19
Women’s Health
I. Background
In the mid-1980s, the United States Public Health Service defined women’s health as “diseases or conditions that are unique to, more prevalent or more serious in women, have distinct causes or manifest themselves differently in women, or have different outcomes or interventions.”1 This task force raised the awareness among the scientific community that women were not “smaller” men and indeed had unique health problems, including oral diseases that may require different approaches. Later in 2001, the Institute of Medicine’s Report “Exploring the biological contributions to human health: Does sex matter?”2 focused the scientific community on the need to understand the roles that sex and gender play in disease prevention and management.
This chapter addresses the unique oral health needs that women have throughout their lives. While hormonal fluctuations during puberty, menses, and menopause can affect oral health, certain diseases such as osteoporosis, burning mouth, breast cancer, and autoimmune disorders (discussed in Chapter 10), are more common in women than men and present unique challenges for dental practitioners in caring for their women patients.
Description of Disease/Condition
Puberty Onset and Menses
At puberty, girls experience an increase in estrogen and progesterone. Puberty in girls is occurring at earlier ages,3 with childhood obesity thought to be contributing to this change. Health concerns of early puberty onset include:
- potential increases in breast and uterine cancer in adult women,
- poor self-esteem,
- eating disorders,
- depression,
- earlier cigarette and alcohol use,
- earlier sexual activity.
As the age of puberty has decreased, the age of menarche has also decreased. Menstruation should occur regularly throughout a woman’s life unless she is pregnant or using contraceptives.
Pregnancy
From the first day of the woman’s last menstrual period to delivery, a full-term pregnancy is considered to be 40 weeks and is divided into three trimesters each lasting approximately 3 months. Pregnancy is increasing among older women due to technological advances. Major organogenesis occurs in the first 3 months. The facial features begin to form in the 2nd month and become recognizably human in the 3rd month. In the 3rd month, the palate closes, allowing the fetus to begin to swallow by the 4th month. By the 5th month, the mother may feel the baby kick or move and the fetal heartbeat is audible by stethoscope. While lungs are not completely formed, a baby born during the 6th month, weighing 1–1.5 lb, can often survive in a neonatal intensive care unit.
Menopause
Menopause is a normal physiological event that signals the cessation of menses. The average age of menopause is 51 years, with a range from 48 to 55 years. Perimenopause is the 3- to 5-year period before the last menstrual period occurs and signals the changes in hormone levels. Women who smoke, have never been pregnant, and live at high altitudes are more likely to have an earlier menopause.
Osteoporosis
Osteoporosis is a systemic skeletal disease characterized by low bone mass and microarchitectural deterioration of bone tissue. These changes increase bone fragility and susceptibility to fracture.
Breast Cancer
Breast cancer is the most common cancer occurring among women. The two most common forms of breast cancer are ductal and lobular, and each can be either invasive or in situ.
Interpersonal Violence against Women
Violence against women, also called “domestic violence” or “spousal abuse,” has been redefined as “intimate partner violence” (IPV). This new term recognizes that intimate partner violence occurs between two people in a close relationship, whether married or dating, men and women, and in gay and lesbian couples.4 IPV can include four types of behaviors:
- physical violence,
- sexual violence,
- threats of physical or sexual violence,
- emotional abuse.5
Pathogenesis/Etiology
Osteoporosis
| Nonmodifiable risk factors | Modifiable risk factors |
| Being female | Diet low in calcium |
| Small frame women | Sedentary lifestyle |
| Advanced age | Anorexia nervosa or bulimia |
| Family history of osteoporosis | Smoking |
| Early menopause (before age 45) | Excessive alcohol intake |
| Prolonged use of certain medications (glucocorticosteroids, anticonvulsants, excessive thyroid hormone, and certain cancer treatments) |
Breast Cancer
- The most common genetic risk factors for breast cancer are mutations in BRCA1 and/or BRCA2, affecting only 5–10% of women with breast cancer.
- Breast cancer risk is also elevated by
- having a family member (first-degree relative) with breast cancer, particularly if the family member was diagnosed at an early age;
- exposure to high levels of radiation in early life;
- prior treatment for Hodgkin’s disease.6
Epidemiology
Pregnancy
- In the United States in 2009, a little over 6 million pregnancies resulted in
- 4,130,665 live births,7
- about 1.2 million induced abortions,
- about 1 million fetal losses from miscarriage or stillbirth.
- The mean age at first birth was 25.5 years, and 41% of the births were to unmarried women.
- Approximately 500,000 babies (12.2% of the births) were preterm.7 A preterm low birth weight (LBW) baby is defined as a baby born before 37 weeks and weighing less than 2500 g (5 lb, 8 oz). Prematurity is a major risk for newborn death, chronic health problems, and developmental disabilities.
- The LBW rate (<2500 g) was 8.16%.7
- Breastfeeding for newborns increased in the United States from 2000 to 2008.8
- Early postpartum breastfeeding (0–3 months) has increased from 71% to 75% of mothers in 2000–2007.
