2
Development of the dentition
INTRODUCTION
Occlusion, in the context of dentistry, has been simply defined as the ‘contacts between teeth’ albeit between the opposing arches.1 The arrangement of the contacts between the upper and lower dentition when the teeth are in a position of maximal intercuspation is described as the static occlusion, and the pattern of the contacts that guide the movement of the mandible away from this position of maximal intercuspation is termed the dynamic occlusion.
Static occlusion can be described and classified through the assessment of incisor and molar relationships (Figures 2.1, 2.2) and the widely accepted static occlusal goals of orthodontic treatment are the six keys to occlusion described by Lawrence Andrews (Box 2.1).2 Dynamic occlusion can be assessed clinically through the careful observation of the pattern of tooth contacts when the mandible is raised into centric occlusion and is then protruded anteriorly or moved laterally.
Box 2.1 The six keys of normal occlusion
1. Molar relationship:
- The distal surface of the distobuccal cusp of the upper first permanent molar occludes with the mesial surface of the mesiobuccal cusp of the lower second permanent molar.
2. Crown angulation (mesiodistal tip):
- The gingival portion of each crown is distal to the incisal portion and symmetrically varied with each tooth in the arch.
3. Crown inclination (labiolingual or buccolingual):
- Incisor teeth with sufficient inclination to prevent overeruption
- Upper canines and premolars have similar degree of lingual inclination, with increased lingual inclination for the molars
- Lower posterior teeth from the canine to the molars have progressively increasing lingual inclination
4. No rotations of teeth
5. No spaces between teeth
6. Flat occlusal plane.
Figure 2.1 Incisor classification.
Class I: the lower incisor edges occlude with or are immediately below the cingulum plateau of the upper incisors.
Class II division 1: the lower incisor edges lie posterior to the cingulum plateau of the upper incisors, with the upper incisors being proclined or of an average inclination. The overjet is increased.
Class II division 2: the lower incisor edges lie posterior to the cingulum plateau of the upper incisors, with the upper incisors retroclined. The overjet is usually minimal but may be increased.
Class III: the lower incisor edges lie anterior to the cingulum plateau of the upper incisors, with the upper incisors. The overjet is reduced or reversed.
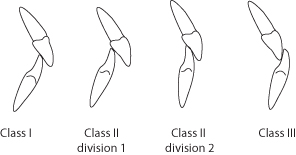
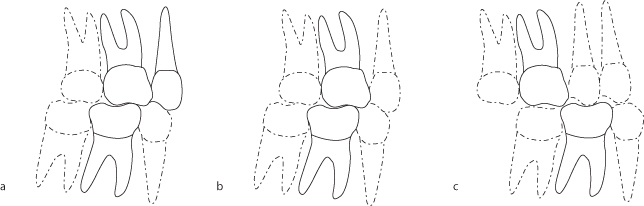
Figure 2.2a–c Molar classification.
(a) Class I: the mesiobuccal cusp of the maxillary first permanent molar lies in the buccal groove of the mandibular first permanent molar.
(b) Class II: the mesiobuccal cusp of the maxillary first permanent molar is mesial to the buccal groove of the mandibular first permanent molar.
(c) Class III: the mesiobuccal cusp of the maxillary first permanent molar is distal to the buccal groove of the mandibular first permanent molar.
Normal occlusal development is intrinsically related to the development of the dentition. The chronology of normal dental development is given in Table 2.1.
