This chapter discusses the main signs and symptoms of diseases affecting the orofacial region. Specific diseases are discussed in Chapter 3.
Pain is by far the most common symptom affecting the orofacial region (see Pain, page 89). The other most common signs and symptoms of orofacial disease fall into a limited number of categories, namely:
• Coloured lesions
• Bleeding
• Soreness
• White lesions
• Ulceration
• Lumps/swelling
• Tooth mobility
• Halitosis
This can be remembered by the mnemonic Could Be Someone We Usually Love To Hear.
Bleeding
Keypoints
• Bleeding may arise from wounds or from the gingival margins, or may be into the tissues – where it appears as petechiae or ecchymoses (purpura).
• Gingival bleeding is usually due to plaque-induced inflammation – gingivitis or periodontitis.
• Gingival bleeding may be aggravated by, and purpura caused by, disorders of haemostasis or drugs interfering with haemostasis.
• Purpura in the mouth is seen mainly at areas of trauma – usually at the occlusal line and junction of the hard and soft palates.
• Bleeding of the lips may be seen where there is a lip fissure, or in erythema multiforme or some types of pemphigus.
• Vascular anomalies such as telangiectasia or angiomas may bleed if traumatized.
Box 2.1 Main causes of gingival bleeding
Gingivitis/periodontitis
Platelet defects
Drugs
Trauma
Causes may include:
• Gingivitis (plaque-induced) – by far the most common cause (Figure 2.1)
Figure 2.1Gingivitis – the common cause of gingival bleeding.
• Thrombocytopenia (low blood platelet numbers)
aplastic anaemia
idiopathic (this means ‘of unknown cause’ but actually it is autoimmune) thrombocytopenic purpura
Figure 2.2Leukaemia may present with gingival bleeding, swelling and/or ulceration.
• Medications that impair haemostasis: anticoagulants, platelet aggregation inhibitors, chemotherapy, some herbal supplements
• Factitial or traumatic injury.
Oral bleeding occasionally arises from a vascular anomaly (Figure 2.3).
Figure 2.3Hereditary haemorrhagic telangiectasia may chronically bleed.
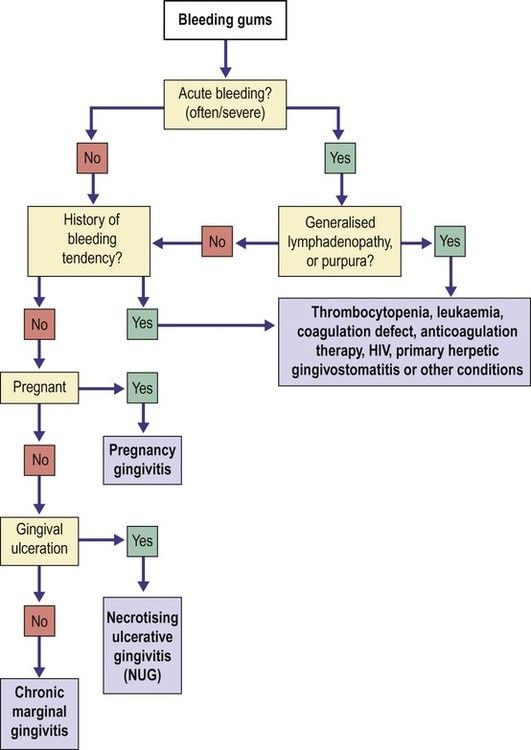
Figure 2.4Algorithm for bleeding gums diagnosis.
Burning mouth
Keypoints
• Burning mouth (glossodynia) is a common complaint.
• The cause is not usually known but it may be a nerve hypersensitivity.
• Burning mouth is not inherited.
• Burning mouth is not infectious.
• Burning mouth may occasionally be caused by some mouth conditions, dry mouth, deficiencies, diabetes or drugs.
• Burning mouth has no long-term consequences.
• Burning mouth typically affects the anterior tongue bilaterally but may affect other sites such as palate and/or lips.
• Oral examination is important to exclude organic causes of similar discomfort – such as erythema migrans (geographic tongue), candidosis, glossitis and lichen planus (Figure 2.5).
Figure 2.5Burning mouth caused by lichen planus.
• In the absence of a recognizable organic cause (Figure 2.6), the condition is termed ‘burning mouth syndrome (BMS)’ and the underlying basis may be psychogenic. These patients may also suffer taste disturbances.
