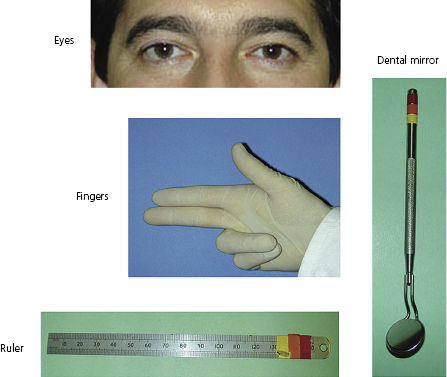
Clinical assessment of the anteroposterior (A–P) plane is done by palpating for the clinical A point (the maximum concavity of the anterior part of the maxilla) and B point (the maximum concavity of the anterior part of the mandible) (Figure 2.2). This will give the rough position of the maxilla relative to the mandible. In a Class I relationship the maxilla is a few millimetres behind the mandible. With the fingers (either intra- or extra-orally) on the A and B points, the clinician can ‘feel’ if there is a discrepancy. Normally, the first finger is a few millimetres shorter than the middle finger. If the skeletal bases are basically Class I, the fingers will lie straight as the maxilla should be a few millimetres ahead of the mandible. If there is a significant discrepancy, one or other finger will be bent.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


