Malocclusion after Orthodontics and Orthognathic Surgery
Prevention and Treatment Pitfalls
Sagittal Split Ramus Osteotomies of the Mandible: Skeletal Stability and Relapse
Immediate (Early) Malocclusion after Sagittal Split Ramus Osteotomies
An immediate (early) malocclusion that is recognized either intraoperatively or soon after surgery (i.e., during the first several days or weeks afterward) will occur after sagittal split ramus osteotomies of the mandible unless each of the following intraoperative conditions is met* (Figs. 17-1 through 17-4):
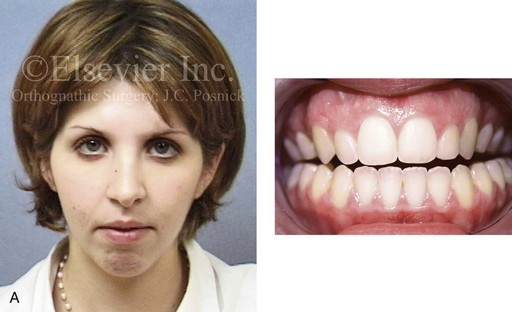
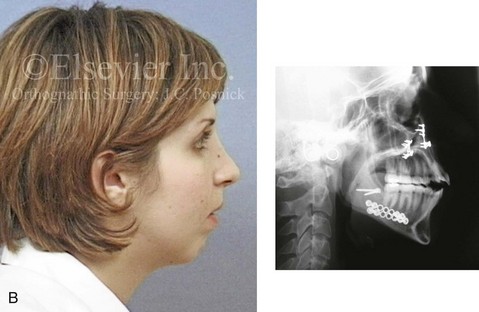

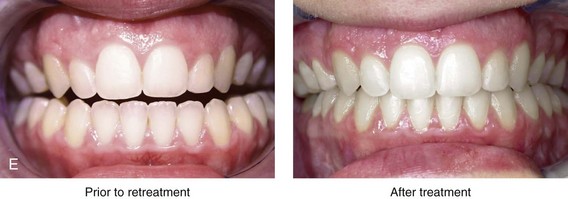
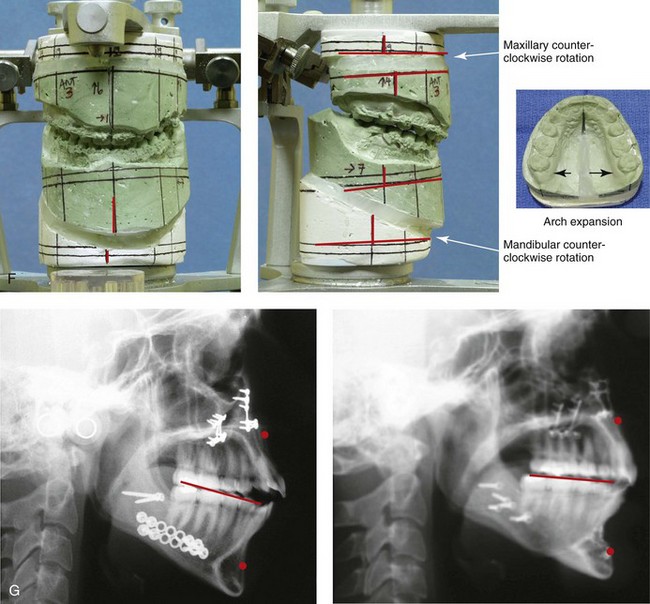
Figure 17-1 A woman in her late 20s was referred by her orthodontist for surgical evaluation. She suffered with masticatory muscle discomfort while chewing and had a jaw deformity, malocclusion, and a lifelong history of obstructed nasal breathing. A long face Class II growth pattern was evident from her childhood onward. She had undergone attempted orthodontic growth modification and then a camouflage approach, without success. She then underwent orthodontics (including upper bicuspid extractions) and surgery at another institution; this included a Le Fort I osteotomy and bilateral ramus osteotomies. Analysis confirmed both inadequate positioning of the jaws at the time of operation and then dental relapse of the maxillary arch form over time. When she presented to this surgeon, her clinical problems included the following:

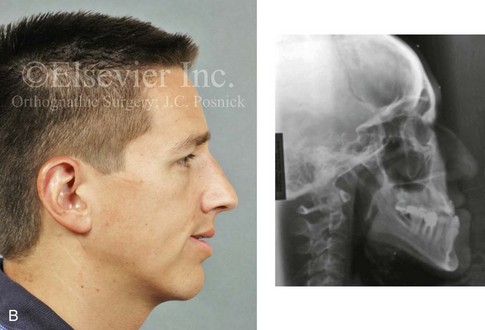


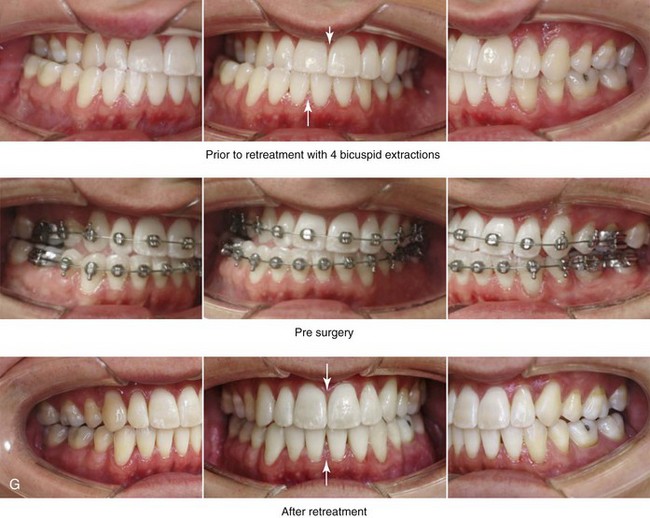
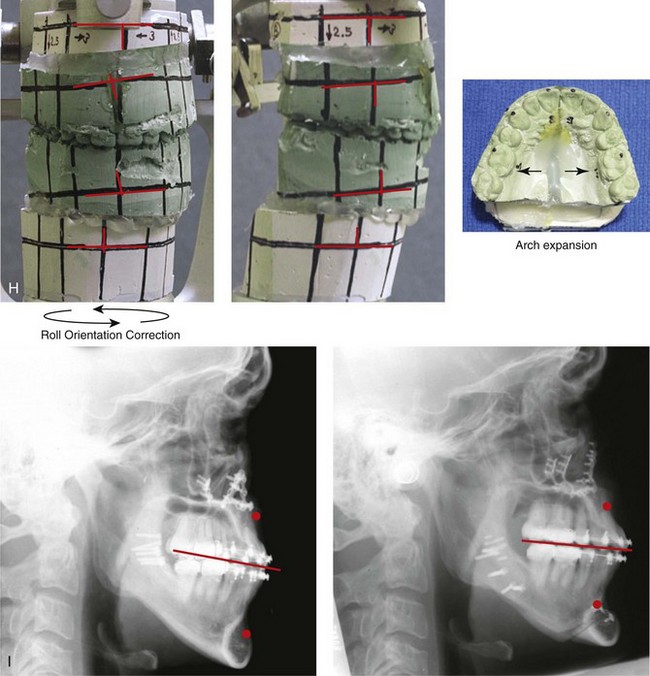
Figure 17-2 A man with a developmental jaw deformity that was characterized as an asymmetric mandibular excess growth pattern (i.e., hemimandibular elongation) presented for treatment. His orthodontist originally attempted growth modification followed by orthodontic camouflage that included four bicuspid extractions, without success. When he was 19 years old, the patient underwent further orthodontics and a surgical approach at another institution. His jaw surgery at the time included maxillary Le Fort I osteotomy and bilateral vertical oblique ramus osteotomies. An initial satisfactory surgical result was not achieved, and further orthodontic camouflage was attempted. During ongoing orthodontic treatment, alveolar bone loss and gingival recession occurred along the buccal aspect of the posterior maxillary dentition and the labial aspect of the anterior mandibular dentition. At the time of referral to this surgeon, the patient was 35 years old; thus, it had been 16 years since his suboptimal treatment. Evaluations were arranged with a periodontist; an orthodontist; a speech therapist; and an ear, nose, and throat specialist. After periodontal treatment, orthodontic decompensation was carried out in preparation for reconstruction. The patient’s surgery included maxillary Le Fort I osteotomy in segments (cant correction, transverse expansion, and minimal horizontal advancement); sagittal split ramus osteotomies (asymmetry correction and minimal horizontal advancement); osseous genioplasty (vertical reduction and horizontal advancement); and septoplasty and inferior turbinate reduction. A, Frontal and occlusal views before retreatment. B, Current profile view shown next to a lateral cephalometric radiograph taken before original surgery, when the patient was 19 years old. C, Frontal views in repose before and after retreatment. D, Frontal views with smile before and after retreatment. E, Oblique facial views before and after retreatment. F, Profile views before and after retreatment. G, Occlusal views before orthodontic retreatment, with orthodontic decompensation in progress, and after retreatment. H, Articulated dental casts after analytic model planning. I, Lateral cephalometric radiographs after first surgery and then after retreatment.
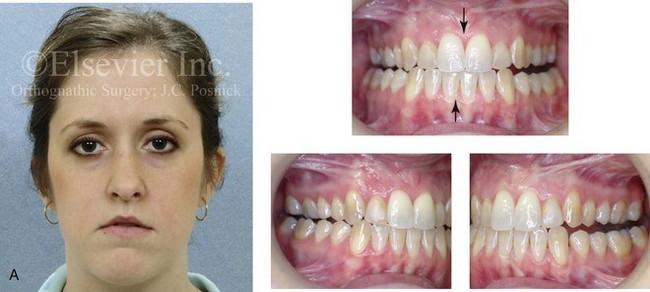