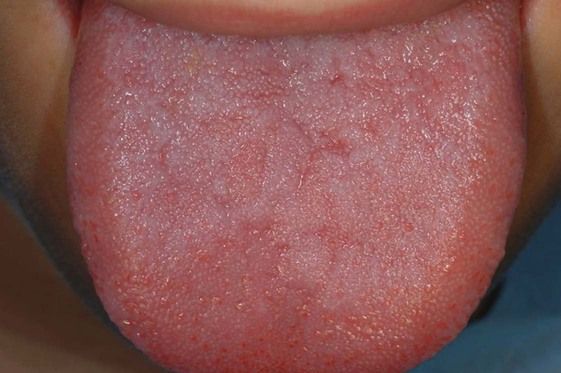
Figure 2.6Burning mouth syndrome (no lesions discernible apart from mild tongue furring).
• Blood tests, biopsy or other tests may be required.
• Burning mouth syndrome may be controlled by some psychotropic drugs or B vitamin.
Box 2.2 Main causes of burning mouth sensation
Erythema migrans
Lichen planus
Candidosis
Haematinic (iron, folate, vitamin B12) deficiency
Psychogenic
Causes may include (alphabetically):
• Allergies (including oral allergy syndrome)
• Bruxism/tongue thrusting
• Candidosis
• Dermatoses such as lichen planus
• Dry mouth and drugs such as angiotensin-converting enzyme (ACE) inhibitors, proton pump inhibitors (PPIs) and protease inhibitors (PIs)
• Erythema migrans (geographic tongue)
• Fissured tongue
• Gastric reflux, and glossitis such as caused by haematinic deficiency, such as
B complex deficiency
folate deficiency
iron deficiency
vitamin B12 deficiency
• Hormonal (endocrine) problems such as diabetes and hypothyroidism.
Once these causes are excluded, the condition is termed ‘burning mouth syndrome’, when the cause may be psychogenic, and include:
• Anxiety states
• Cancerophobia
• Depression
• Hypochondriasis.
A normal-appearing tongue may be seen in psychogenic causes, and with a burning sensation caused by deficiency states, drugs (e.g. captopril and other ACE inhibitors, proton pump inhibitors) and diabetes mellitus.
This section deals only with a normal-looking but burning tongue.
Burning mouth syndrome
Common, especially in middle-aged females.
Typical orofacial symptoms and signs: invariably persistent burning sensation with no organic disease.
Main oral sites affected: anterior tongue (occasionally palate or lip).
Aetiopathogenesis: see above.
Gender predominance: female.
Age predominance: middle age or older.
Extraoral possible lesions: often psychogenic complaints or anxiety.
Main associated conditions: few profess anxiety about (for example) cancer or sexually shared disease; some admit this on specific questioning.
Differential diagnosis: differentiate from organic causes.
Investigations: blood picture, glucose, thyroid hormone and haematinic assays to exclude organic causes; psychiatric investigation for depression.
Main diagnostic criteria: clinical.
Main treatments: treat any organic cause. Topical anaesthetics and oral distractors such as sucking on ice chips or sugarless candy, and chewing sugarless gum may be temporarily effective. Otherwise, B vitamins, topical capsaicin, psychotherapy (cognitive-behavioural therapy; CBT) or antidepressants are all occasionally helpful.
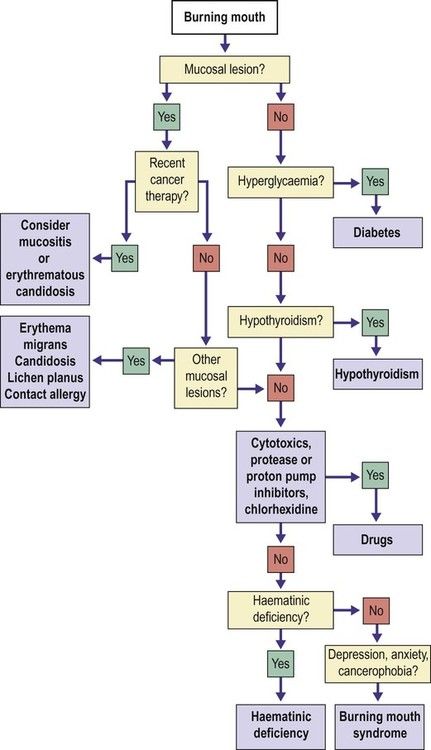
Figure 2.7Algorithm for burning mouth diagnosis.
Desquamative gingivitis
Keypoints
• Desquamative gingivitis is not a disease entity but a clinical term for persistently sore, glazed and red or ulcerated gingivae.
