2
Effective Data Management and Communication for the Contemporary Orthodontist
Summary
In this modern competitive era, technology offers all of us modalities we can use to stand above the rest. Health information technology has the potential to greatly improve healthcare alongside yielding huge savings. Over the past several decades, computer systems and information technology have pervaded all aspects of dentistry, successfully bridging the divide between the clinical setting and research. However, this transformative technology demands learning of new skills to understand, maintain and use it effectively, and to deliver what it promises to deliver. The role of communication processes, verbal/nonverbal, oral/written, in human interactions needs no emphasis, as it forms the core basis of all successful relationships across humanity beyond creed, race, and ethnicity. One such relationship is the doctor–patient relationship, which is constantly evolving. Having moved from paternalistic to ‘equal partners’, it is now more likely progressing towards a ‘service provider–consumer’ format. Moreover, in the new ‘cyber age’ reliance on electronic communication is constantly on the rise, far superseding interpersonal contacts. This chapter discusses the integration of information technology systems in orthodontics, to improve work flow and efficiency, as well as for the management and protection of electronic data from theft and corruption. It also discusses the various methods of electronic communication in patient management per se, as well as electronic communication with other specialists and peers, and its increasing role in orthodontic education.
Introduction
Information technology refers to the use of computers and software to produce, manipulate, store, communicate, and/or disseminate information. Computerized data management systems are becoming an integral part of any healthcare system and transforming it through integration of all clinical disciplines. Although encoding clinical data into a computer is a positive step, it is not enough. A continuity-of-care record is needed in order to document, measure, support and coordinate within and between specialties. The challenges in this task include the threat of information overload, the need to provide for data-sharing between specialists, the appropriate use of the data for the delivery of healthcare, and prevent misuse and loss of data. All of these challenges need to be considered before installation of health information technology (Boyd et al., 2010).
Effective communication is defined as the exchange of information and a person’s beliefs to provide feedback and communicate one’s message. When translated to the doctor–patient scenario, communication entails the ability of the doctor to comprehend fully the patient’s concern and medical information, diagnose the problem, and advocate a treatment plan, to the satisfaction of both parties. In this communication process, the doctor and the patient assume the roles of the communicator and the receiver, alternately, until a common consensus is arrived at. The ultimate goal of an effective communication process is to foster a strong doctor–patient relationship, linked to important outcomes of care–treatment compliance (Francis et al., 1969; DiMatteo, 1995), clinical outcomes (Greenfield et al., 1988; Kaplan et al., 1989), malpractice claims (Beckman et al., 1994), and transfer of patients between doctors (Marquis et al., 1983). Evidence indicates that good doctor–patient relationships are on the decline, due to consumer-centric attitudes, decrease in professionalism, and commercialization of healthcare delivery systems (Chaitin et al., 2003). The path to a better doctor–patient relationship demands better communication, aimed at the patient’s perspective of treatment and includes the patient as a collaborative partner with his or her doctor (Roter, 2000; Murphy et al., 2001), beginning with scheduling the patient’s initial visit, progressing through diagnostic records, scheduling diagnosis, treatment planning, finances, finally culminating in the execution of the treatment plan. All the aforementioned tasks are aided by use of software programs that can enhance the doctor–patient experience, taking it to previously inconceivable heights.
The Role of Information Technology in the Orthodontic Practice
Practice Management Systems
Practice management software (PMS) is a computer program/s that performs and organizes the administrative and clinical areas of an orthodontic practice. Traditionally PMS was limited to administrative tasks, and the electronic medical record (EMR) system was meant for maintaining patient medical records. However, the current versions of PMS available for orthodontic use have integrated EMRs and track appointments, billing, clinical information, and aids in patient communication, helping orthodontists to manage everyday tasks more efficiently than ever. A PMS also tracks referrals with generation of new referral reports, while managing incoming referrals from other specialists.
Patient Demographic Documentation by the Assistant
Patient demographic documentation often starts when a new patient fills out a detailed information chart, which includes the patient’s name, address, contact information, birth date, employer, and insurance information. Office staff manually enter this information into the software. The software can automatically interact with the relevant insurance company server in real time when connected over the internet, to verify the patient’s credentials.