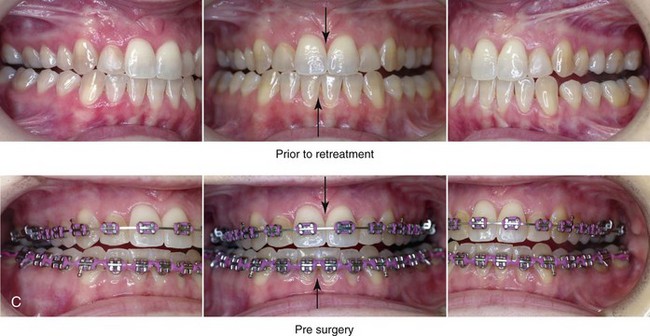
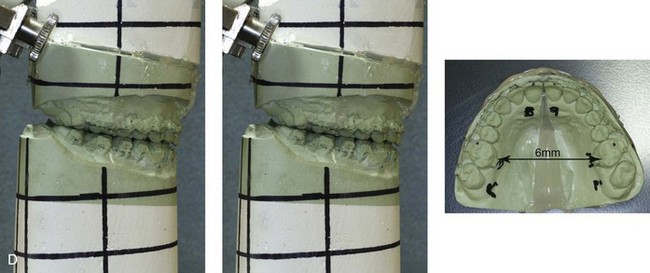

Figure 17-3 A 28-year-old woman was referred by her orthodontist for the evaluation of residual malocclusion and facial asymmetry. Eight years earlier, the patient had presented with an asymmetric mandibular excess growth pattern and underwent a combined orthodontic and surgical approach at another institution. The surgery included maxillary Le Fort I osteotomy (three segments) with iliac interpositional grafting in combination with bilateral sagittal split ramus osteotomies. Immediately after surgery, the occlusion that had been achieved was recognized to be unsatisfactory. The patient was taken back to the operating room 1 week later for the removal of the fixation of the right ramus of the mandible, the adjustment of the occlusion, and the reapplication of fixation. The occlusion remained unsatisfactory. Six months later, the patient was taken back to the operating room again, where she underwent a left vertical oblique ramus osteotomy without fixation followed by 6 weeks of intermaxillary fixation. Over the long term, the occlusion remained unsatisfactory, and the patient also had a minor degree of facial asymmetry as seen in the frontal view. At the time of referral to this surgeon, the patient stated that she hoped for the correction of the occlusion and an improvement in her current lip asymmetry. The decision was made to not operate on the mandible again. Options to improve the occlusion included maxillary Le Fort I osteotomy in segments versus surgically assisted rapid palatal expansion. Segmental maxillary surgery with immediate repositioning and interpositional grafting was carried out. The occlusion was maintained with a prefabricated acrylic splint for 6 weeks, which was followed by the immediate placement of a transpalatal arch. A, Frontal facial and occlusal views before retreatment. B, Profile facial view and lateral cephalometric radiograph before retreatment. C, Occlusal views before retreatment and preoperatively with orthodontic appliances in place. D, Articulated dental casts that indicate surgical planning. E, Demonstration of the use of the maxillary surgical model to construct a transpalatal arch wire for immediate placement at the time of splint removal (i.e., 5 weeks after surgery). The roof of the patient’s mouth is shown with the transpalatal wire in place in accordance with the surgical model. The use of orthodontic mechanics for 6 months to actively maintain the arch width achieved at operation is useful to limit a tendency toward relapse. It is also important to limit any orthodontic mechanics that may position the teeth outside of the alveolar housing, because this situation will be prone to long-term dental relapse.
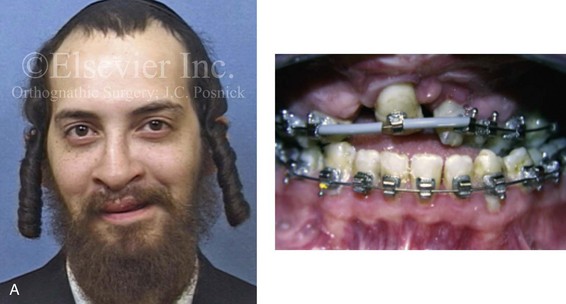
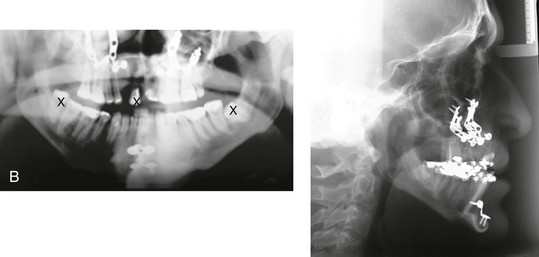
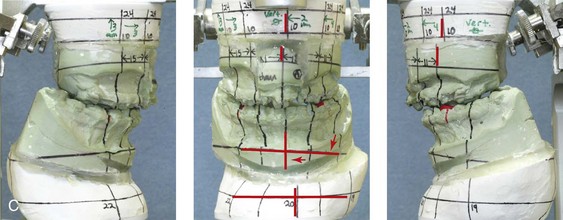


Figure 17-4 A 21-year-old man who was born with bilateral cleft lip and palate arrived for surgical evaluation. He had undergone suboptimal orthognathic surgery (Le Fort I osteotomy and osseous genioplasty) at another institution 4 years earlier. The history, physical examination, and radiographs suggested a combination of both unfavorable initial surgical healing and late dental relapse. The patient was referred to this surgeon and underwent a comprehensive surgical and dental rehabilitative approach. After periodontal evaluation and treatment, orthodontic decompensation was undertaken. The patient’s surgery included maxillary Le Fort I osteotomy in three segments with differential repositioning (cant correction, closing down of cleft dental gap, closure of fistula, horizontal advancement, counterclockwise rotation, and vertical adjustment); bilateral sagittal split ramus osteotomies (asymmetry correction); and septoplasty and inferior turbinate reduction. This was followed by planned prosthetic rehabilitation of the maxillary and mandibular arches and ongoing periodontal surveillance. A, Frontal and occlusal views at the time of surgical evaluation (i.e., 4 years after the suboptimal orthognathic procedures at another institution). B, Cephalometric and Panorex radiographs at the time of surgical evaluation. C, Articulated dental casts that indicate analytic model planning. D, Frontal views with smile before and after retreatment including dental rehabilitation. E, Occlusal views before and after retreatment including dental rehabilitation.
1. The proximal segment is successfully split from the distal mandible (i.e., no “bad” split) on each side (right and left).
2. The distal mandible is placed in the preferred occlusion and tightly held in intermaxillary fixation (IMF). Unless the natural occlusion between the upper and lower teeth is precise (i.e., without centric relation–centric occlusion slides), the IMF should be maintained with the use of an accurate prefabricated acrylic splint.
3. Each proximal segment is positioned with the condyle seated in the terminal hinge position. Each proximal segment is then secured to the distal segment with the use of either passively placed bicortical screws or monocortical screws and plates. This is accomplished without torquing or overseating the proximal segment. The following conditions should be present:
• Adequate bone contact between the proximal and distal segments, without compression or torquing
• Appropriate alignment of the proximal and distal segments to limit the rotation or torquing of each proximal segment.
4. With the release of IMF, the mandible is put through the range of motion to confirm the adequate stability of the skeletal fixation across the ramus osteotomy site on each side.
5. The occlusion is then checked for any centric relation–centric occlusion discrepancies or other causes of malocclusion. If a discrepancy is seen, each proximal segment must be released of its fixation and then again repositioned until the planned, stable, and reproducible occlusion is achieved (i.e., Steps 1 through 5 are repeated, as needed).
Late Malocclusion after Sagittal Split Ramus Osteotomies
Malocclusion after the successful initial healing of sagittal split ramus osteotomies is the result of either skeletal or dental causes.* Skeletal causes may include condylar resorption (see Chapter 36); remodeling or malunion (i.e., relapse) at the osteotomy site; or continued mandibular growth; these conditions are all described in more detail later in this chapter. Dental causes of malocclusion after sagittal split ramus osteotomies are often not appreciated until much later, but they are generally related to the unstable orthodontic positioning of the teeth outside of the boundaries of the alveolar process before or after surgery; this is discussed later in this chapter (see also Chapters 5 and 6).208
Condylar Resorption after Orthognathic Surgery
Although it is rare, idiopathic condylar resorption may present after orthognathic surgery (maxillary or mandibular osteotomies), routine orthodontic treatment, or routine dental procedures; it may also occur spontaneously and not in association with any specific form of treatment (see Chapter 36).12,117,118,143,144,148,159,202,212,237,278,327 Condylar resorption is usually bilateral, symmetric, and seen in young females who are between 15 and 35 years old. Although no agreed upon etiology has been delineated for idiopathic condylar resorption, hormonal and autoimmune causes are suspected (see Chapter 36). Unilateral condylar resorption in association with compressive forces may also be seen after the excessive use of elastics in an attempt to overcome residual malocclusion. The clinical setting may involve heavy elastic use either as part of an orthodontic camouflage approach to avoid surgery (Fig. 17-5) or after orthognathic procedures that did not achieve the desired occlusion. In either case, heavy compressive forces on the condyle may result in temporomandibular joint symptoms followed by condylar resorption with a loss of condylar (posterior facial) height.