• The usual complaint is of persistently sore gingivae in many areas.
• Lichen planus or pemphigoid are the most common causes.
Box 2.3 Main causes of desquamative gingivitis
Pemphigoid
Lichen planus
Fairly common, it is almost exclusively a disease of middle-aged or older females.
Typical orofacial symptoms and signs: soreness or stinging, especially on eating spices or citrus foods, or taking acidic drinks. Gingivae are red and glazed (patchily or uniformly), especially labially and in several sites. Gingival margins and edentulous ridges tend to be spared. Erythema is exaggerated where oral hygiene is poor.
Main oral sites affected: facial gingivae.
Aetiopathogenesis: lichen planus or mucous membrane pemphigoid, and rarely pemphigus or other dermatoses (skin disorders) (Figures 2.8–2.10).
Figure 2.8Desquamative gingivitis: associated with lichen planus.
Figure 2.9Desquamative gingivitis: associated with lichen planus.
Figure 2.10Desquamative gingivitis: associated with pemphigoid.
Gender predominance: female.
Age predominance: adult.
Extraoral possible lesions: cutaneous, mucosal or adnexal lesions of dermatoses may be associated.
Differential diagnosis: differentiate mainly from acute candidosis, chronic marginal gingivitis, and occasionally from plasma cell gingivitis.
Investigations: biopsy with immunostaining.
Main diagnostic criteria: clinical and histology.
Main treatments: improve oral hygiene; topical corticosteroids, or systemic dapsone as appropriate. Corticosteroid creams used overnight in a polythene splint may help. Frequent dental cleanings and periodontal maintenance are important for disease control.
Dry mouth (hyposalivation and xerostomia)
Keypoints
• Xerostomia is a frequent, and the most common, salivary complaint but is not synonymous with hyposalivation.
• Xerostomia is a subjective complaint of oral dryness, and objective evidence of hyposalivation is far less common.
• Hyposalivation (hyposialia) is a reduction in saliva production – usually defined as an unstimulated whole salivary flow rate <0.1 ml/min.
• Causes of hyposalivation are often iatrogenic (doctor-induced), particularly with drugs (medications) or cancer therapy.
• Hyposalivation may also be caused by dehydration, or diseases affecting the salivary glands.
• Xerostomia has similar causes to hyposalivation and, additionally, may be psychogenic.
• Saliva helps swallowing, talking, and taste, and protects the mouth. Where saliva is reduced there is a risk of dental caries and tooth wear, halitosis, altered taste, mouth soreness and infections.
• Hyposalivation presents with obvious dryness (Figure 2.11) or frothy scant saliva (Figure 2.12), or with complaints of difficulties with speech, swallowing or denture retention; of soreness; or of complications such as candidosis, caries or sialadenitis.
Figure 2.11Dry mouth, and lobulated tongue which may follow chronic hyposalivation.
Figure 2.12Dry mouth manifesting as frothy saliva.
Box 2.4 Main causes of dry mouth sensation
Drugs
Irradiation of salivary glands
Sjögren syndrome
Psychogenic
Causes of hyposalivation may include:
• Iatrogenic
drugs (medications) with anticholinergic or sympathomimetic effects, such as tricyclic antidepressants, phenothiazines and antihistamines
irradiation of major salivary glands
cytotoxic agents, bone marrow transplantation and chronic graft-versus-host (GvHD) disease
• Non-iatrogenic
dehydration, e.g. uncontrolled diabetes, diabetes insipidus, diarrhoea and vomiting, hypercalcaemia, severe haemorrhage
salivary gland disorders
a. amyloidosis or other deposits
b. cholinergic dysautonomia
c. cystic fibrosis
d. ectodermal dysplasia
e. HCV infection
f. HIV infection
g. IgG4 syndrome
h. salivary gland aplasia
i. sarcoidosis
j. Sjögren syndrome.
Causes of xerostomia may ALSO include:
• Psychogenic states
anxiety states
bulimia nervosa
depression
hypochondriasis.