Scheduling Patient Visits
Patient appointment scheduling programs, the most important among administrative tasks, should consider proper management of the practitioner’s time, cost-effectiveness, flexibility, which can reduce overheads and increase patient satisfaction. Various software programs are available for scheduling patient visits – integrated through an interactive voice-based system (IVRS), which can be phone based or integrated into the office website (web based). The web module IVRS may be integrated into a single program that is also amenable to manual entries by the office staff. Such administrative applications deployed over the internet, enable patients to interact with the organizational aspects of the orthodontic practice. Online appointment scheduling, pre-registration, pre-visit preparations, and out-of-pocket treatment cost estimates all enhance communication and convenience. By having more control and a sense of participation in the administrative processes of the orthodontic office, patients may develop greater trust in the practice as a whole and potentially a better relationship with the doctor (Anderson et al., 2003).
Payment/Financial Record Maintenance
It is paramount to document financial details for each appointment, to ensure transparency and ease of insurance claims, if applicable. Each charge usually corresponds to a particular service performed during a particular appointment, and most of the time multiple treatment procedures are performed by the operator. The settlement of the insurance claim, if applicable, may be performed as an automated process by the software, using proprietary electronic data interchange with the insurance company’s server. This process is termed electronic claims submission (ECS). Electronic fund transfer (EFT) is the process whereby patients can pay a fee by electronic means, such as credit/debit card. Online banking can be automatically drafted by the software, enabling automatic debit from the payer’s account, and deposit it into the practice’s account on due dates (Lewis, 2006). The aforementioned steps of appointment scheduling, capturing patient demographics, and performing billing tasks are usually integrated into one module – the PMS (Table 2.1).
Table 2.1 Comparison of patient management software systems
| Software | Website | Special features |
| Dentimax | www.dentimax.com/ | IVRS, e-module |
| SaralDent Dental | www.saralindia.com/ | Manual SMS and email reminders |
| Medipac Dental | www.e2ilabs.com/ | Automated SMS and email reminders |
| Curve Hero | www.curvedental.com/ | Web-based interface; anytime/anywhere access |
All are shareware. Free demo copies can be downloaded from the company websites.
IVRS, interactive voice-based system.
Advantages of Using PMS
A PMS:
- Enables easy identification of new patients and round-the-clock appointment scheduling
- Enhances ability to manage multiple appointment schedules
- Helps locate patient records easily by name or date
- Makes easy the process of call-backs, rescheduling, and referring of patients to different offices
- Minimizes recalls, missed and overlapping appointments
- Makes possible cross-scheduling among multiple clinics and medical offices
- Reduces staffing and administrative overhead, thus enhancing revenue
- Has built-in reports that help save time and reduce paper clutter
- Prompts sending reminder letters/phone calls/SMS to patients in what are known as patient communication systems
- Reduces stress for the patients and staff
- Eliminates the need to physically transfer patient information from one place to another
- Enables transparency in financial transactions with the use of EFT and ECS.
Although an electronic patient record (EPR) offers several advantages over conventional paper records, it suffers the risk of tampering. Attorney Arthur Pearson points out that in case of litigation, the prosecution could easily argue that the patient’s electronic record has been tampered with, and this would put the defendant in an indefensible position (Scholz, 1989). Methods to overcome this issue include creating monthly duplicates of datasets, which are placed in an offsite data server ‘escrow’, or having printed records, as well. The former option is expensive and, the latter defeats the very purpose of having a ‘paperless’ electronic record. Current PMS/EMR program databases have features discouraging/preventing tampering. They usually require two digital signatures for every entry completed. Any changes/additional entries are added as a separate addendum entry. Tampering is quite an arduous task, even for experienced programmers. In the unlikely event that data have been tampered with, the electronic trail is traceable in case of litigation (Starke and Starke, 2006).
The deployment of PMS or other solutions for a ‘paperless office’ requires the setting up of a local area network (LAN) with a server and client system architecture (Haeger, 2005). Alternatives include internet program delivery (IPD)- or application service provider (ASP)-based solutions, which are basically outsourced hosting and delivery of management software, including data backup and archiving, and therefore do not require extensive hardware setup in the office.
Advantages of ASP solutions over office installed/maintained programs include (Lewis, 2006):
- No need to enforce local data management and protection systems
- EPRs are recorded/stored in the ASP server and thus available from any geographical location in the internet-connected world
- The patient data access system is easily integrated on the office website, providing patients, insurance agencies, and referring doctors with easy access
- Customer support is rapid in case of the unforeseen event, because the servers are offsite, in the custody of the ASP provider.