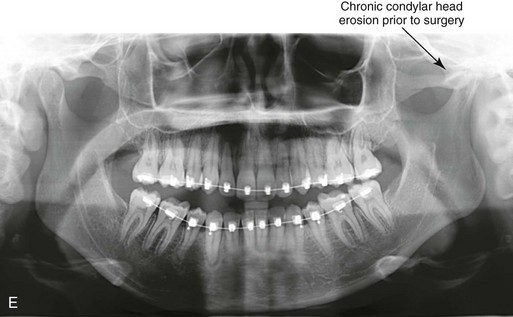
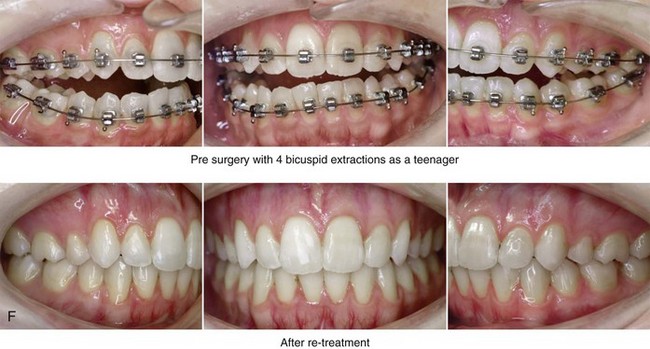
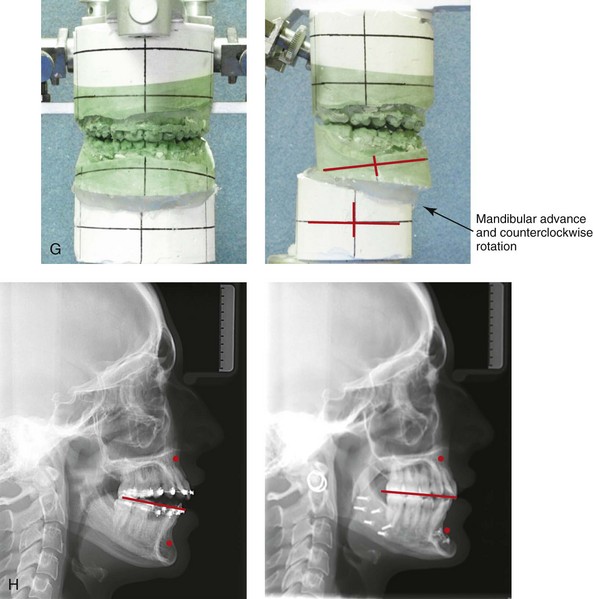
Figure 17-5 A 23-year-old woman was referred for surgical evaluation. During her high school years, she was recognized as having a malocclusion, and she underwent four bicuspid extractions and orthodontic treatment to neutralize the occlusion. During her college years, she experienced a closed lock of her jaw as a result of a dislocated disc within the left temporomandibular joint. After 3 months of conservative management, the patient underwent arthroscopy with lysis of adhesions. With a recurrence of the closed lock attributed to the disc in the left temporomandibular joint, she underwent discectomy and fat graft interposition. A review of the patient’s earlier medical records, including dental models and radiographic analyses, confirmed the primary cause of current malocclusion to be a longstanding developmental jaw deformity that was initially treated with orthodontics alone. Dental relapse had occurred, and the patient’s temporomandibular disorder was likely the result of unstable intercuspation. The relief of the temporomandibular disorder was achieved through an open-joint procedure but with the additional loss of posterior facial height and mandibular asymmetry. The patient was referred to this surgeon and agreed to a comprehensive orthodontic and orthognathic approach. The patient’s procedures included bilateral sagittal split ramus osteotomies (horizontal advancement and counterclockwise rotation) and osseous genioplasty (horizontal advancement). Facial balance and satisfactory occlusion were achieved and maintained without the return of temporomandibular disorder. A, Frontal views in repose before and after retreatment. B, Frontal views with smile before and after retreatment. C, Oblique facial views before and after retreatment. D, Profile views before and after retreatment. E, Panorex radiograph before retreatment. This image indicates a chronic flattening of the left condylar head. F, Occlusal views before retreatment, with orthodontics in progress, and after successful retreatment. G, Articulated dental casts indicate analytic model planning. H, Lateral cephalometric radiographs before and after successful retreatment.
Continued Growth of the Mandible after Orthognathic Surgery
Under normal conditions, the mandible is the last bone in the craniofacial skeleton to complete growth. In general, mandibular growth should be complete between the ages of 14 and 16 years in girls and between the ages of 16 and 18 years in boys. Chronologic and skeletal age will vary from individual to individual, and mandibular growth in men may continue beyond the age of 18 years, but this is uncommon. Jaw growth in girls is usually complete within 2 years after the onset of regular menses. The completion of jaw growth may be assessed in the following ways: 1) via the growth-plate analysis of a hand and wrist radiograph 2) via the analysis of a quantitative condylar head bone scan in comparison to a lumbar vertebra (L2) 3) via the analysis of the mandibular length with the use of serial lateral cephalometric radiographs 4) via the analysis of cervical vertebral maturation with the use of serial lateral cephalometric radiographs 5) via the assessment of serial dental models in centric relation or 6) via the assessment of serial occlusal photographs taken in centric relation.*
Mandibular growth in individuals with micrognathia is generally complete at an earlier age than it is among normal “average” mandibular growers. Alternatively, the cessation of lower jaw growth in individuals with true mandibular excess may occur later than it does in average individuals (Figs. 17-6 and 17-7) (see Chapter 20); this is especially true for individuals with asymmetric mandibular excess growth anomalies (see Chapter 22). Alternatively, the individual with a typical Class II long face growth pattern (i.e., vertical maxillary excess combined with mandibular deficiency) can be assumed to have a normal mandibular growth vector without a tendency for late development (see Chapter 21). I believe that, if the long face patient’s chronic nasal obstruction problem is simultaneously managed at the time of orthognathic surgery (i.e., septoplasty, inferior turbinate reduction, the widening of a tight nasal aperture, and the lowering of the nasal floor), further pathologic vertical growth is also likely to be arrested (see Chapter 10).
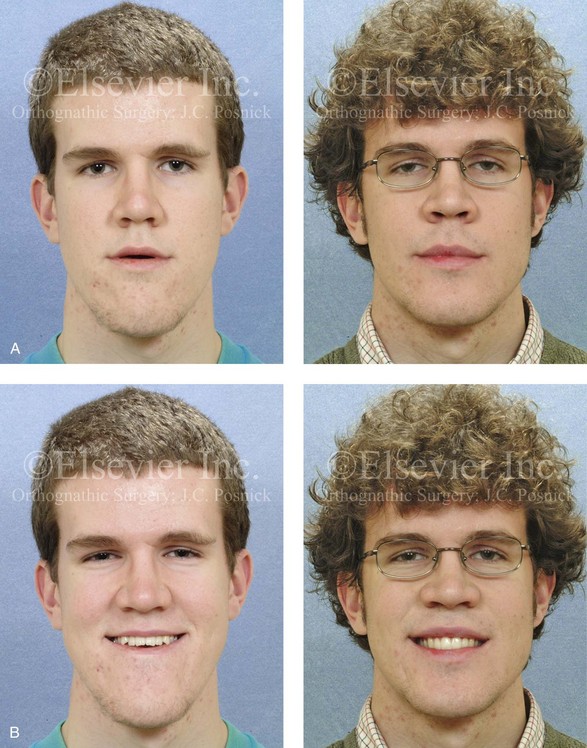
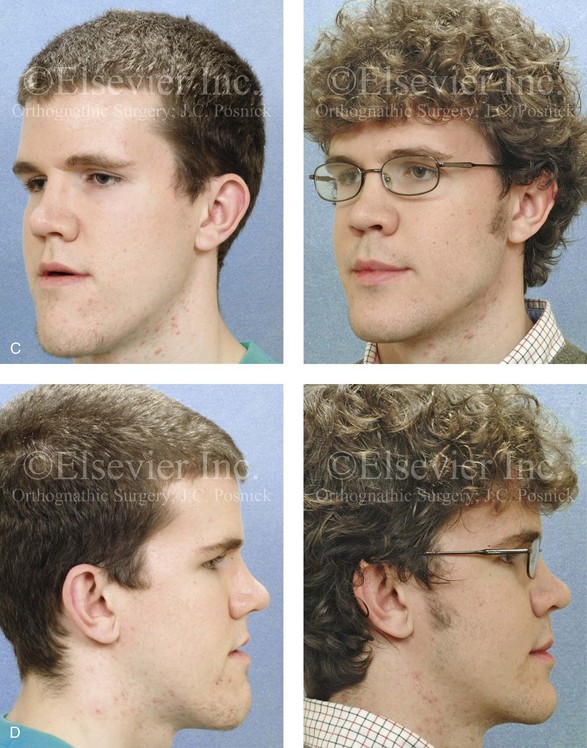
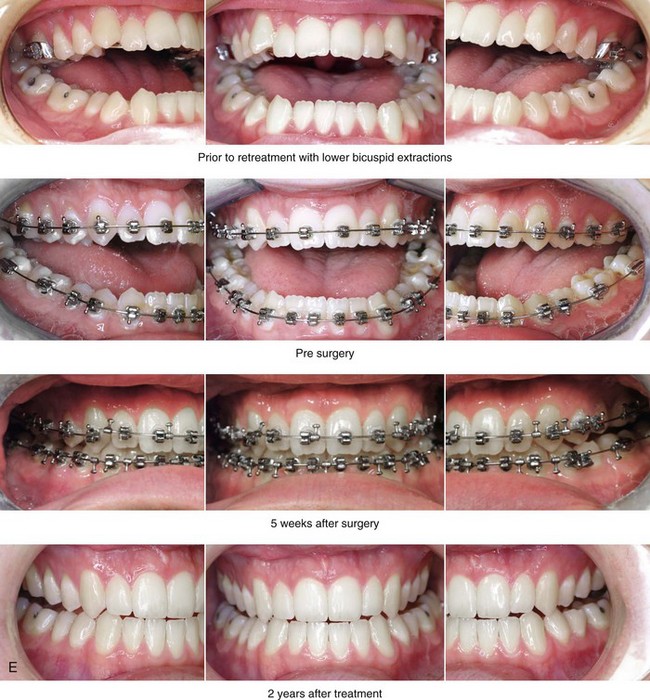
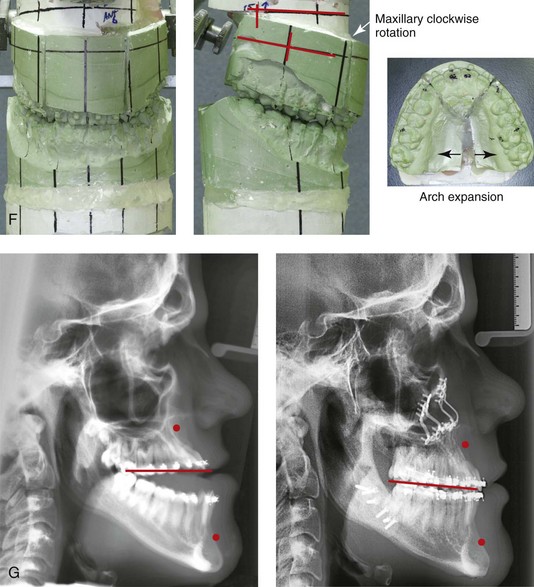
Figure 17-6 An 18-year-old man with malocclusion and a lifelong history of obstructed nasal breathing was referred for the surgical evaluation. The pattern of deformity was maxillary deficiency in combination with relative mandibular excess, which resulted in a severe Class III negative overjet anterior open bite. He had previously undergone growth modification and camouflage orthodontics including lower bicuspid extractions, without success. After a thorough evaluation, he underwent 12 months of orthodontic decompensation followed by jaw and intranasal surgery. The patient’s surgery included Le Fort I osteotomy in segments (horizontal advancement, clockwise rotation, transverse widening, and correction of the arch form) with interpositional grafting; sagittal split ramus osteotomy (minimal counterclockwise rotation); osseous genioplasty (bone burring and recontouring); and septoplasty and inferior turbinate reduction. These procedures were followed by finishing orthodontics. The occlusion achieved during the operation and maintained at the patient’s debracketing 6 months later was ideal. By 2 years after surgery, however, a symmetric Class III negative overjet malocclusion had recurred. A, Frontal views before and 2 years after reconstruction. B, Frontal views with smile before and 2 years after reconstruction. A review of the 2-year postoperative dental models indicated stable maintenance of the arch width and of the correction of the curve of Spee. The models could be articulated into a similar occlusion as had been achieved at the time of operation. Therefore, the cause of change in occlusion could not be attributed to the segmental osteotomies or dental relapse. The cause of the recurrent malocclusion was felt to be either ongoing mandibular growth or Le Fort I osteotomy site relapse. An analysis of the postoperative cephalometric radiographs—which showed an increase in the sella–nasion–B-point angle and the maintenance of the sella–nasion–A-point angle—confirmed maxillary stability. Ongoing mandibular growth was the cause of the malocclusion. Treatment options included Le Fort I osteotomy (3-mm advancement) versus sagittal split ramus osteotomies (3-mm set-back). The patient was pleased with the functional improvements (i.e., swallowing, speech, chewing, lip closure/posture, and breathing) and the enhanced facial aesthetics without temporomandibular disorders. He elected to receive no further treatment. C, Oblique facial views before and 2 years after reconstruction. D, Profile views before and 2 years after reconstruction. E, Occlusal views before retreatment, immediately before surgery, 5 weeks after surgery, and 2 years after treatment. F, Articulated dental casts after analytic model planning. G, Lateral cephalometric radiographs before and after treatment.