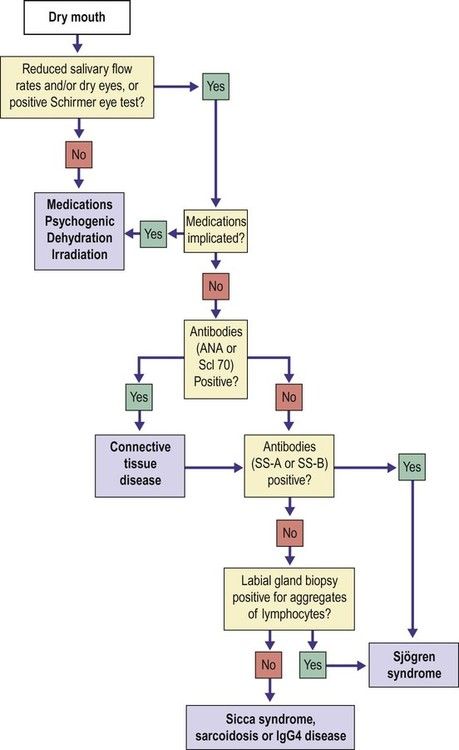
Figure 2.13Algorithm for dry mouth diagnosis.
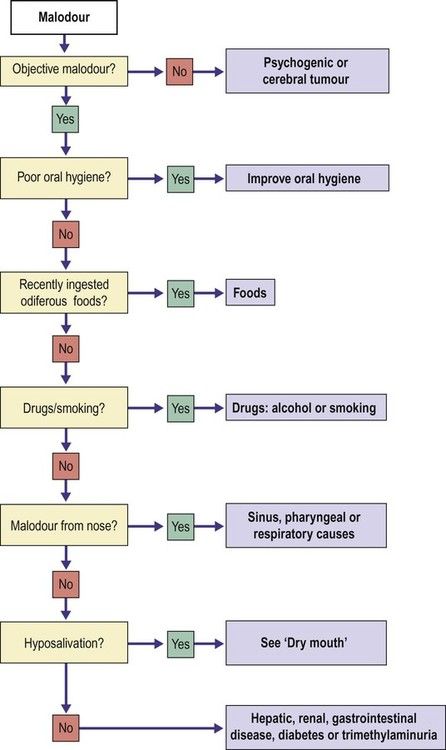
Halitosis (oral malodour)
Keypoints
• Oral malodour is a common subjective complaint but often far more obvious to the sufferer than others.
• Malodour ‘if real’ can be measured with a gas chromatography or a halimeter, but objective evidence for it by measuring volatile sulphur compounds (VSCs) in the breath by halimetry or smelling the breath is far less common.
• Malodour is common on awakening or if there is infrequent eating or starvation, and is then sometimes called ‘physiological’.
• It is usually caused by diet, habits, dental plaque or oral disease.
• Oral malodour is to be anticipated in smokers, after eating odiferous foods such as garlic or durian, or drinking excess alcohol or coffee.
• Oral malodour is common where there are oral infections.
• Malodour can sometimes be caused by sinus, nose or throat conditions.
• Oral malodour occasionally arises from metabolic disorders but it is only rarely caused by more serious disease.
• In the absence of an identifiable malodour or a defined organic cause, the complaint of malodour may be psychogenic in origin.
• It often significantly improves with oral hygiene and tongue-brushing.
• It may also be helped by:
regularly eating yoghurts or ingesting certain probiotics
finishing meals with apples, carrots or celery
chewing spearmint, tarragon, eucalyptus, rosemary, or cardamom
avoiding habits such as smoking and odiferous foods, and avoiding foods such as eggs, legumes, certain meats, fish and foods that contain choline, carnitine, nitrogen and sulphur.
Box 2.5 Main causes of halitosis (oral malodour)
Odiferous foods
Smoking
Poor oral hygiene
Causes may include:
• Starvation
• Lifestyle habits
habits
a. alcohol
b. amyl nitrites
c. solvent misuse
d. tobacco
volatile foodstuffs
a. durian
b. garlic
c. highly spiced foods
d. onions
• Drugs (see also Chapter 4): amphetamines, aztreonam, cytotoxic drugs, disulfiram, melatonin, mycophenolate sodium, nicotine lozenges, nitrates and phenothiazines
• A blister, if solitary, may be due to saliva extravasation into the tissues (mucocele).
• Blisters may be due to a subepithelial split, seen mainly in sub-epithelial immune blistering diseases (e.g. pemphigoid) (Figure 2.16).
Figure 2.16Blistering in pemphigoid.
• Blisters due to intraepithelial vesiculation are less common and caused particularly by pemphigus, and readily break to form erosions.
• Blisters rarely are caused by blood extravasation into the tissues (purpura) (Figure 2.17).
Figure 2.17Blood blisters in purpura.
