Chapter 19 Conventional bridges
Conventional bridges or implants?
The advent of implant supported restorations has, to some extent, reduced the need for conventionally prepared bridges. However, the financial cost of implant retained restorations is higher than conventional bridges, due to the additional cost of the implant components. Others claim that there is little long-term difference due to the biological impact conventional bridge preparation has to abutment teeth and the potential need for further treatment. Despite the cost, implants require surgical procedures demanding sufficient quantity and quality of bone (see Chapter 17). These issues, together with the status of the remaining dentition, may influence the choice as to how to replace teeth and, as such, conventional bridges remain useful options in prosthodontics.
Terminology
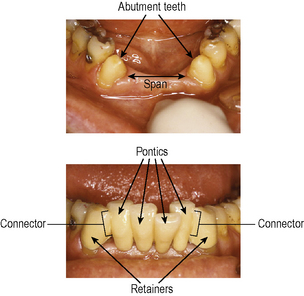
The terminology used for bridges or fixed partial prostheses/dentures includes the following (Figure 19.1):
Conventional versus resin retained bridges
Occasionally the shape and/or appearance of the abutment teeth may require alteration and this can be incorporated into the bridge design. The patient seen in Figure 19.2 has congenitally missing upper lateral incisor teeth. The image shows that the left central incisor is discoloured and the composite veneer used to mask this has not been successful. Preparation of the central incisor for a metal–ceramic retainer on a cantilever designed bridge will improve the appearance of the tooth and provide support for the pontic.

Preparation of teeth for full coverage crowns also allows some control over distribution of space and size of teeth. For example, Figure 19.3 shows the upper right central incisor tooth is missing, but the span (mesio-distal space) is greater than the mesio-distal width of the contralateral incisor crown. Removal of the crowns on the adjacent teeth will allow the retainers to be made with a slightly larger mesio-distal width and hide the space and tooth size discrepancy. In a similar way, tilted or angled abutment teeth can be aligned to some degree to improve the appearance in the anterior region.

Bridges with more than one pontic require a fixed–fixed or fixed–movable design rather than a cantilever design. This allows support and retention to be gained from the abutment teeth either side of the pontic. When the abutment teeth are minimally restored, minimal preparation (resin retained) bridges can be considered, but longer span bridges demand greater retention from the abutment teeth and this can only be achieved from conventional preparations. The risk of decementation of minimally prepared (resin retained) bridges becomes too great once the span increases by more than one pontic. For example, the edentulous span for the elderly patient seen in Figure 19.1 is too long for a minimally prepared (resin retained) bridge and the abutment teeth have been prepared for metal–ceramic retainers to optimize retention. The age of the patient, the mild wear on the teeth and the exposed root surface will ensure sufficient secondary and tertiary dentine formation to reduce potential pulpal trauma during tooth preparation.
Optimizing aesthetics

When the space is too large compared to the contralateral tooth (Figure 19.3):
Bridge design
Cantilever bridges
Cantilever bridges are designed so that the pontic is attached to a retainer on one side only, and are therefore usually more conservative of tooth tissue, especially if the other potential abutment tooth is minimally restored or sound. Retrievability is also easier if cantilever bridge designs are used. Consider the patient in Figure 19.4: three separate cantilever bridges have been placed instead of a fixed–fixed bridge design (see next section). Thus, if one abutment tooth fails due to secondary caries for example, only one tooth and bridge need replacing, so reducing the complexity of treatment and cost to the patient. Longer span bridges, particularly those where the pontic or retainers are involved in lateral guidance, increase the occlusal forces on the bridge and potentially reduce their survival. Historically, attempts were made to overcome this problem by using two abutment teeth. A typical example was a bridge to replace an upper canine; two premolar teeth were prepared for three-quarter crown retainers and linked to form a three unit cantilever bridge with a mesial pontic to replace the canine. This should be avoided as maintaining good oral hygiene beneath linked retainers is difficult, increasing the risk of caries and periodontal disease.
Occasionally cantilevered pontics can be used in conjunction with more extensive bridge designs. The patient seen in Figure 19.5 has a four unit fixed–fixed conventional bridge with the upper second premolar and second molar teeth used as abutments and the upper first premolar and molar teeth as pontics. The second premolar abutment has a pontic on either side and is referred to as a pier abutment, the first premolar pontic being cantilevered off the bridge.

Fixed–fixed bridges
A fixed–fixed bridge has a pontic rigidly connected to retainers on both sides and has one path of insertion. The vertical orientation of both abutment teeth needs to be reasonably well aligned and parallel to each other (Figures 19.1, 19.5 and 19.6) to avoid undercuts. Most fixed–fixed bridges have full coverage crown retainers: if one abutment tooth had a relatively small restoration and an inlay was use as a retainer, occlusal contact on the tooth would lead to shear stresses being generated in the cement lute, with eventual debonding and risk of secondary caries (Figure 19.7). In theory, the use of a movable joint withinthe inlay would allow independent micromovement of that abutment tooth in an axial direction in />
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


