Regressive Alterations of Teeth
➧. Classification of Regressive Alterations Affecting Teeth
Erosion Associated with Common Food Substances
Erosion Associated with Medications
Erosion Related to Deleterious Habits
Occupation-related Dental Erosion
Occupations Associated with Exposure to Acidic Fumes Abfraction





Tooth Surface Loss
Mair in 1992 described the term ‘non-carious cervical lesions’ or ‘cervical wear’ to refer to loss of tooth substance at the cementoenamel junction. These non-carious cervical lesions include cervical erosion, abrasion and abfraction. Clinical studies by Kitchin (1941) have shown that cervical wear lesions are often situated on the vestibular surfaces of teeth, seldom on lingual surfaces and rarely on proximal surfaces. These are also more pronounced on incisors, canines, and premolars and more prevalent in the maxilla than in the mandible.
Attrition
Attrition involves occlusal/proximal surfaces of teeth. It occurs more frequently in males than in females due to greater masticatory forces. It appears as a small polished facet on cusp tips and causes flattening of incisal edges in case of anterior teeth (Figure 1). The wear will lead to exposure of the dentin causing hypersensitivity. The worn surfaces of opposing teeth occlude together very accurately. Wear of the proximal surface causes decrease of arch length. Lambrechts et al (1989) reported that the rate of attrition is about 29 μm/year for molars and 15 μm/year for premolars.

Figure 1 Attrition of the mandibular posterior teeth in a patient with the habit of tobacco chewing. Courtesy: Department of Oral Medicine and Radiology, MCODS, Mangalore
Clinical significance
Attrition of teeth leads to esthetic and functional disturbances. Dentinal hypersensitivity is usually the most common complaint. Severe attrition leads to pulpal exposure (Figure 2), non-vital teeth and periapical pathology. The razor sharp cuspal or incisal edges of teeth may cause traumatic ulcers.
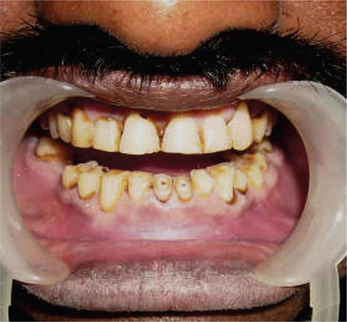
Figure 2 Severe attrition of the mandibular incisors causing exposure of the pulp. Photograph also showing attrition of incisal edges of maxillary central incisors. Courtesy: Department of Oral Medicine and Radiology, MCODS, Mangalore
It is often believed that generalized attrition will also result in a reduction in occlusal face height (vertical dimension of occlusion). However, it has been often noticed that in spite of the extensive loss of tooth surface the resting facial height appears to remain unaltered primarily because of dentoalveolar compensation. Bruxism-associated attrition may be associated with temporomandibular dysfunction.
Abrasion
Clinical features
It is seen frequently on exposed root surfaces and in cervical regions of labial and buccal surfaces due to overzealous toothbrushing in horizontal manner. Maxillary teeth are involved more than mandibular teeth, and left side is affected commonly in case of right-handed persons and vice versa. It appears as a V-shaped or a wedge-shaped ditch on the root side of the cementoenamel junction in teeth with some gingival recession (Figure 3). The exposed dentin appears highly polished (Figure 4). Improper use of dental floss and tooth picks may also produce such lesions on the exposed proximal root surfaces.

Figure 3 Cervical abrasion with respect to the upper molar along with gingival recession. Courtesy: Department of Oral Medicine and Radiology, MCODS, Mangalore

Radiographic features
However, abrasive lesions caused by dental floss are usually slender half-moon-shaped radiolucent areas in the proximal regions of the neck of the teeth. Owing to the normal flossing pattern, the distal surface of teeth exhibit relatively deeper radiolucent areas compared to the mesial surfaces of teeth. Pulp chambers may be obliterated.
Erosion (Corrosion)
Clinical features
Clinically, erosions appear as wide, polished and smooth areas on the enamel approximating the cervical margin of the tooth (Figure 5). The erosive areas are almost always shallow and exhibit ‘scooped-out’ architecture. The common teeth to be affected by erosion are the anterior teeth.

Causes for Corrosion (Flowchart 1)

1. Endogenous/intrinsic causes
Frequent episodes of vomiting as seen in pregnancy, acid reflux or regurgitation, anorexia nervosa and bulimia cause corrosion of teeth. Bodecker (1945) showed that the gingival crevicular fluid is acidic and may cause corrosion when in contact with the cervical regions of the teeth.
Erosion of the lingual or palatal surface of teeth due to regurgitation of the acidic contents of the stomach, aggravated by the circular movement of the tongue is termed perimolysis (Figure 6).

Figure 6 Erosive lesions on the palatal surface of the maxillary anterior teeth. Courtesy: Department of Oral Medicine and Radiology, MCODS, Mangalore
Pregnancy and dental erosion
Laine (2002) described the effect of pregnancy on periodontal and dental health. He reported that the tooth environment is significantly altered in pregnancy. He stated that a number of salivary cariogenic microorganisms may increase in pregnancy, along with decrease in salivary pH and buffer effect.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