Although safety of patient data is of major concern as the data is stored on ‘out of office’ servers, these ASP servers are managed by professionals, and are compliant with privacy norms and data protection policies.
Computer-Aided Diagnosis and Treatment Planning to Enhance Communication
Case Documentation
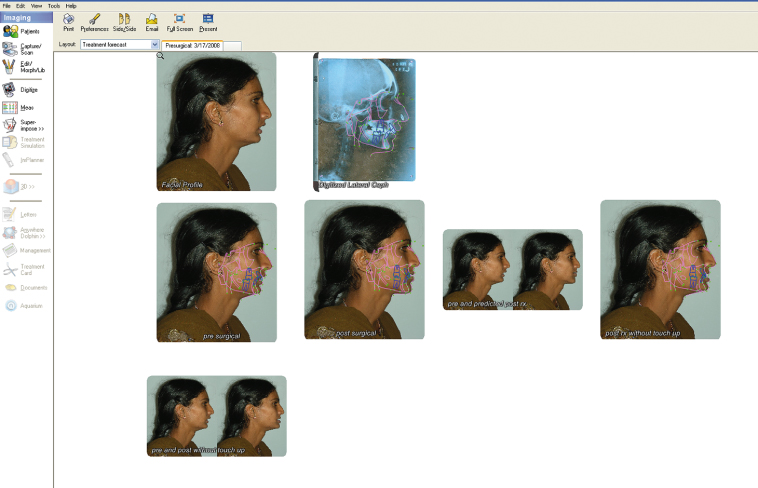
The majority of available software for orthodontic offices includes case documentation modules for routine dental complaints, and special modules for all dental specialties (Figure 2.1). These programs allow the practitioner to make accurate diagnoses and create compelling treatment plans. Some software vendors offer case sheet customization based on the practitioner’s needs. The integrated functions and features enable the practitioner to present recommendations to patients in a way that they can understand, making communication easier.
Figure 2.1 Example of an orthodontic case documentation module.
Diagnostic Record Taking
Digital Photographs
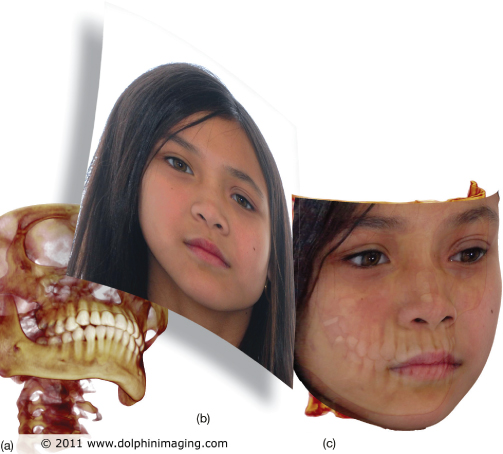
Digital photography has replaced film-based cameras due to its unparalleled advantages in routine clinical practice over conventional film images, for example immediate visualization of the captured image, possibility of image enhancement, indefinite ‘shelf life’ of the ‘soft copy’, ease of printing and duplication, absence of film, processing costs, and ease of electronic transmission around the world (Sandler et al., 2002; Revankar et al., 2009a). Further, the immediate availability of images enables the doctor to demonstrate the current status of the patient’s dentition and extraoral features to them. Digital photography experience has been enhanced by availability of programs that can perform wireless transfer of photographs from the camera to the computer (Revankar et al., 2010), ability to automatically tag photographs with DICOM (digital imaging and communication in medicine)-compatible data, automatic parsing of duplicate photographs, and colour/hue matching (Halazonetis, 2004). It is now possible to integrate cone-beam computed tomography (CBCT) data in DICOM format with standard extraoral frontal photographs of the patient to generate three-dimensional (3D) facial photographs without the need for 3D facial camera systems (Mah, 2007). This is sometimes referred to as 2D facial photo wrap (Dolphin Imaging and Management Solutions, Chatsworth, CA) (Figure 2.2) and is definitely a giant step ahead in rendering a visual identity to the patient’s 3D volume.
Figure 2.2 2D facial wrap. (a) 3D craniofacial skeleton rendering from cone-beam computed tomography data. (b) Standard 2D digital photograph of the patient. (c) Facial photo wrap.