- Mothers who breastfeed their babies at 6 months increased from 34.2% to 43.8%, from 2000–2007.
- Mothers who exclusively breastfed their babies for the first 3 months were estimated at 35.0% and for the first 6 months were 14.8% in 2008.
Oral, Transdermal, and Implanted Contraception Use
Of the 62 million women between ages 15 and 44 in 2008, 62% were using some form of contraception.9 Of these women, 35.7% or over 13 million women are using some form of oral, transdermal, or implanted contraception. Many systemic and oral side effects have been observed in women using hormonal contraception.
Osteoporosis
Approximately 30% of all postmenopausal women have osteoporosis in the United States and Europe.10 At least 40% of these women and 15–30% of men will sustain one or more fractures in their remaining lifetime. The most common fracture sites are hip, radius, and vertebral compression fractures.
Breast Cancer
Each year, around 200,000 women will be diagnosed with invasive breast cancer and about 40,000 women will die from breast cancer.6 Another 50,000 women will be diagnosed with noninvasive breast cancer. It is second to lung cancer in the number of cancer deaths in women. Although breast cancer is most common in Caucasian women, African-American women are more likely to die of breast cancer. While men are also diagnosed with breast cancer, the female-to-male ratio remains 100:1. Age and being female are the greatest risk factors for breast cancer, with breast cancer occurring more frequently in women over age 70 years.
Interpersonal Violence against Women
It is estimated that from 1 to 3 million women are battered each year by their intimate partner.11 IPV occurs along a continuum from a single episode of violence to continual battering. It is a leading cause of injury to women ages 15–44 years.
Nearly 3 in 10 women and 1 in 10 men have experienced rape, physical violence, or stalking by an intimate partner.12
Risk factors that contribute to intimate partner violence include:
- being violent or aggressive in the past;
- seeing or being a victim of violence as a child;
- using drugs or alcohol, especially drinking heavily;
- not having a job or other life events that cause stress.
 Coordination of Care between Dentist and Physician
Coordination of Care between Dentist and Physician
Critical times for the dentist and physician to work together to maintain and improve the woman’s health (and that of her child) are during pregnancy, when breast cancer occurs and requires management with chemotherapy or intravenous bisphosphonates, and when interpersonal violence is suspected. Dentists should consult with the pregnant patient’s obstetrician or other physician whenever management questions exist.
 II. Medical Management
II. Medical Management
Identification/Medical History/Physical Examination
Pregnancy
A history of pregnancies is often described by terms gravida (# of pregnancies), parida (# of deliveries after 20 weeks), and abortus (# of pregnancy losses prior to 20 weeks regardless of cause: spontaneous, elective, therapeutic abortion, or ectopic pregnancy). The sum of parity and abortus equals gravidy.
Menopause
Many women experience a variety of symptoms as a result of the hormonal changes associated with the transition through menopause. As women experience menopause, they are starting to lose bone mass and their risks for cardiovascular disease (CVD) increase as their cholesterol levels rise after menopause.
Hot flashes are the most common symptom of menopause affecting over 75% of women. These feelings of warmth throughout the body can last for about 30 seconds. Women usually experience them for 2–3 years, although some women have reported having them for up to 5 years. Night sweats can also signal menopause.
Interpersonal Violence against Women
Physical violence can result in broken bones, internal bleeding, or trauma to soft tissue and organs and even death. Trauma inflicted to the head and neck region is common.
Laboratory Testing
Pregnancy
Pregnancy tests (urine or serum) assess presence of human chorionic gonadotropin (hCG) produced by the placenta. Home urine tests can detect pregnancy as early as the day of the missed menstrual period.
Prenatal tests commonly include tests that assess for birth defects that may occur in up to 3% of pregnancies:
- Alpha-fetoprotein (AFP), a substance produced by the fetal liver. Abnormally low levels can suggest Down syndrome; abnormally high levels can suggest a fetal neural tube defect to include brain and spinal cord.
- Triple marker test: usually AFP, hCG, and unconjugated estriol.
- Other prenatal tests: tests for sexually transmitted diseases and human immunodeficiency virus, gestational diabetes screening at 24–48 weeks, blood tests for anemia and blood type, screening for immunity to various infectious diseases.
- Amniocentesis can also be used in the prenatal diagnosis of chromosomal abnormalities and fetal infections.
Osteoporosis
- Dual-energy X-ray absorptiometry (DXA) remains the most common diagnostic test for measuring bone mineral density.
Medical Treatment
Pregnancy
During pregnancy women are advised to take 400 µg folic acid supplement to prevent spina bifida; use precautions with all medications; eat a balanced diet with frequent small meals; and avoid smoking, drinking alcohol, recreational drugs, large amounts of caffeine, and artificial sweeteners.
