CHAPTER 17
Nasal Fractures
Hani F. Braidy and Vincent B. Ziccardi
Department of Oral and Maxillofacial Surgery, New Jersey Dental School, University of Medicine and Dentistry of New Jersey, Newark, New Jersey, USA
Reduction of displaced nasal bones and associated nasal structures.
Indications for Closed Reduction of Nasoseptal Fractures
- Displaced fractures with cosmetic deformity
- Fractures with resulting nasal obstruction
- Severely comminuted fractures
Indications for Open Reduction of Nasoseptal Fractures
- Severely displaced fractures
- Severe displacement of the nasal cartilage complex
- Concomitant extensive lacerations
- Remaining deformity after closed reduction
Contraindications
- Cerebrospinal fluid (CSF) rhinorrhea
- Old fractures (>4 weeks)
Anatomy
- The pyramidal-shaped nasal bone complex includes the paired nasal bones that articulate with the nasal processes of the frontal bone and the maxilla.
- The nasal septum consists of the following structures: crest of the maxillary and palatine bone, perpendicular plate of the ethmoid, vomer, and quadrangular cartilage.
- The nose has an extensive blood supply derived from the internal carotid (anterior ethmoidal artery and branches) and external carotid (greater palatine, superior labial, sphenopalatine, and angular arteries) artery.
- Anterior epistaxis typically involves a complex of vessels known as Little’s area or Kiesselbach’s plexus (the confluence of the anterior ethmoidal, greater palatine, superior labial, and sphenopalatine arteries).
Closed Nasoseptal Reduction Technique
- Depending on the degree of displacement, patients are treated with local, intravenous, or general anesthesia. With general anesthesia, the patient is orally intubated, and the nasal cavities and maxillofacial skeleton are prepped and draped.
- The nasal complex is anesthetized with local anesthetic containing a vasoconstrictor injected along the nasal floor, lateral nasal walls, septum, turbinates, and nasal bridge. Infraorbital, infratrochlear, and supratrochlear bilateral blocks are performed as well.
-
Intranasal packings containing oxymetazolin (or 4% cocaine) are placed within the bilateral nasal cavities (see Figure 17.4 in Case Report 17.1).
- A sterile marking pen is used to mark the location of the medial canthal tendons (MCT) and the midline.
-
The distance between the nostril and the bridge of the nose (nasofrontal suture) is estimated by placing the Goldman elevator against the external surface of the nose with its tip next to the medial canthus (Figure 17.5, Case Report 17.1). A fingertip from the dominant hand is placed on the instrument to “mark” that distance. The instrument is introduced into the nose and directed superiorly and laterally to reduce the displaced nasal bones, while the fingers of the nondominant hand provide counterpressure externally and aid in molding the nasal bones (Figure 17.1; and see Figure 17.6, Case Report 17.1).
- An Asch forceps is then used to reduce the nasal septum over the maxillary crest (Figure 17.7, Case Report 17.1). If the nasal septum cannot be reduced with the Asch forceps alone, a septoplasty can be performed with a Killian or hemi-transfixion incision with mucoperichondrial flap elevation.
-
The nose is reexamined with a nasal speculum to view the position of the septum and to evaluate the nasal passages for obstruction and septal hematoma formation. Doyle splints are placed if septal hematoma evacuation has been performed or if tears are present within the nasal mucosa to minimize synechiae formation (Figure 17.9, Case Report 17.1). Doyle splits are impregnated with triple antibiotic ointment, placed within the nasal passages, and secured to the membranous septum with a 3-0 silk suture (Figure 17.10, Case Report 17.1).
-
Steri-strips are placed over the nasal bridge (Figure 17.11, Case Report 17.1), and an Aquaplast thermoplastic nasal splint is heated, trimmed, and applied to the nasal dorsum (Figure 17.12, Case Report 17.1).
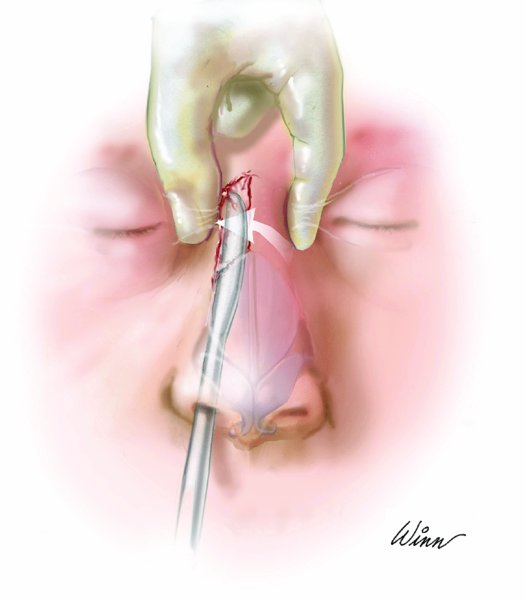
Figure 17.1. The nasal fracture is reduced with a lateral and superior rotation of the reduction forcep.
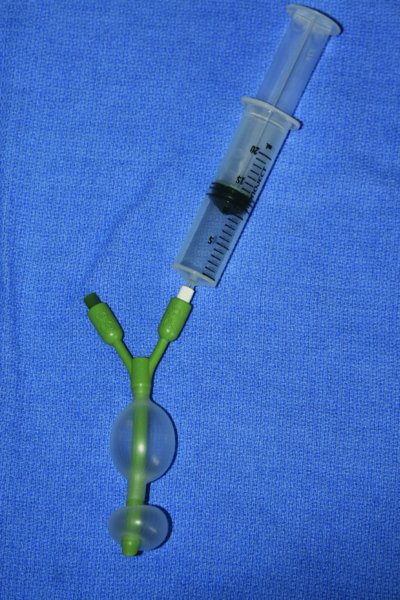
Figure 17.2. Epistat nasal catheter capable of placing anterior, posterior, or combined nasal pressure to arrest epistaxis.

Figure 17.3. Gross nasal and septal deformity.

Figure 17.4. Oxymetazolin pads placed within the nasal cavities for hemostasis.