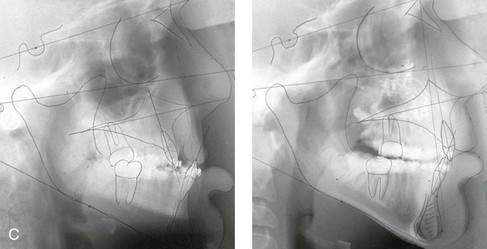
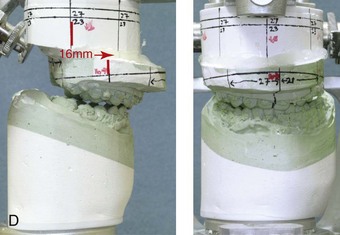
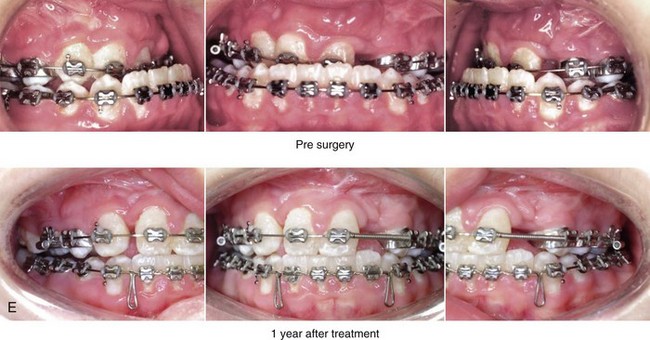
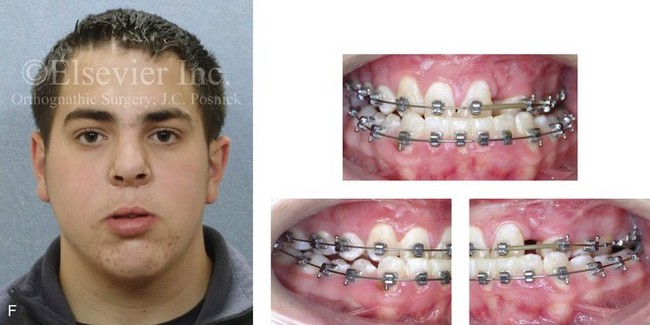
Figure 17-7 A 13-year-old boy born with bilateral cleft lip and palate arrived for surgical evaluation with a severe cleft jaw deformity. He underwent primary lip and palate repair, a pharyngeal flap procedure, bone grafting, and a columella lengthening procedure at another institution. He was referred to this surgeon with severe maxillary hypoplasia that was causing profound effects on his speech articulation, chewing ability, breathing, and self-esteem. For this reason, early jaw reconstruction was chosen. He underwent maxillary Le Fort I osteotomy (horizontal advancement and vertical lengthening with interpositional [iliac] bone grafting). This was carried out with the understanding that further maxillary growth should not be expected, whereas mandibular growth would likely continue and result in a recurrent Class III. A review of the longitudinal cephalometric radiographs after surgery confirmed no significant horizontal maxillary relapse but ongoing mandibular growth. A, Frontal views with smile before and 1 year after surgery just before the removal of the orthodontic appliances. B, Oblique facial views before and 1 year after surgery. C, Lateral cephalometric views before and 1 year after surgery. D, Articulated dental casts that indicate analytic model planning. E, Occlusal views before and 1 year after surgery, just before debanding. F, Facial and occlusal views from when the patient was 18 years old (i.e., 5 years after Le Fort I advancement) that indicate recurrent Class III malocclusion as a result of ongoing mandibular growth.
Ramus Remodeling and Malunion after Sagittal Split Ramus Osteotomy
With the use of rigid internal fixation (e.g., bicortical screws or plates and screws), the remodeling and malunion of the ramus osteotomy site is believed to be an uncommon cause of relapse.109,115,179,206,236,248,302,324 Although infrequent, infection that has led to sequestration (e.g., of the buccal shelf of the proximal segment) and malunion has been reported. In most clinical settings, there is little evidence to support the concept of late relapse at the ramus osteotomy site after satisfactory initial healing has occurred (by approximately 5 weeks). However, limited bone contact or inadequate fixation of the bony segments may cause initial fibrous union followed by malunion and resulting malocclusion. This would be documented as morphologic change in the mandibular angle (i.e., clockwise rotation of the distal segment) in the presence of unchanged condylar morphology (i.e., no ongoing erosion of the condylar head). There would also be measurable change in either the mandibular length (i.e., as measured from the condyle to the pogonion) or the sella–nasion–B-point angle documented during the analysis of the serial cephalometric radiographs after surgery.
Proffit and colleagues do make a case for ramus remodeling with relapse after mandibular set-back when managing a Class III skeletal pattern.248 These authors believe that, when the orthognathic procedure for the management of a Class III skeletal pattern is a mandibular set-back only versus a two-jaw surgery (i.e., with the primary movement being maxillary advancement in combination with only minor mandibular adjustment), then relapse at the ramus osteotomy site is a common occurrence. In a recent clinical study, Proffit and colleagues confirmed that—despite improvements in surgical fixation techniques (i.e., rigid fixation versus intraosseous wires and IMF)—when mandibular set-back only procedures are carried out for a Class III malocclusion, skeletal instability is often significant. They confirmed better long-term skeletal and occlusal stability when two-jaw surgery is performed for the management of Class III skeletal patterns (i.e., maxillary advancement with limited mandibular set-back).251
Le Fort I Osteotomy: Skeletal Stability and Relapse
Immediate (Early) Malocclusion after Le Fort I Osteotomy
Immediate (early) malocclusion that is recognized either intraoperatively or during the first several days or weeks after surgery may occur after a Le Fort I osteotomy unless the following intraoperative conditions are met (see Figs. 17-1 through Fig 17-4)*:
1. After Le Fort I down-fracture osteotomy, full mobilization of the maxilla and the segments (if segmentation has been carried out) is accomplished before the placement of fixation.
2. An accurate prefabricated acrylic splint is secured to the maxillary occlusal surfaces. The splint stabilizes the new maxillary arch form (i.e., the arch width and the curve of Spee) when segmental osteotomies are carried out.
3. After the securing of the splint to the maxillary dentition, IMF is applied to establish the new horizontal position of the maxilla; the dental midline (yaw orientation); the preferred maxillary plane orientation (pitch orientation); and any cant correction (roll orientation) required.
4. With the condyles seated in the terminal hinge position and IMF established via the prefabricated splint, the maxillomandibular complex is rotated until the desired vertical position of the maxilla is achieved.
• Bony prematurities are common with maxillary impaction. It is easy for the surgeon to overlook interferences in the posterior region of the lateral nasal walls just medial to the descending palatine vessels (see Fig. 15-25, A and B).
• Care should be taken to prevent premature contacts across the Le Fort I osteotomy site, which are followed by a “slide” into maximum bone contact during further vertical closure of the maxillomandibular complex. This would cause condylar displacement with malocclusion that should be recognized at the release of the IMF. The malocclusion would typically present as either a symmetric anterior open bite (if both condyles are displaced) or as an asymmetric lateral shift in the bite (if one condyle is displaced).
5. There must be adequate bone contact across the osteotomy site after the maxilla is stabilized with plate and screw fixation into the desired position. If not, an interpositional graft of sufficient quality should be placed and secured (see Chapters 15 and 18). Without adequate bone contact across the osteotomy site, fibrous union may occur (see Chapter 16). Another possibility is that of initial bony union with relapse (i.e., malunion) occurring as full healing proceeds during the 6 to 12 months after surgery, thereby resulting in late malocclusion.
6. Adequate plate and screw stabilization of the maxilla generally requires the placement of titanium fixation at each pyriform rim and each zygomatic buttress (see Fig. 15-26). When interpositional grafts are required, additional titanium fixation is placed from the superior maxilla and extended across the graft to the dentate segment (see Fig. 15-29, A, B, and C). Additional plate and screw fixation may also be placed horizontally across any interdental osteotomies, if needed.
7. With release of the IMF, the occlusion is checked as the mandible is rotated (opened and closed) with the condyles seated in the terminal hinge position. The occlusion must evenly contact and fit passively into the splint. If not, the plate and screw fixation across the Le Fort I osteotomy is released. Any bony interference is then identified and removed. The maxilla is again repositioned and the fixation reapplied (i.e., repeat Steps 4 through 7) until the planned occlusion is achieved and confirmed.
Late Malocclusion after Le Fort I Osteotomy
Skeletal causes of a late malocclusion after Le Fort I osteotomy may include the following: 1) remodeling (relapse) at the Le Fort I osteotomy site (as described later in this chapter) 2) fibrous union at the Le Fort I osteotomy site (as described later in this chapter) 3) remodeling (relapse) at the segmental osteotomy sites (as described later in this chapter) 4) condylar resorption (as described previously in this chapter and in Chapter 36)143 and 5) continued mandibular growth (as described previously in this chapter; see Figs. 17-6 and 17-7).* Dental causes of malocclusion after Le Fort I osteotomy are often not realized until much later. They are related to the unstable orthodontic positioning of the teeth outside of the boundaries of the alveolar process before or after surgery (as described later in this chapter and in Chapters 5 and 6).208
The precise cause of relapse at the Le Fort I osteotomy site is often difficult to pinpoint, but it is generally related to the following: 1) inadequate mobilization of the down-fractured maxilla before the placement of fixation 2) inadequate bone contact across the osteotomy site after the fixation is applied 3) inadequate (non-rigid) plate and screw fixation across the osteotomy site or 4) excessive occlusal forces or movement transmitted across the osteotomy site during initial healing.†
Fibrous union of the maxilla after Le Fort I osteotomy is an infrequent occurence. When it occurs, expect to find painless mobility of the upper jaw, with or without malocclusion. Risk factors should be recognized, at which point surgical techniques and postoperative management can be adjusted to limit this complication (see Fig. 16-21). The combination of extensive horizontal advancement and vertical lengthening will result in large osteotomy site defects with limited bone contact. Failure to form adequate bony bridges at the healing sites is likely to result in delayed healing, fibrous union, or late relapse. Negative influences on bone healing at the Le Fort I osteotomy site may include the following: (1) injury to flap circulation (2) thin osteoporotic bone at the zygomatic buttress and the pyriform rims, with inadequate fixation and (3) the decision to not place interpositional grafts when the bone gaps are of critical size. Additional postoperative healing risk factors include the following: (1) infection or wound dehiscence after surgery (2) the presence of a heavy occlusion (e.g., grinding, clenching) (3) too rapid of a return to normal chewing forces (4) excessive mouth opening against intermaxillary elastics and (5) the breakage (stress fracture) of the fixation plates. Systemic conditions that are known risk factors for poor bone healing include the following: (1) diabetes (2) collagen disease (3) vascular disease (4) osteoporosis or bisphosphonate use (5) nicotine abuse (6) poor nutritional status; and (7) previous radiation treatment.
Relapse across the segmental maxillary osteotomy sites after palatal widening is generally related to the following: (1) inadequate mobilization of the segments (2) inadequate surgical splinting of the new arch shape during initial healing (i.e., the first 5 weeks) (3) inadequate or unstable interdigitating occlusion between the maxillary and mandibular teeth after the splint is removed or (4) inadequate medium-term orthodontic maintenance (i.e., lasting approximately 6 months) with an appropriate appliance after the surgical splint is removed (see Figs. 17-3 and 17-8). Transverse relapse after the removal of the surgical splint may also occur as a result of the use of counterproductive intermaxillary elastic forces. For example, the use of vertical elastics placed on the buccal brackets of the upper and lower molars in an attempt to close posterior open bites may result in the simultaneous unintended collapse of the arch width.