Box 2.6 Main causes of oral blisters
Mucoceles
Angina bullosa haemorrhagica
Pemphigoid
Trauma (mucosal burn)
Causes may include:
• Infections
enteroviruses such as Coxsackie viruses and ECHO viruses
herpes simplex virus
herpes varicella-zoster virus
• Mucoceles
• Purpura, and angina bullosa haemorrhagica (localized oral purpura)
• Burns
• Cysts
• Skin diseases
dermatitis herpetiformis
epidermolysis bullosa (congenita and acquisita)
erythema multiforme and Stevens–Johnson syndrome
intraepidermal IgA pustulosis
lichen planus (superficial mucoceles)
linear IgA disease
pemphigoid (usually mucous membrane pemphigoid)
pemphigus (usually pemphigus vulgaris)
Sweet syndrome
• Drugs
• Paraneoplastic disorders
• Amyloidosis.
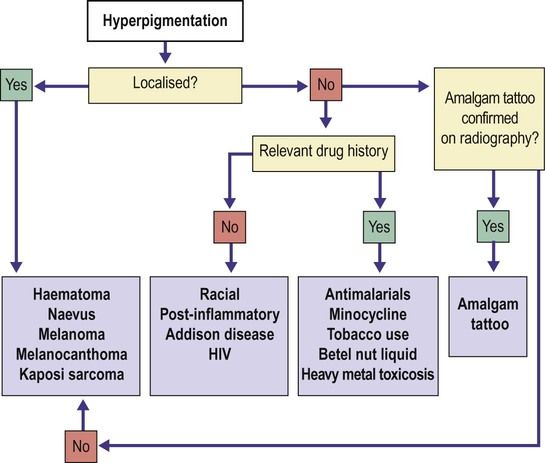
Mucosal brown and black lesions
Keypoints
• Mucosal brown and black lesions are common.
• Most mouth pigmentation is inherited. The most common cause of multiple oral brown lesions is racial or ethnic pigmentation, common in people of colour but also seen in some Caucasians and most noticeable on the facial gingivae, or other keratinized areas such as the dorsum of tongue or palate.
• Most pigmented lesions affect only the mouth but they are occasionally seen elsewhere or associated with other conditions.
• Otherwise, the cause is usually embedded amalgam, inflammation, or drugs or social habits.
• The most common cause of single oral brown lesions are naevi (Figure 2.18) or melanotic macules.
Figure 2.18Hyperpigmentation: naevus.
• Oral post-inflammatory pigmentation (pigmentary incontinence) is the common cause of multiple oral brown lesions associated with chronic inflammatory disorders (oral lichen planus and lichenoid lesions, pemphigus, or pemphigoid).
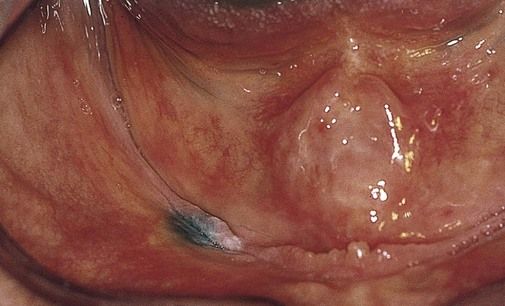
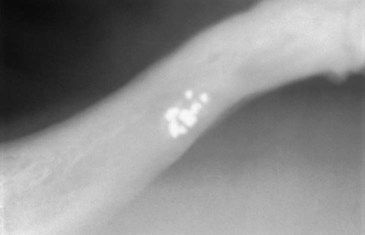
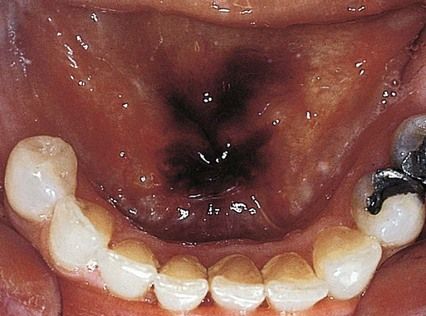
• The most common cause of single oral grey or black lesions is an amalgam tattoo, where amalgam has become embedded during restorative dental procedures (Figures 2.19, 2.20). A graphite tattoo from a pencil broken in the mouth is uncommon.
• Rare causes of brown or black lesions include drugs (Figure 2.21) or endocrinopathies such as Addisonian hypoadrenalism (Figure 2.22) and neoplasms such as malignant melanoma and Kaposi sarcoma.
Figure 2.21Hyperpigmentation: drug-induced (antimalarials, minocycline and others can be responsible).
Figure 2.22Hyperpigmentation: in hypoadrenocorticism (Addison disease).
• Solitary brown or black lesions may raise concern about the possibility of melanoma.