(Image courtesy of Dolphin Imaging and Management Solutions, Chatsworth, CA; www.dolphinimaging.com.)
E-Models
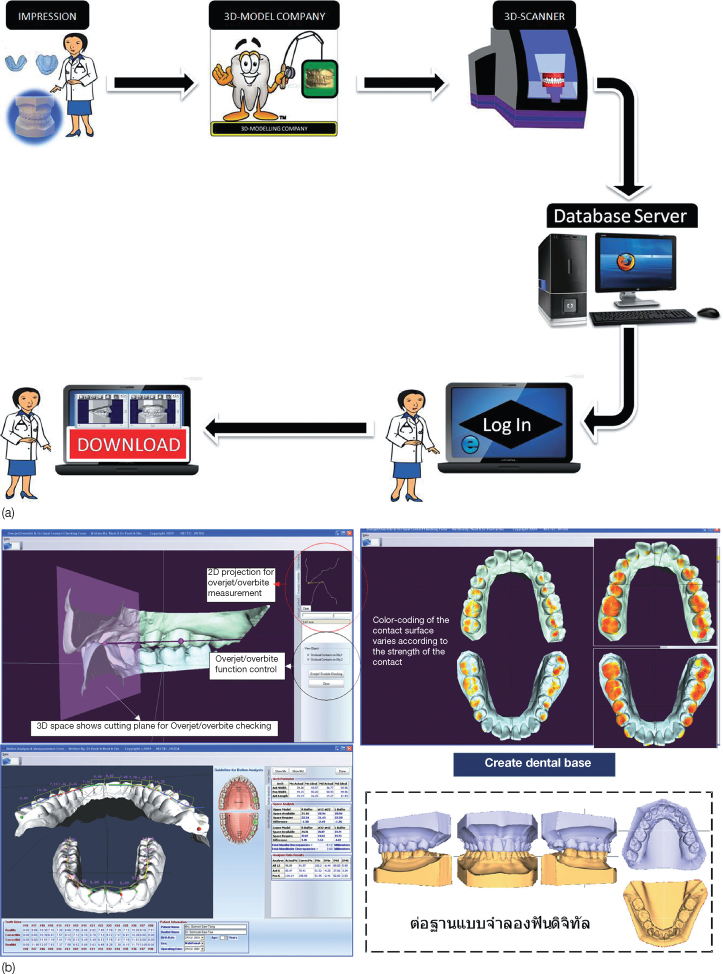
The transition from physical study models to 3D images is progressing slowly due to the expensive nature of the 3D model scanners. Desktop-based model scanners are available both in the LASER (light amplification by stimulated emission of radiation) and optical/white structured light variety (Table 2.2). However, outsourcing options are available, whereby the physical models or impressions can be sent to the 3D modeling company and the 3D models generated from it are downloaded through the internet (Table 2.3). The orthodontist has to log on to the company website with his or her unique case ID enabling round-the-clock access to the digital models (Figure 2.3). These 3D models have proved to be viable alternatives to plaster models, in terms of measurements, diagnosis of malocclusion, and treatment planning (Tomassetti et al., 2001; Stevens et al., 2006).
Table 2.2 Commercially available desktop model scanners

STL, stereolithography; ASC, Autodesk, Inc 3D file; DICOM, digital imaging and communications in medicine; OBJ, wavefront technologies format; PLY, polygon file format; VRML, virtual reality modeling language.
Table 2.3 Commercial outsourcing-based digital modeling and archiving solutions
| Solution | Company | Website |
| Orthocad | Cadent, Carlstadt, NJ, USA | www.cadentinc.com |
| e-model | GeoDigm, Chanhassen, MI, USA | www.geodigmcorp.com |
| Orthoplex | Dentsply GAC International Bohemia, NY, USA | www.gacintl.com/orthoplex |
| Ortholoine | Objet Geometries Inc Billerica, MA, USA | www.objet.com/Pages/Case_Studies/Medical/Ortholine |
| Anadent 3D | Sinthanayothin C, Thailand | www.anadent3d.com |
| Orthomodel | Tarcan B, Istanbul, Turkey | www.orthomodel.com/eng |
Figure 2.3 (a) Flow chart for outsourcing plaster model digitization.
(Courtesy of Dr Roopak D. Naik, Dharwad, India.)