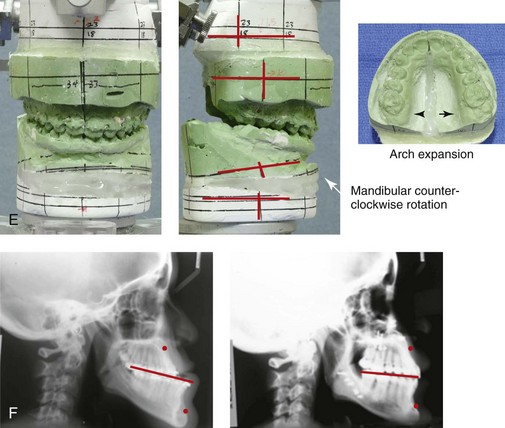
Figure 17-8 A 15-year-old high school student was referred by her orthodontist for surgical evaluation of a long-standing developmental jaw deformity with malocclusion and a lifelong history of obstructed nasal breathing. The pattern of growth disturbance was maxillary deficiency in combination with relative mandibular excess, and this resulted in a Class III negative overjet anterior open bite malocclusion. The patient had undergone growth modification and camouflage orthodontics, without success. Referral to this surgeon was followed by orthodontic decompensation in conjunction with jaw and intranasal surgery and then finishing orthodontics. The patient’s surgery included maxillary Le Fort I osteotomy in two segments (horizontal advancement, transverse widening, and vertical lengthening); sagittal split ramus osteotomies (counterclockwise rotation and minimal horizontal advancement); and septoplasty and inferior turbinate reduction. The surgical occlusion that was initially achieved at operation and then maintained during the early phase of healing was stable. By 6 to 12 months after surgery, a degree of posterior crossbite had recurred. A, Frontal views with smile before and after reconstruction. B, Oblique facial views before and after reconstruction. A review of the postoperative dental models indicated intermolar transverse constriction as compared with what was surgically planned, executed, and achieved at 5 weeks after surgery, when the prefabricated splint was removed. A review of the dental models confirmed a combination of skeletal and dental relapse that resulted in maxillary arch constriction. In retrospect, the postoperative orthodontic mechanics of the labial arch wire to maintain the surgically achieved arch width were not adequate. The use of a transpalatal wire or an acrylic palatal plate maintained for 6 months after surgery may have prevented maxillary arch form relapse after the surgical splint was removed (i.e., 5 weeks after surgery). Treatment options for the residual malocclusion include redo Le Fort I segmental osteotomies with expansion versus surgically assisted rapid palatal expansion. The patient was pleased with the improvements (i.e., chewing, speech articulation, lip closure/posture, and breathing) and the enhanced facial aesthetics. She was left with a functional occlusion without centric relation–centric occlusion discrepancies or temporomandibular disorder. She elected to receive no further treatment. C, Profile views before and after reconstruction. D, Occlusal views with orthodontic decompensation in progress and 3 years after treatment. The positive overjet overbite is maintained but with recurrent maxillary transverse constriction. E, Articulated dental casts that indicate analytic model planning. F, Lateral cephalometric radiographs before and after reconstruction.
1. Inadequate skeletal mobilization. When significant widening of the posterior maxilla is required, bilateral (rather than unilateral) parasagittal osteotomies will assist with the tension-free placement of the segments into the splint (see Chapter 15).
2. Inadequate splint strength. The use of a non-flexible splint (e.g., a reinforced U-shaped acrylic splint, transpalatal support) is essential to maintain the arch width during initial healing (see Chapter 13).
3. Inadequate soft-tissue mobilization. After the completion of segmental osteotomies, the stretching of the palatal soft tissues through the down-fracture (i.e., the use of a spreader forceps) improves the tension-free placement of the segments into the splint.
4. Inadequate postsurgical care. After the splint is removed (i.e., 5 weeks after surgery), the seamless transfer of responsibility from the surgeon to the orthodontist for ongoing maxillary arch form maintenance is essential. The effective use of orthodontic mechanics is generally needed for at least 6 months to retain the arch form. (This is described later in this chapter.)
Orthodontic Treatment: Dental Stability and Relapse
The objective of orthodontics in conjunction with jaw surgery is to align the dentition in each arch by placing the maxillary and mandibular teeth fully within the basal bone. When the jaws and jaw segments are then surgically repositioned, the preferred occlusion is achieved. Following Andrews’ Six Keys to Normal Occlusion provides the framework for the accomplishment of the orthodontic objectives (see Chapters 5 and 6).208
Moen and colleagues carried out a prospective clinical study to evaluate the short-term occlusion achieved and the long-term occlusion maintained after bilateral sagittal split ramus osteotomies with advancement for the treatment of Class II skeletal deformities.208 Prospectively, 36 patients with Class II skeletal patterns who were to undergo bilateral sagittal split ramus osteotomies agreed to participate in the study. The mean age at operation was 33 years (range, 16 to 59 years). All of the study patients underwent perioperative orthodontics and were followed clinically, with dental models and radiographs (i.e., lateral cephalometric and Panorex). These standard records were obtained at 8 weeks, 1 year, and 13 years after surgery. Interestingly, for the majority of patients, cephalometric analysis confirmed insignificant skeletal changes during long-term follow up after successful initial healing had occurred. Long-term recurrent malocclusion was found to be primarily dental rather than skeletal in origin.208 To achieve and then maintain the ideal occlusion, the importance of the stable orthodontic positioning of the teeth in the alveolus cannot be overstated (Figs. 17-9 through 17-14).