• Features suggestive of melanoma include (ABCDE):
Assymetry in shape
Border irregular
Colour variations or changes
Diameter (large size)
Elevation above mucosa
• Imaging, biopsy or other investigations may be indicated to differentiate the causes.
• Pigmented lesions are often removed by surgery for histopathological examination.
• There are usually no long-term consequences.
Box 2.7 Main causes of mucosal brown or black lesions
Racial
Naevus
Melanotic macule
Amalgam tattoo
Smoking
Causes may include:
• Racial
• Food/drugs
beetroot
betel nut
chlorhexidine
liquorice
tobacco
systemic drugs, such as minocycline, certain antimalarials and chemotherapeutic agents
• Hormonal
pregnancy (chloasma)
Addison disease
Albright syndrome (fibrous dysplasia)
• Others
Kaposi sarcoma
leukoplakia with pigmentary incontinence
lichen planus with pigmentary incontinence
melanoacanthoma
melanoma
melanotic macule
naevus
Peutz–Jeghers syndrome.
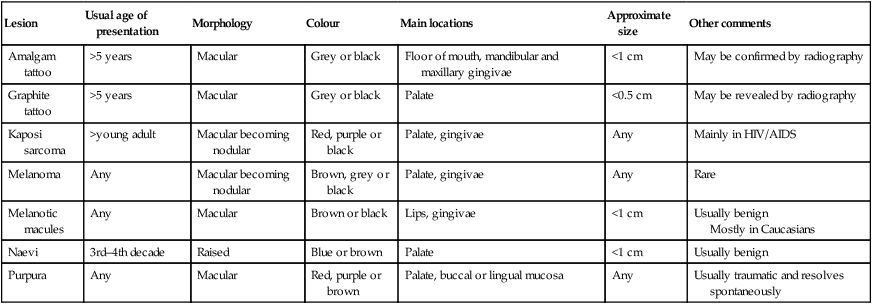
Table 2.1
Features of most important isolated hyperpigmented oral lesions
Lesion
Usual age of presentation
Morphology
Colour
Main locations
Approximate size
Other comments
Amalgam tattoo
>5 years
Macular
Grey or black
Floor of mouth, mandibular and maxillary gingivae
<1 cm
May be confirmed by radiography
Graphite tattoo
>5 years
Macular
Grey or black
Palate
<0.5 cm
May be revealed by radiography
Kaposi sarcoma
>young adult
Macular becoming nodular
Red, purple or black
Palate, gingivae
Any
Mainly in HIV/AIDS
Melanoma
Any
Macular becoming nodular
Brown, grey or black
Palate, gingivae
Any
Rare
Melanotic macules
Any
Macular
Brown or black
Lips, gingivae
<1 cm
Usually benign Mostly in Caucasians
Naevi
3rd–4th decade
Raised
Blue or brown
Palate
<1 cm
Usually benign
Purpura
Any
Macular
Red, purple or brown
Palate, buccal or lingual mucosa
Any
Usually traumatic and resolves spontaneously
Black or brown hairy tongue
Common, especially in adult men.
Typical orofacial symptoms and signs: persistent brown or black hairy appearance of tongue.
Main oral sites affected: central dorsum of tongue, mainly posteriorly but extending anteriorly.
Aetiopathogenesis: unknown. Smoking, foods such as liquorice, drugs (e.g. iron salts, chlorhexidine, bismuth) and poor oral hygiene (proliferation of chromogenic microorganisms may predispose.
Gender predominance: male.
Age predominance: adult.
Extraoral possible lesions: none.
Main associated conditions: none.
Differential diagnosis: candidosis.
Investigations: history of use of offending agents.
Main diagnostic criteria: clear-cut clinically.
Main treatments: improve oral hygiene; discontinue any drugs responsible; scrape or brush tongue (in evenings with cold water); suck dry peach stone (yes!).
Figure 2.23Algorithm for hyperpigmentation diagnosis.
Mucosal erosions (see also mucosal ulceration)
Keypoints
• Mucosal damage may lead to inflammation and/or partial-thickness loss of epithelium, both of which appear red, or to loss of most of the epithelium, which then may initially appear red but becomes covered with a yellowish fibrinous slough. Full-thickness loss of epithelium typically causes a grey or yellow lesion (an ulcer).
• Patients often present with a mix of these appearances; mucositis is the term applied to widespread oral erythema, ulceration and soreness.
• Any of the causes of mucosal blisters may result eventually in erosions.
