The oral medicine and oral surgery–endo interface
Differential diagnosis of orofacial lumps and bumps
When examining any lesion whether obviously related to a tooth or adjacent to a tooth, a standard description (Table 17.1) is undertaken in order to establish diagnosis or enable differential diagnosis.
Soft tissue swellings
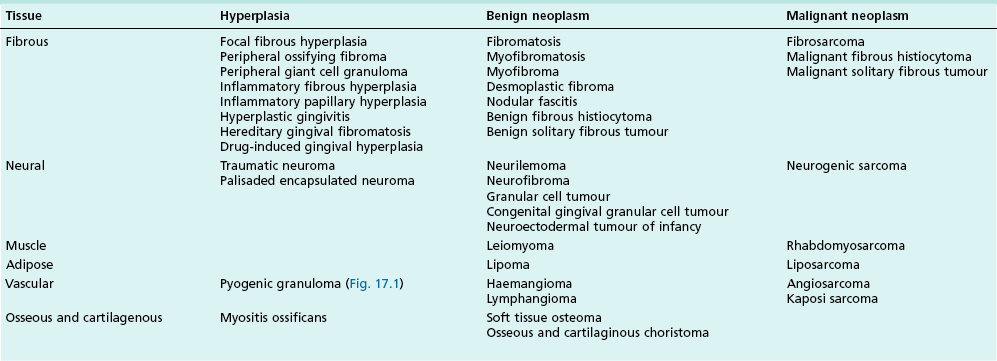
Various tissue elements may give rise to soft tissue lesions that are hyperplasias or neoplasms, either benign or malignant. Connective tissue lesions presenting as swellings are shown in Table 17.2.

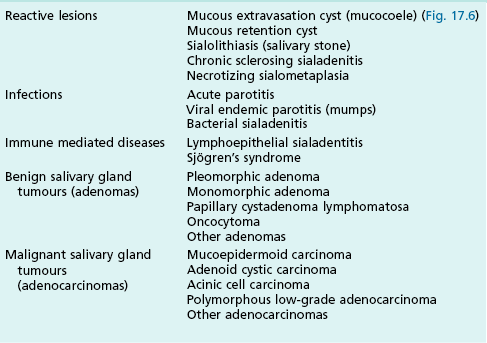
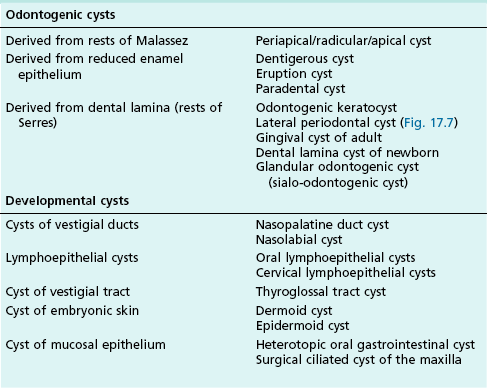
Other tissues involved in orofacial soft tissue swellings may be epithelial (Table 17.3) in origin or related to the salivary glands (Table 17.4), haematological (Table 17.5) tissues or cysts (Table 17.6).
Table 17.3
Soft tissue swellings derived from epithelial tissue
| Benign epithelial lesions | Squamous papilloma, epithelial polyp (Fig. 17.2) Keratocanthoma, verrucous papilloma (Fig. 17.3a) Leaflet papilloma (Fig. 17.3b,c) |
| Benign pigmented lesions | Melanotic macule, naevi, seborrheic keratosis, actinic lentigo, Peutz–Jeghers syndrome, melasma, acanthosis nigricans |
| Leukoplakia | |
| Epithelial hyperplasia | Hyperkeratosis, acanthosis, nicotinic stomatitis, proliferative verrucous leukoplakia |
| Epithelial atrophy | Oral submucous fibrosis |
| Epithelial dysplasia | Carcinoma in situ |
| Erythroplakia | |
| Malignant epithelial neoplasms | Squamous cell carcinoma (Fig. 17.4), verrucous carcinoma (Fig. 17.5) |
| Melanoma |










Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