Menopause
Hormone replacement therapy (HRT) was once fairly widely used to replace the hormones that were decreasing with menopause. Findings from the Women’s Health Initiative of increased risks for CVD, breast cancer, and stroke when taking HRT resulted in the development of new guidelines supporting the use of HRT for only a short-term basis to help alleviate the symptoms of menopause. Recent studies demonstrate that estrogens exacerbate CVD in older women with existing atherosclerosis but may be protective from CVD in younger healthier women without atherosclerosis or inflammation.13 The decision to take hormone therapy during and after menopause is based on medical history, severity of the symptoms, and potential risks and benefits of hormone administration.
Osteoporosis
Current treatment recommendations include antiresorptive agents to reduce bone resorption (and subsequently increase bone formation), leading to an increase in bone mineral density to varying degrees.
Antiresorptive agents include:
- estrogen,
- selective estrogen receptor modulators,
- bisphosphonates,
- the human monoclonal antibody to receptor activator of NFκB ligand (RANKL).
Bisphosphonates inhibit osteoclastic activity and have been shown to decrease vertebral fractures. They bind to bone mineral and have a long skeletal retention. Patients with a diagnosis of osteoporosis are also advised to take vitamin D and calcium, to maintain a proper diet, and to start or continue a program of weight-bearing exercise.
Breast Cancer
Treatment for breast cancer is determined by the stage of the tumor at the time of diagnosis, the aggressiveness of the tumor, and age of the patient.
Treatment options for breast cancer include:
- radiation to kill any additional cells to reduce the risk of recurrence;
- surgery to remove the tumor;
- chemotherapy, hormonal therapies, or biological therapies to treat systemic disease, reduce the risk of recurrence, and increase survival;
- targeted therapies are being developed based on various genetic markers found in the tumor.
These new treatments have increased the survival of breast cancer patients, and it is estimated that there are now 2.5 million survivors of breast cancer.
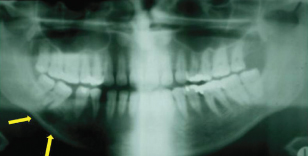
In cases of advanced breast cancer, metastases may be found in the lungs, bone, and liver. The mandible is a possible site of metastasis (see Fig. 19.1). Bone metastases can cause pain, fractures, and other bone problems. Intravenous bisphosphonates, potent inhibitors of osteoclastic activity, are the current standard of care for preventing and treating skeletal-related events for patients with advanced breast cancer with bone metastases.14
Figure 19.1 Metastatic lesion of the mandible in a 55-year-old woman with breast cancer.
 III. Dental Management
III. Dental Management
Evaluation
As with every patient, the dental evaluation of the woman begins with a thorough history. Focused key questions for the patient and physician related to the health condition are shown on the next pages.
 Key questions to ask the patient
Key questions to ask the patient
 Key questions to ask the physician
Key questions to ask the physicianDental Treatment Modifications
Puberty and Menses
Microbial changes in oral flora have been reported during puberty, attributed to responses to the sex hormones, estrogen, and progesterone, by the oral flora. Capnocytophaga species increase in incidence and proportion, and Prevotella intermedia has the ability to substitute estrogen and progesterone for vitamin K, an essential growth factor. These organisms, along with increased blood flow to gingival tissues as a result of hormonal changes, have been implicated in the increased gingivitis and gingival bleeding observed during puberty when oral home care is poor.
Oral changes may occur during menses and vary considerably among women.
Dental Treatment Considerations
- Early oral hygiene education.
- Scaling and improved daily oral hygiene care for mild cases of gingivitis.
- More aggressive care and more frequent recalls for severe cases of gingivitis until the condition improves or resolves.
Pregnancy
Pregnancy is a stressor to oral health. It is not uncommon to encounter a woman today who still believes that you “lose a tooth for each pregnancy.” This misconception arose from the belief that the calcium needed for the developing fetal bones was available from the teeth. The calcium in the teeth is in a stable crystalline form and is not bioavailable. Blood calcium serves as the reservoir for calcium required for fetal development.
- Dental Caries
- The relationship between caries and pregnancy is not clearly defined. The relationship of increased parity to increased dental caries may relate both to biological and sociodemographic factors.15
- If the pregnant woman is craving cariogenic foods, her risk for caries may increase.
- Based on clinical trials showing no difference in early childhood caries outcome in the offspring,16 current practice does not recommend the use of prenatal fluoride for pregnant women.
- Periodontal Diseases
- Gingivitis is the most common oral condition, occurring in 60–75% of pregnant women.
- It can range from mild inflammation to severe gingival overgrowth; be generalized or localized; occur at any time during pregnancy. The increase in hormones exaggerates the gum tissue’s response to bacterial plaque. The gingival tissue is usually red and swollen, and bleeds easily. It often occurs in the anterior part of the mouth.
- A “pregnancy tumor” or pyogenic granuloma (see Fig. 19.2) can occur in up to 10% of pregnant women. Pregnancy granulomas may be excised prior to delivery if the tis/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