Clockwise from left – the doctor ships the rubber base impressions or plaster casts to the 3D model company and 3D scanning is accomplished in the company’s scanner. Following this the digital models are available on the company’s secure login webpage where the doctor logs in to see the models or download them. (b) Visualization and manipulation of digital models in Anadent 3D software.
(Image courtesy Dr Sinthanayothin C, NECETC, Thailand.)
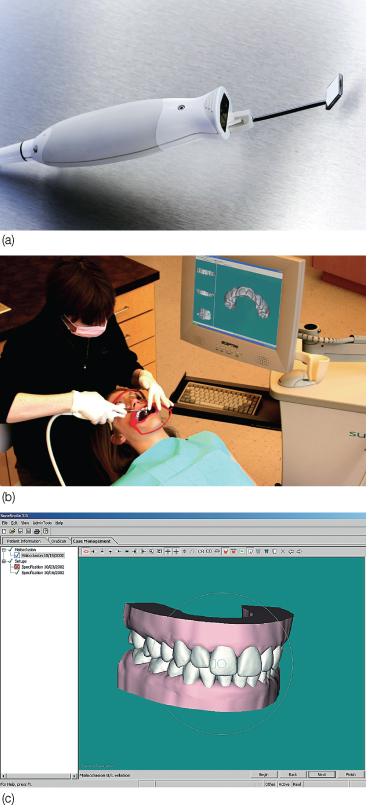
An alternative to standard impression techniques is intraoral scanning, termed ‘dedicated impression scanning systems’ and capable of generating 3D models. The first dedicated impression scanning system in orthodontics is the Orascanner (Suresmile, OraMatrix, Richardson, Texas, USA), a light-based imaging device that projects a precisely patterned grid onto the teeth. The orthodontist can make a diagnosis and plan treatment on the computer, using software tools to measure tooth and arch dimensions (Mah and Sachdeva, 2001). The virtual models also act as a valuable tool for patient education (Figure 2.4).
Figure 2.4 (a) The Orascanner apparatus. (b) Intraoral scanning with the Orascanner. (c) 3D digital model generated from the scan.
(Image courtesy Dr Rohit Sachdeva, OraMetrix, Inc., Richardson, TX.)
Digital Radiography
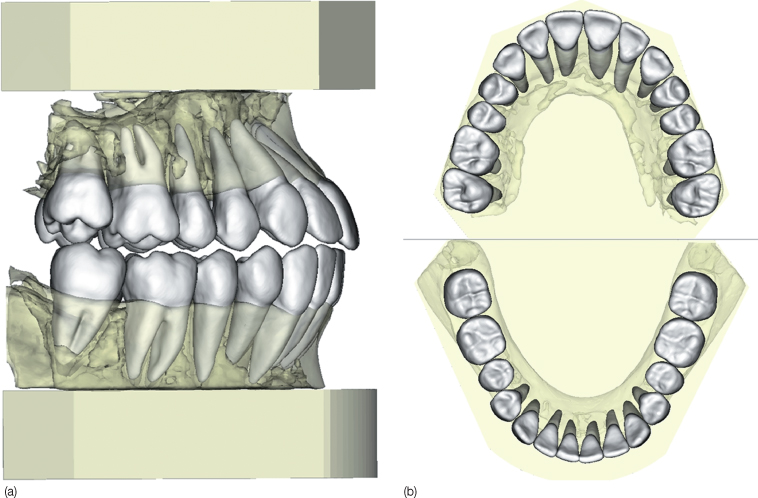
Radiographic imaging has now progressed from 2D to 3D with the increasing use of CBCT. 3D CBCT scans are also being used as alternatives to standard plaster models (Figure 2.5) and 3D-based dental measurement (3DD) programs (El-Zanaty et al., 2010). The advantages of 3D CBCT models over conventional plaster and other forms of digital models are (Chenin et al., 2009):
- Include not only the tooth crown, but also the roots
- Impactions/developing teeth and alveolar bone can be visualized
- Dynamic virtual setup simulation and generation of stereolithographic models using computer-aided manufacturing (CAM) is possible.
Figure 2.5 Dental models generated from CBCT data. (a) Models on bases trimmed to ABO standards. (b) Occlusal views.
(These digital models were generated with Anatomodel software. Anatomage Inc., San Jose CA www.anatomage.com; reproduced with permission from German and German, JCO April 2010).