• Any of the causes of mucosal blisters (may result eventually in erosions).
• Erosions are especially seen after burns, caused by drugs (Figure 2.24) and lichen planus (Figure 2.25).
Figure 2.24Erosion showing fibrinous slough.
Figure 2.25Erosions induced by lichenoid adverse drug reaction. Erosions are yellow: the white lesions are lichenoid.
• Mucositis, and sometimes bleeding, is common after chemo- or radio- or chemoradio-therapy, and graft-versus-host disease (GvHD). Sometimes called mucosal barrier injury, mucositis is common during the treatment of cancer but also in the conditioning prior to haematopoietic stem cell transplantation (bone marrow transplants).
Mucosal fissures or cracks
Keypoints
• Fissures are common on the dorsum of the tongue (Figure 2.26) when they are usually of genetic basis and, as there is no break in the epithelium, they are symptomless unless, as is common, there is an associated geographic tongue (erythema migrans) (Figure 2.27).
Figure 2.26Fissured tongue in a patient with Crohn disease.
Figure 2.27Fissured tongue in a patient with erythema migrans (geographic tongue).
• Fissures otherwise are often associated with epithelial breaks and are seen mainly on the lip, usually at the commissures (angular cheilitis or stomatitis), rarely elsewhere (lip fissure).
Box 2.9 Main causes of mucosal fissures
Angular stomatitis
Lip fissure
Any cause of lip swelling (e.g. Crohn disease)
Causes may include:
• Angular stomatitis
• Lip fissure
• Down syndrome
• Crohn disease or orofacial granulomatosis (OFG)
• Actinic cheilitis.
Angular stomatitis (perleche; angular cheilitis)
Common, especially in older edentulous patients who are denture-wearers.
Typical orofacial symptoms and signs: symmetrical erythematous fissures on skin of commissures (Figures 2.28, 2.29), and (very rarely) commissural leukopakia intraorally.
Figure 2.28Angular stomatitis (cheilitis) causing fissuring at commissures.
Figure 2.29Angular stomatitis causing fissuring at commissures.
Main oral sites affected: commissures, bilaterally.
Aetiopathogenesis: usually due to infection with Candida albicans. Staphylococcus aureus and/or streptococci may also be cultured from lesions. Patients may have denture-related stomatitis or other forms of intraoral candidosis. Other causes include lip incompetence, especially from orthodontic appliances, iron deficiency, hypovitaminoses (especially B), malabsorption states (e.g. Crohn disease), HIV infection and other immune defects.
Gender predominance: none.
Age predominance: older.
Extraoral possible lesions: none usually.
Main associated conditions: see aetiopathogenesis.
Differential diagnosis: see aetiopathogenesis.
Investigations: occasionally, blood picture and haematinic assays; investigations for diabetes and other immune defects; smears for fungal hyphae and bacteriological culture, if refractory.
Main diagnostic criteria: usually clear-cut.
Main treatments: Eliminate any underlying systemic predisposing factors. Treat intraoral candidal infection, in particular denture-related stomatitis. Treat angular stomatitis with topical antifungal such as miconazole or triamcinolone/nystatin combination, or fucidin or mupirocin if staphylococcal.
Fissured (cracked) lip
Typical orofacial symptoms and signs: chronic discomfort and, from time to time, some bleeding.
Main oral sites affected: typically in the lower lip (Figure 2.30), usually median.
Figure 2.30Lip fissure.
Aetiopathogenesis: a fissure may develop in the lip where a patient, typically a child, is mouth-breathing. Sun, wind, cold weather and smoking are thought to predispose. A hereditary predisposition for weakness in the first branchial arch fusion may exist. Lip fissures are also common in Down syndrome and when lips swell as, for example, in cheilitis granulomatosa and orofacial granulomatosis/Crohn disease (Figure 2.31).
Figure 2.31Fissured lip in a patient with swelling from Crohn disease.
Gender predominance: males.
Age predominance: young adult.
Extraoral possible lesions: none usually.
Main associated conditions: see aetiopathogenesis.
Differential diagnosis: see aetiopathogenesis.
Investigations: see aetiopathogenesis. If diffuse lip swelling accompanies the fissuring, biopsy is indicated.
Main diagnostic criteria: clinical. Differentiate from angular stomatitis and cheilitis glandularis (occasionally).
Main treatments: predisposing factors should be managed if possible. Bland creams or ointments (e.g. E45) may help the lesion heal spontaneously. Short-term use of low-potency topical corticosteroids with or without antifungals or antimicrobials may promote healing. If the fissure fails to heal, excision, preferably with a z-plasty, laser ablation or cryosurgery may be needed.