Table 2.1 The chronology of dental development
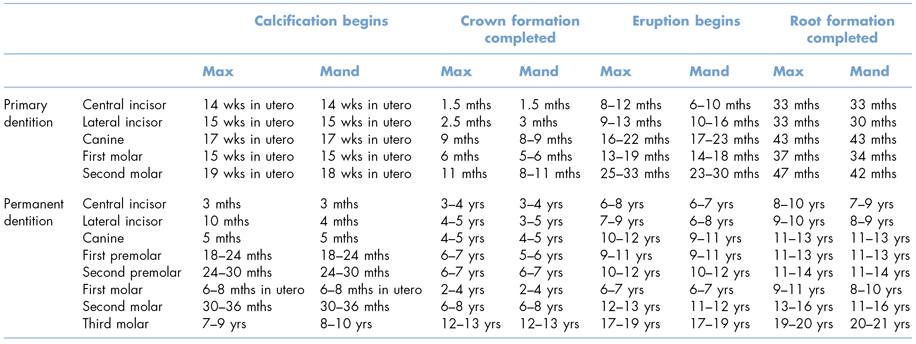
Max, maxillary; mand, mandibular; wks, weeks; mths, months; yrs, years.
Although the teeth and the contacts between the upper and lower dentition provide a means of classifying and assessing the static and dynamic occlusion, a complete assessment of a patient’s occlusion requires consideration of the periodontium, orofacial musculature, the temporomandibular joints and the underlying pattern of skeletal growth.
THE STAGES OF OCCLUSAL DEVELOPMENT
Primary Dentition (2.5 Years to 6 Years)
Intra-arch Alignment (Crowding/Spacing/Inclination of Incisors)
The fully developed primary dentition is established from the approximate age of 2.5 years. Ideally the arches are spaced, with the term ‘primate space’ or ‘anthropoid space’ being used to describe the space that is localized mesial to the upper primary canine and distal to the lower primary canine. Spacing in the primary dentition is desirable, with an excess of 6 mm of space in each arch being a favourable indication that the developing permanent dentition will be well aligned. An absence of space in the primary dentition has been associated with a 70% likelihood of crowding when the permanent dentition becomes established.3 Within the upper and lower arches the primary teeth have a typically upright appearance.4
Inter-arch Relationship (Overjet/Overbite/Molar Relationship)
The incisor relationship in the primary dentition can be indicative of the likely arrangement when the permanent dentition develops if the overjet or reverse overjet is significant. Otherwise, minimal variations in overjet measurements have little predictive value, with a normal range of overjet being between 0 and 4 mm.
The overbite is relatively increased as the primary dentition erupts and typically this gradually reduces prior to the exfoliation of the incisors as a result of attrition and some forward growth of the mandible. Oral habits such as digit or pacifier sucking are common in this age group and if these persist anterior open bites develop.
The buccal occlusion in the primary dentition is often characterized by the mesiobuccal cusp of the upper second primary molar occluding in the buccal groove of the lower second primary molar, with the distal surfaces of both the upper and lower second primary molars being in the same vertical plane. This arrangement is due to the lower second primary molar being significantly larger than the upper second primary molar and is not necessarily predictive of a developing Angle’s Class II molar relationship.
Functional Occlusion
Functional occlusion is difficult to assess in the primary dentition stage due to the changes that occur to the morphology of the teeth as a result of attrition and the underlying growth and development of the alveolar processes and the mandible and maxilla. In addition, young children can have a tendency to posture the mandible when asked to ‘bite together’ and this can complicate occlusal assessment.
While open bites that develop as a result of an ongoing oral habit will resolve if the habit is broken prior to the eruption of the permanent incisors, the lateral crossbites that can also develop as a consequence of the habit are more persistent and may be associated with a functional displacement of the mandible.
Transitional Dentition (6 Years to 12 Years)
Intra-arch Alignment (Crowding/Spacing/Inclination of Incisors)
An awareness of the typical changes that can occur during this transitional phase of dental development can enable a practitioner to reassure parents and patients that potentially unsightly appearances will improve spontaneously with further growth, and also enables appropriate referrals to be made for interceptive treatment (see Chapter 20) as required.
The lower permanent incisors develop in a lingual position relative to the primary incisors and as they erupt their alignment is typically irregular and they can appear mildly crowded. The lower incisors can then spontaneously align as space is created through three processes:
- A small increase in the tra/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