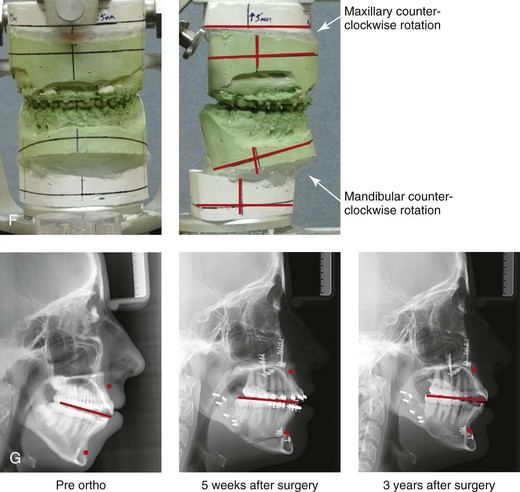
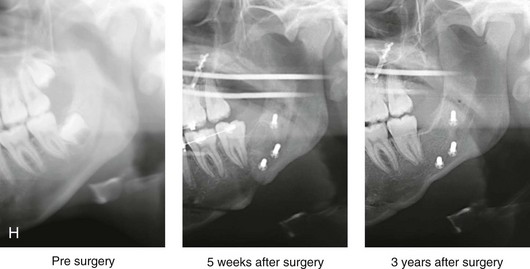
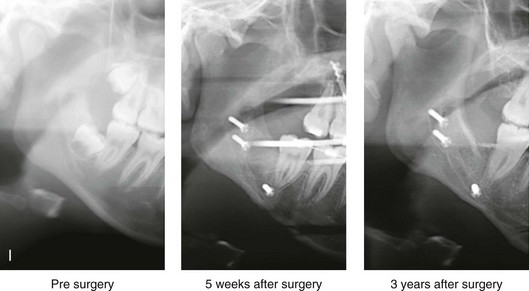
Figure 17-9 A female high-school student was referred by her orthodontist for surgical evaluation. Since her mid childhood years, the patient was known to have a long face growth pattern, and she had a lifelong history of obstructed nasal breathing. She had undergone attempted growth modification followed by orthodontic camouflage, without success. At the time of referral, the patient’s concerns included lip incompetence, gummy smile, weak profile, malocclusion, and nasal obstruction. She agreed to a surgical correction. The orthodontic treatment plan then changed in preparation for orthognathic surgery. Extractions were not carried out to correct the maxillary and mandibular arch forms. The patient then underwent maxillary Le Fort I osteotomy (horizontal advancement and vertical intrusion); bilateral sagittal split ramus osteotomies (minimal horizontal advancement and counterclockwise rotation); osseous genioplasty (vertical reduction and horizontal advancement); and septoplasty, inferior turbinate reduction, and recontouring of the nasal floor. Successful initial surgical healing was achieved. The occlusion maintained at splint removal (i.e., 5 weeks after surgery) was as planned. The orthodontic appliances were removed 6 months after surgery, with ideal occlusion and orthodontic retention continued. The patient returned 3 years after surgery with complaints of recurrent anterior open-bite malocclusion. A, Frontal views in repose before and 3 years after surgery. B, Frontal views with smile before and 3 years after surgery. An analysis was carried out that included the review of lateral cephalometric and Panorex radiographs taken before surgery, 5 weeks after surgery, and 3 years after surgery. The patient had no temporomandibular disorder, and there was no evidence of condylar resorption. Therefore, idiopathic condylar resorption was ruled out. Cephalometric analysis of the presurgical, early postoperative, and late postoperative cephalometric radiographs revealed satisfactory initial repositioning and healing of the jaws without skeletal relapse at 3 years. A comparison of the 5-week postoperative and 3-year postoperative sella–nasion–A-point and sella–nasion–B-point angles and facial heights confirmed skeletal stability. A review of the arch form (i.e., the dental models) suggested orthodontic relapse that included transverse maxillary constriction and incisor intrusion. The mandibular arch form also indicated dental relapse. Treatment options included redo Le Fort I osteotomy in three segments for the correction of the arch form versus surgically assisted rapid palatal expansion. Orthodontics would also be required. The advantages of four bicuspid extractions as part of dental decompensation were also discussed. The patient was pleased with the enhanced facial aesthetics (i.e., a less gummy smile, an improved profile, and lip closure) and the improved breathing that was achieved. She also did not have any temporomandibular disorder. She elected to receive no further treatment. C, Oblique facial views before and 3 years after surgery. D, Profile facial views before and 3 years after surgery. E, Occlusal views before the orthodontic retreatment, immediately before surgery, 5 weeks after surgery, and 3 years after surgery. F, Articulated dental casts that indicate analytic model planning. G, Serial lateral cephalometric views before orthodontic retreatment, 5 weeks after surgery, and 3 years after surgery. H, Serial Panorex views of the left condyle–ramus before surgery, 5 weeks after surgery, and 3 years after surgery. I, Serial Panorex views of the right condyle–ramus before surgery, 5 weeks after surgery, and 3 years after.