Two-Dimensional Cephalometry
There have been tremendous advancements in the field of lateral cephalometric radiograph digitization, tracing, analyses, and treatment prediction, and a horde of cephalometric software is available for this mundane task. Online cephalometric analysis alternatives (Abraham, 2007) are also available (per case charge) that do not require the purchase and instalation of software (Table 2.4). Either digital or film radiographs, scanned or photographed on a viewer, can be used with a scale adjacent to the film that enables software calibration. At the time of writing, digitization of the film prior to automatic analysis is on the brink of change from manual to automatic landmark identification, using the ‘neural-associative-processor-based’ hardware recognition systems (Yagi and Shibata, 2003). These systems have been demonstrated successfully to identify landmarks automatically, with high accuracy without human input in both adults and adolescents (Tanikawa et al., 2010).
Table 2.4 Comparison of various 2D and 3D cephalometric software
| Software | Website | Special features |
| Viewbox | www.dhal.com | 3D module for CBCT data |
| Onyxceph | http://2i.webworld.org/ | Model analysis from photographs |
| Ceph Basic | www.image-instruments.de/ceph-basic/en/index_us.htm | Includes patient education module |
| Dolphin Imaging | www.dolphinimaging.com | 3D module for CBCT data |
| Vistadent | www.gactechnocenter.com/V3D.htm | 3D module for CBCT data |
| Anatomage 3D | www.anatomage.com | Automatic digitization |
| Cephanalysis.com | www.cephanalysis.com | Outsourcing; per case |
CBCT, cone-beam computed tomography.
Three-Dimensional Cephalometry
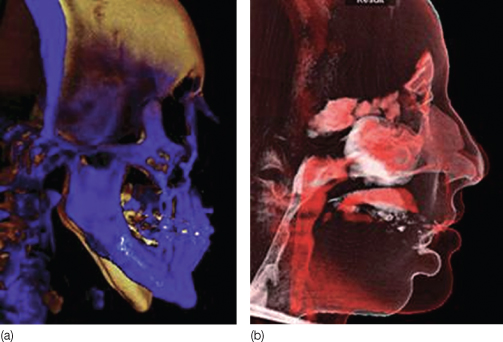
Since the inception of the cephalostat, Broadbent tried advocating a 3D stereoscopic analysis, and suggested combined use of the lateral cephalogram, postero-anterior radiograph, and a submental vertex view (Broadbent, 1931). However, the essence of Broadbent’s cephalostat was lost over the decades, when orthodontists worldwide used the lateral cephalogram, which is a 2D representation of a 3D object, as the primary diagnostic head film with its inherent disadvantages. As pointed out earlier, 3D cephalometry with the newer CBCT machines is as close as it can get to craniometry in the intact human (Gribel et al., 2011a,b). The biggest problem with 3D cephalometry is the absence of population norms for the 3D measurements, and this was recently addressed by Gribel et al. (2011a,b). Assessment of changes due to growth or treatment as well as evaluation of internal structures can be done using 3D volumetric superimposition technology (Dolphin 3D, Dolphin Imaging and Management Solutions, Chatsworth, California, USA).
Figure 2.6 Pre- and post-3D volumetric superimpositions of mandibular advancement surgery. (a) Hard tissue superimposition: blue is post surgical. (b) Soft tissue superimposition.
(Image courtesy of Dolphin Imaging and Management Solutions, Chatsworth, CA; www.dolphinimaging.com.)