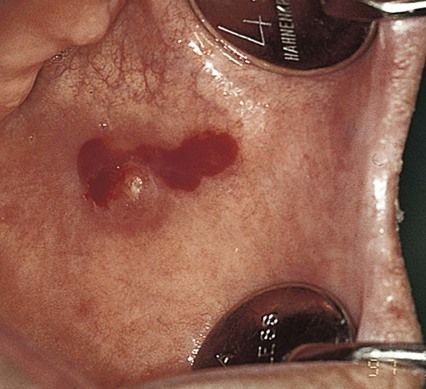
Mucosal purpura
Keypoints
• Purpura is the accumulation of blood in the mucosa, appearing usually as red or brown macules (Figure 2.32). Purpuric lesions do not blanch on pressure (cf. vascular lesions such as haemangioma, telangiectasia).
Figure 2.32Purpura.
• Petechiae are pinpoint-sized haemorrhages from small capillaries in the skin or mucous membranes. Petechia is the term given to the individual small red or red–blue spots which are about 1–5 mm in diameter and make up the rash.
• Purpura is seen mainly in areas prone to trauma, such as at the occlusal line (Figure 2.33) or junction of hard and soft palates.
Figure 2.33Purpura.
• Occasional small traumatic petechiae at the occlusal line are common in otherwise healthy patients. Otherwise, oral purpura is uncommon.
• Purpura is usually caused by trauma such as suction, but haemostatic disorders may also present in this manner, so a blood picture (including blood count and platelet count) and haemostatic function may be indicated.
Box 2.10 Main causes of oral purpura
Trauma or suction
Platelet defects
Causes may include:
• Trauma (including suction, forceful coughing or vomiting)
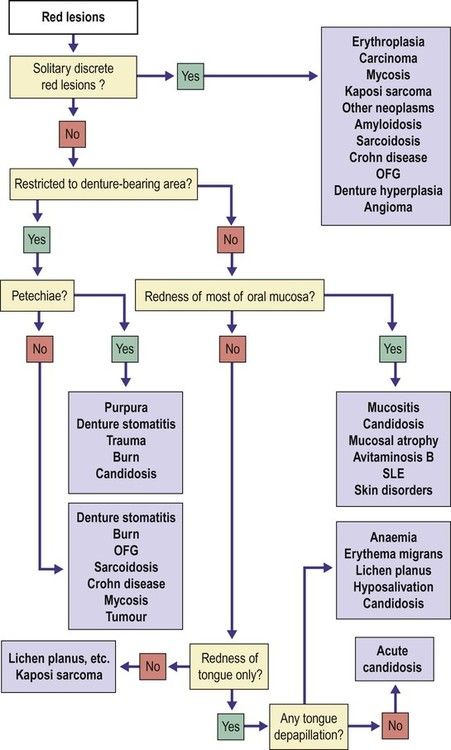
• Mucosal red lesions are usually inflammatory in origin.
• Mucosal red lesions may also be caused by epithelial loss (as in desquamative gingivitis) or atrophy as in erythroplasia (erythroplakia) – which usually represents severe epithelial dysplasia and is potentially malignant, or redness may represent frank carcinoma or other malignant neoplasms.
• Some mucosal red lesions are due to purpura or vascular anomalies such as telangiectasia or haemangiomas (the latter are more commonly purple or blue).
Mucosal ulceration or soreness (see also mucosal erosions)
Keypoints
• Soreness typically indicates a break in epithelial continuity, usually caused by erosions or ulcers.
• Ulcers can have a wide range of causes.
• Single ulcers lasting more than 3 weeks are a special concern since they may represent a malignant neoplasm (Figure 2.41) or a chronic infection such as TB, syphilis or mycoses (fungal infections). Gingival ulcers may be caused by these conditions, or acute necrotizing gingivitis (Figure 2.42).
Figure 2.41Ulceration: carcinoma presenting as an ulcerated white lesion.
Figure 2.42Ulceration: necrotizing ulcerative gingivitis (NUG). The papillae are ulcerated.
• Other persistent ulcers may have a systemic cause, such as a skin disease like lichen planus, pemphigoid or even pemphigus.
• Recurrent ulcers may represent recurrent aphthous stomatitis (aphthae) (Figures 2.43–2.45) but occasionally they manifest in systemic disease and are then termed ‘aphthous-like’ ulcers (Figure 2.46).