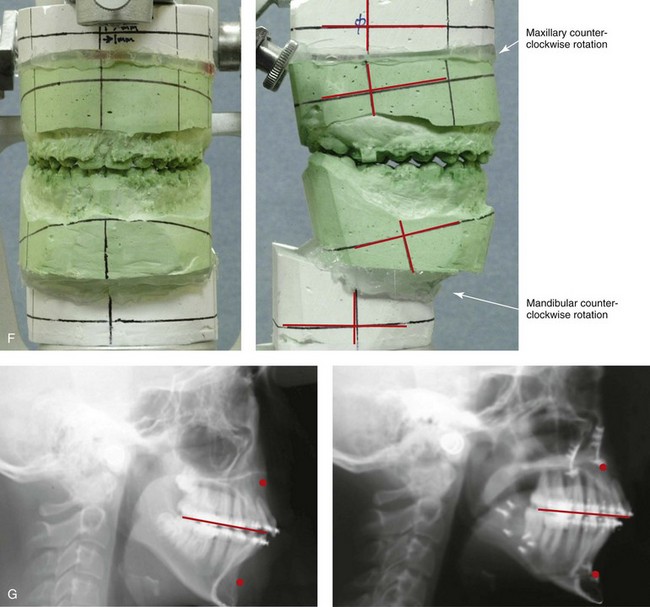
Figure 17-10 A 14-year-old girl was referred by her orthodontist for surgical evaluation. She presented with a long face Class II growth pattern and a lifelong history of obstructed nasal breathing. She underwent non-extraction orthodontics, including mechanics to correct the maxillary arch form. The patient’s surgery included maxillary Le Fort I osteotomy (vertical intrusion, horizontal advancement, and counterclockwise rotation); sagittal split ramus osteotomies (horizontal advancement and counterclockwise rotation); osseous genioplasty (vertical reduction and horizontal advancement); and septoplasty, inferior turbinate reduction, and nasal floor recontouring. Healing occurred without complications. The occlusion that was initially achieved and maintained at 5 weeks after surgery was as planned. Unfortunately, the patient refused continued postoperative orthodontics and the appliances be removed 3 months after surgery. She was also not compliant with retainer use. By 1 year after surgery, there was a recurrence of the anterior open bite. A, Frontal views in repose before and after treatment. B, Frontal views with smile before and after treatment. A review of the dental models confirmed dental relapse with a recurrent accentuated curve of Spee and arch constriction of the maxilla. In retrospect, segmental orthodontic mechanics followed by segmental maxillary surgery would likely have prevented this problem. At this time, treatment options include segmental orthodontic mechanics and redo Le Fort I osteotomy in segments. The patient and her family were pleased with the improvements in lip closure/posture, a diminished gummy smile, improved profile aesthetics, and better breathing during the day and night. The patient did not have temporomandibular disorder, and she elected to received no further treatment. C, Oblique facial views before and after treatment. D, Profile views before and after treatment. E, Occlusal views in mixed dentition before treatment, with preoperative orthodontics complete, with initial surgical occlusion achieved (i.e., 5 weeks after surgery), and 1 year after treatment. Note: Discoloration of right maxillary central incisor crown suggests pulpal pathology. F, Articulated dental casts that indicate analytic model planning. G, Lateral cephalometric views before and after treatment.
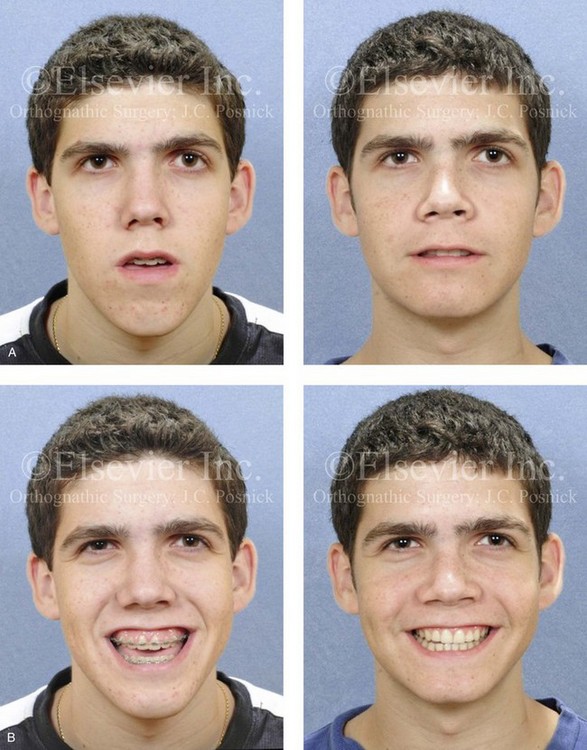
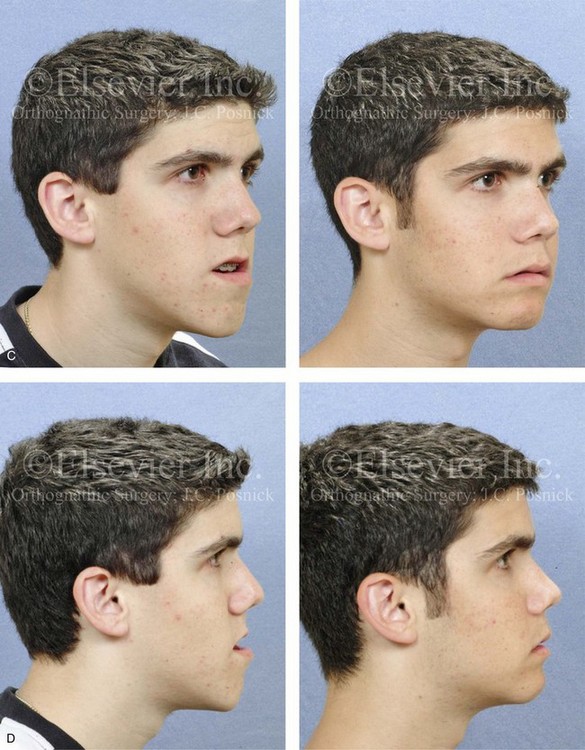
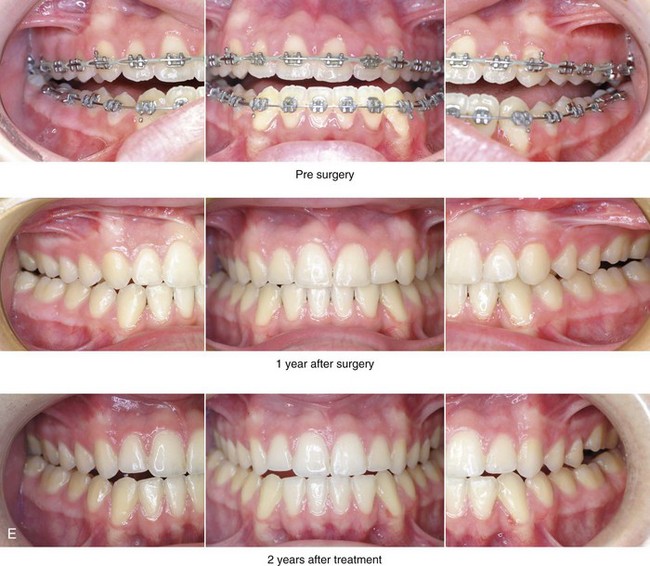
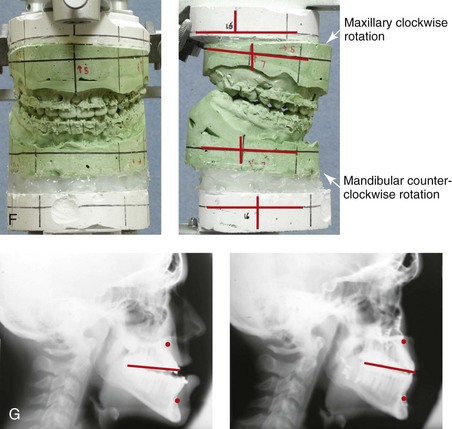
Figure 17-11 A 17-year-old boy was referred by his orthodontist for the surgical evaluation of a long-standing developmental jaw deformity with malocclusion and a lifelong history of obstructed nasal breathing. The patient had undergone both growth modification and camouflage orthodontics, without success. Examination confirmed a Class III long face growth pattern with an anterior open bite. He then underwent orthodontic mechanics in preparation for jaw surgery. The maxillary arch was leveled with orthodontic mechanics. The patient’s surgery included maxillary Le Fort I osteotomy (horizontal advancement, vertical shortening, and clockwise rotation); bilateral sagittal split osteotomies of the mandible (minimal set-back and clockwise rotation); and septoplasty, inferior turbinate reduction, and nasal base recontouring. An osseous genioplasty with horizontal advancement would have further enhanced the patient’s facial aesthetics but was refused. The surgery was followed by finishing orthodontics. The patient’s occlusion at 5 weeks after surgery was excellent, and it remained so at the time of the debracketing 6 months after surgery. By 1 year after surgery, a slight Class III tendency with posterior constriction was evident. A, Frontal views in repose before and after surgery. B, Frontal views with smile before and after surgery. By 2 years after surgery, the anterior occlusion was edge to edge, and the maxillary arch form was irregular. The cause of the recurrent malocclusion was felt to be either ongoing mandibular growth or a loss of maxillary arch form as a result of dental relapse. A review of the cephalometric data suggested stability of the mandible (i.e., the sella–nasion–A-point and sella–nasion–B-point angles were unchanged at intervals after surgery). A review of the dental models confirmed dental relapse with a change in the maxillary arch form (i.e., constriction in the arch width and an accentuated curve of Spee). Treatment options include maxillary Le Fort I osteotomy in segments for the correction of the arch form versus surgically assisted rapid palatal expansion. An osseous genioplasty was also offered to improve the patient’s profile aesthetics. The patient was pleased with the functional improvements (i.e., chewing and speech articulation), and he did not have temporomandibular disorder; he also appreciated the enhanced facial aesthetics. He elected to receive no further treatment. C, Oblique facial views before and after surgery. D, Profile views before and after surgery. E, Occlusal views immediately before surgery and at 1 year and 2 years after surgery. F, Articulated dental casts that indicate analytic model planning. G, Lateral cephalometric radiographs before and after surgery.


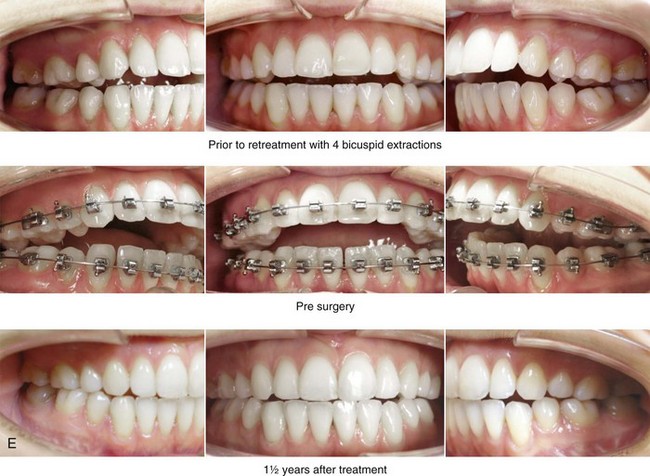
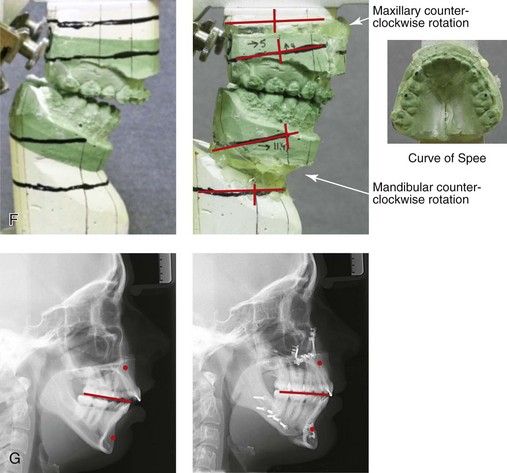
Figure 17-12 A 20-year-old female college student was referred for surgical evaluation. During the mixed dentition, she was noted to have a long face growth pattern with an anterior open bite. She was treated from the time that she was 11 to 15 years old with growth-modification followed by a four-bicuspid orthodontic camouflage approach, without success. She presented for surgical evaluation with complaints of chronic obstructed nasal breathing; an anterior open bite that caused difficulty with chewing and with speech articulation; wide lip separation with lip strain at closure; and a retrusive profile appearance. There was generalized root resorption and early anterior mandibular labial bone loss and gingival recession. A comprehensive evaluation also confirmed septal deviation and inferior turbinate hypertrophy with increased nasal airway resistance. The patient agreed to an orthodontic and orthognathic/intranasal surgical approach. Her surgery included maxillary Le Fort I osteotomy in segments (arch form correction, horizontal advancement, vertical shortening, and counterclockwise rotation); bilateral sagittal split ramus osteotomies (horizontal advancement and counterclockwise rotation); osseous genioplasty (horizontal advancement); and septoplasty, inferior turbinate reduction, and nasal floor recontouring. A, Frontal views in repose before and after treatment. B, Frontal views with smile before and after treatment. The occlusion that was initially achieved and maintained at 5 weeks after surgery was as planned. Postoperative orthodontic appointments were complicated by the patient’s attendance at an out-of-state college. At the time of appliance removal (i.e., 10 months after the operation), there was partial recurrence of the anterior open bite. The occlusion then remained stable at the 18-month postoperative interval. There was no popping, clicking, or pain in either temporomandibular joint. There was mild masticatory muscle discomfort, which was relieved with an effective night guard. An analysis of the postoperative cephalometric radiographs, which were taken at 1 month and 18 months after surgery, confirmed a stable SNB angle. The condyle-to-gonion measurement also remained stable. A review of the condyle morphology on the Panorex radiograph revealed no significant change. A review of the dental models (i.e., the surgical planning models and those from 16 months after surgery) suggested a degree of dental relapse in the form of recurrent curve of Spee issues in the maxilla and the mandible. The patient elected to undergo no further treatment. C, Oblique facial views before and after treatment. D, Profile views before and after treatment. E, Occlusal views before retreatment, with orthodontics in progress, and at 16 months after surgery. F, Articulated dental casts that indicate analytic model planning. G, Lateral cephalometric radiographs before and 16 months after surgery.
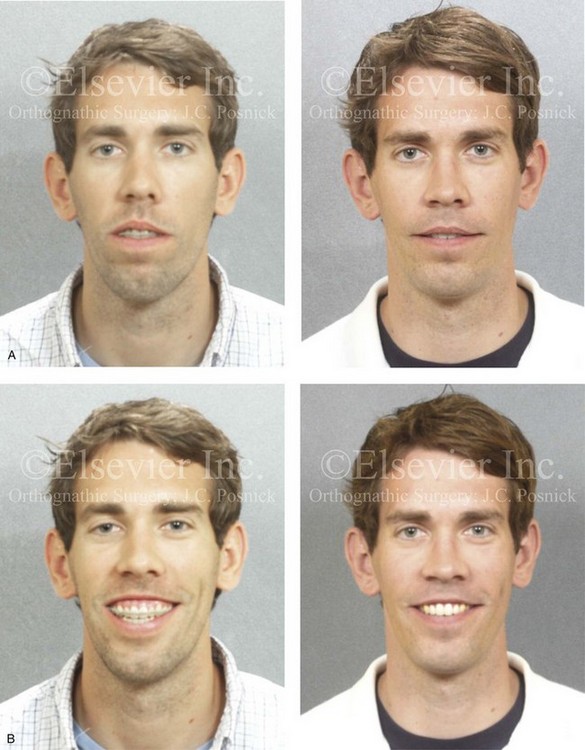
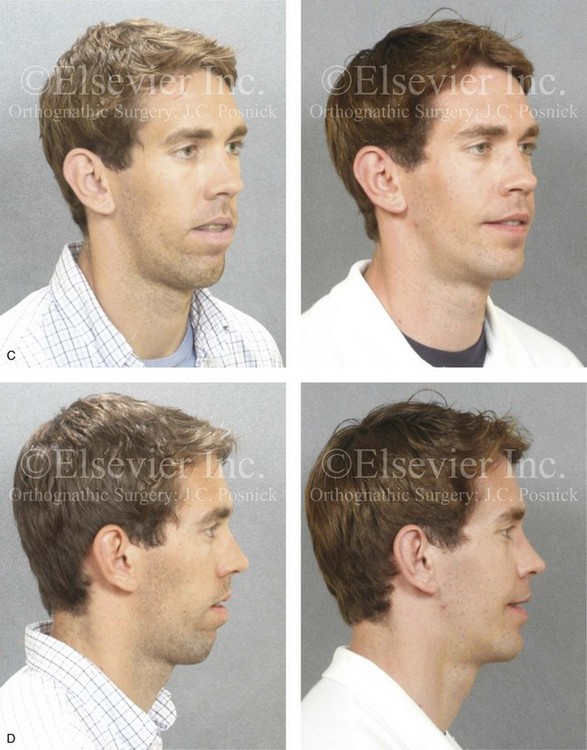