Discussing Treatment with the Patient
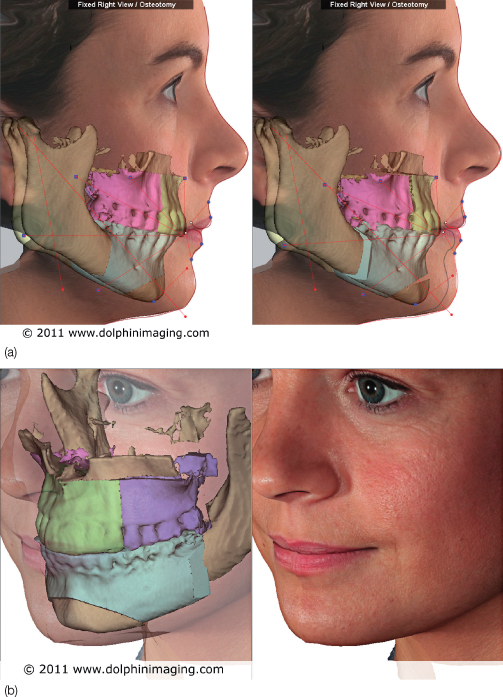
A motivated patient who understands and undertakes responsibility for his or her treatment is an asset to any practitioner. To inspire treatment compliance, a patient needs to understand the treatment procedure he or she might undergo, which is graphically possible with the aid of interactive motivational software (Table 2.5). The graphical simulation of a treatment procedure to be undertaken can aid eliciting truly informed consent (Figure 2.7). Commensurate with the fact that the human brain registers and recalls more of what is seen in comparison with inputs received through the other senses, there is evidence suggesting that these computer-based visual patient education programs enable better recall and hence positive feedback from the patient, in comparison with traditional means of patient education alone (Patel et al., 2008). Post-treatment, predicted profiles of the patient can also help in this endeavor. In fact, it is mandatory in some countries to show the software-generated post-treatment composites of varied treatment options to the patient before treatment (Figure 2.8). Previously, only 2D profile predictions were possible. However, with ‘dynamic CBCT’ technology it is now possible to generate 3D composites of predicted treatment outcomes (Figure 2.9).
Table 2.5 Patient education software
| Software | Website |
| Caesy | www.caesy.com/ |
| Optio | www.optiopublishing.com/ |
| Orasphere | www.orasphere.com/ |
| Consult Pro | www.consult-pro.com/ |
| Dolphin Aquarium | www.dolphinimaging.com |
| Orthomation | www.gactechnocenter.com |
Figure 2.7 Screenshot from a patient education software.
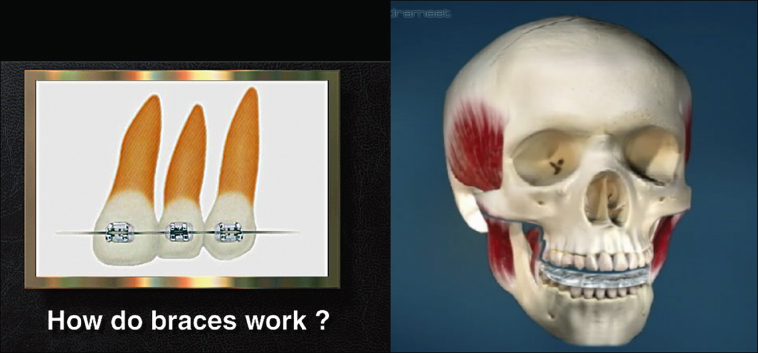
Figure 2.8 Predicted post-treatment profiles for varied treatment plans in an orthognathic patient, generated with Dolphin Imaging 10.
(Image courtesy of Dolphin Imaging and Management Solutions, Chatsworth, CA; www.dolphinimaging.com.)

Figure 2.9 3D soft tissue prediction of orthognathic surgery. (a) Mandibular osteotomy on cone-beam computed tomography (CBCT) dataset – right view. (b) Mandibular osteotomy on CBCT dataset – 45° view.
(Image courtesy of Dolphin Imaging and Management Solutions, Chatsworth, CA; www.dolphinimaging.com.)
Other Arenas of Communication
Communication Using the Internet
The internet is probably the biggest invention of the millennium and among mankind’s best, comparable with the invention of the integer zero by Indian mathematicians of yore. The internet has made communicating between geographically distant locations and time zones incredibly easy. In orthodontics, this means easy and reliable dissemination of information, electronic patient communication and appointment scheduling, patient referral to colleagues, transfer of patient records, online diagnostic aids, backup and retrieval, journal manuscript submissions, distant learning through webinars, real time interaction without physical presence of faculty, and much more (Engilman et al., 2007). Modes of communication using the internet include (Revankar and Gandedkar, 2010):
- Email (electronic mail)
- File transfer protocol (FTP)
- Hyper text transfer protocol (HTTP) file transfer
- RFB (remote frame buffer) protocol and VNC (virtual network computing)
- VoIP (voice over internet protocol)
- Video teleconferencing/videoconferencing (tele-orthodontics) (Figure 2.10).
Figure 2.10 Schematic representation showing the various methods of data transmission over the internet and their associated protocols.

Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