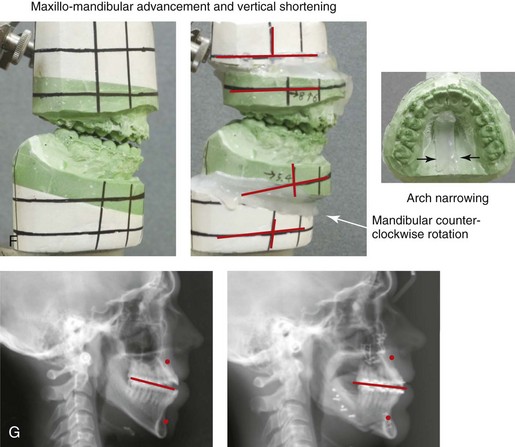

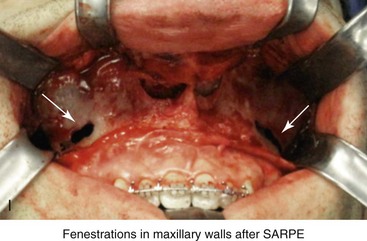
Figure 17-13 A 25-year-old man presented with a long face anterior open-bite growth pattern. He had undergone four bicuspid extractions and a surgically assisted rapid palatal expansion procedure to reduce crowding and to expand the maxillary arch width at another institution. He was referred to this surgeon with residual maxillofacial problems, including jaw discrepancy, residual malocclusion, and chronic obstructed nasal breathing. The patient agreed to additional orthodontic mechanics and surgery, including Le Fort I osteotomy in two segments (vertical shortening, horizontal advancement, and arch narrowing); sagittal ramus osteotomies (horizontal advancement and counterclockwise rotation); septoplasty; the reduction of the inferior turbinates; and osseous genioplasty (vertical shortening and horizontal advancement). He is shown before and after the completion of his final phase of treatment. A, Frontal views in repose before and after retreatment. B, Frontal views with smile before and after retreatment. C, Oblique facial views before and after retreatment. D, Profile views before and after retreatment. E, Occlusal views after earlier orthodontic treatment including four bicuspid extractions, after surgically assisted rapid palatal expansion (SARPE), just before orthognathic surgery, and after retreatment. F, Articulated dental casts that indicate analytic model planning. G, Lateral cephalometric views before and after retreatment. H, Panorex radiograph before retreatment. I, Intraoperative view of the anterior maxilla after the surgically assisted rapid palatal expansion (SARPE) procedure and just before Le Fort I osteotomy.
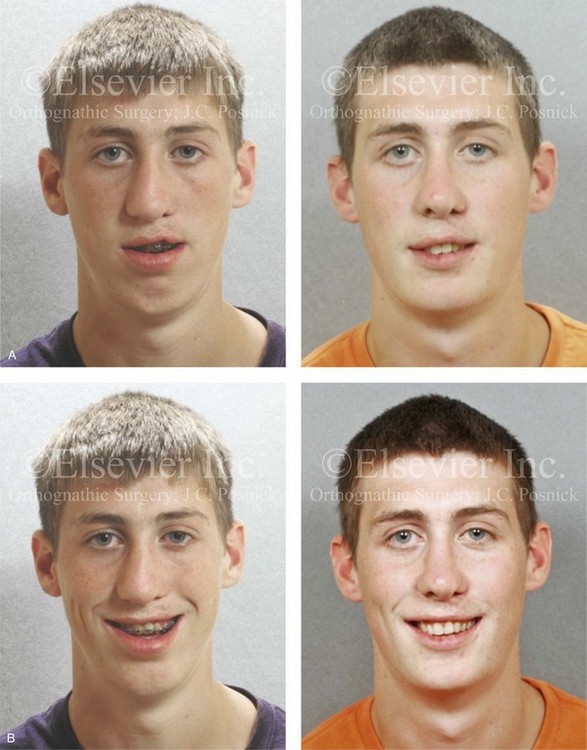
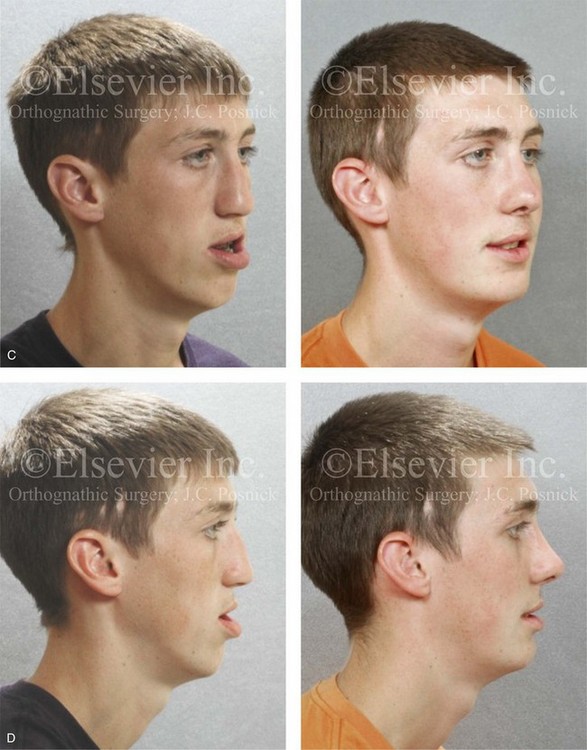

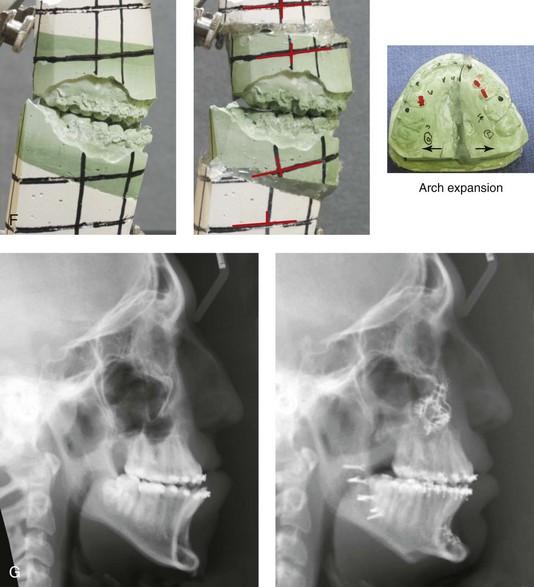
Figure 17-14 A young man born with a unilateral cleft lip and palate had been treated by other surgeons. His treatments had included primary cleft lip repair; primary cleft palate repair; two cleft lip revisions; three cleft palate revisions; the placement of a superiorly based pharyngeal flap; iliac grafting for a cleft defect; cleft rhinoplasty; and suboptimal Le Fort I osteotomy with an external RED distraction osteogenesis (DO) device. The patient was referred to this surgeon when he was 17 years old with residual cleft deformities, including the following:
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


