Problems in Eruption of First and Second Permanent Molars
The dentition in the molar region develops over a long period of time. The formation of the first permanent molars begins before birth; on average they emerge at about age 6 years. The second and third molars follow at about 12 and 18 years, respectively. Duration of development of this region is connected with the relatively slow increase in size of the related tooth-bearing parts of the jaws.
Compared with the regions of the dentition mesial to the permanent molars, the development is simple. There are no deciduous teeth that must exfoliate, and the eruption sequence does not vary. Problems in the molar region are thus limited principally to anomalies of position, eruption, and crowding.
The aspects dealt with in this chapter are: ectopic eruption of first permanent molars, submerged second deciduous molars, agenesis of permanent molars, and ankylosis, impaction, and crowding in the molar region.
16.2 Ectopic eruption of first permanent molars
In approximately 3% of children the first permanent molar erupts too far mesially. It usually contacts the roots of the adjacent second deciduous molar via its mesio-occlusal marginal ridge. This results in atypical resorption of the deciduous molar root.17 Ectopic eruption occurs mainly in the maxilla, seldom in the mandible. Ectopic eruption of the maxillary first permanent molars is associated with mesial angulation and sometimes with a relatively large crown. Spatial relationships within the jaws and arches appear to have only a limited importance.18
Ectopic eruption can be diagnosed clinically on the basis of partial or total failure to emerge. The picture on radiographs is explicit: the mesio-occlusal marginal ridge of the permanent molar is located apical to the crown of the second deciduous molar and is trapped under it.
In the maxilla about half the cases of ectopic eruption appear to correct themselves spontaneously. The first permanent molar ceases to be restrained by the deciduous molar and resumes eruption. In the remainder (and those usually have relatively large first permanent molar crowns) the obstruction remains and the first permanent molar does not erupt farther until the deciduous molar exfoliates or is extracted (Figs. 16-1 and 16-2).
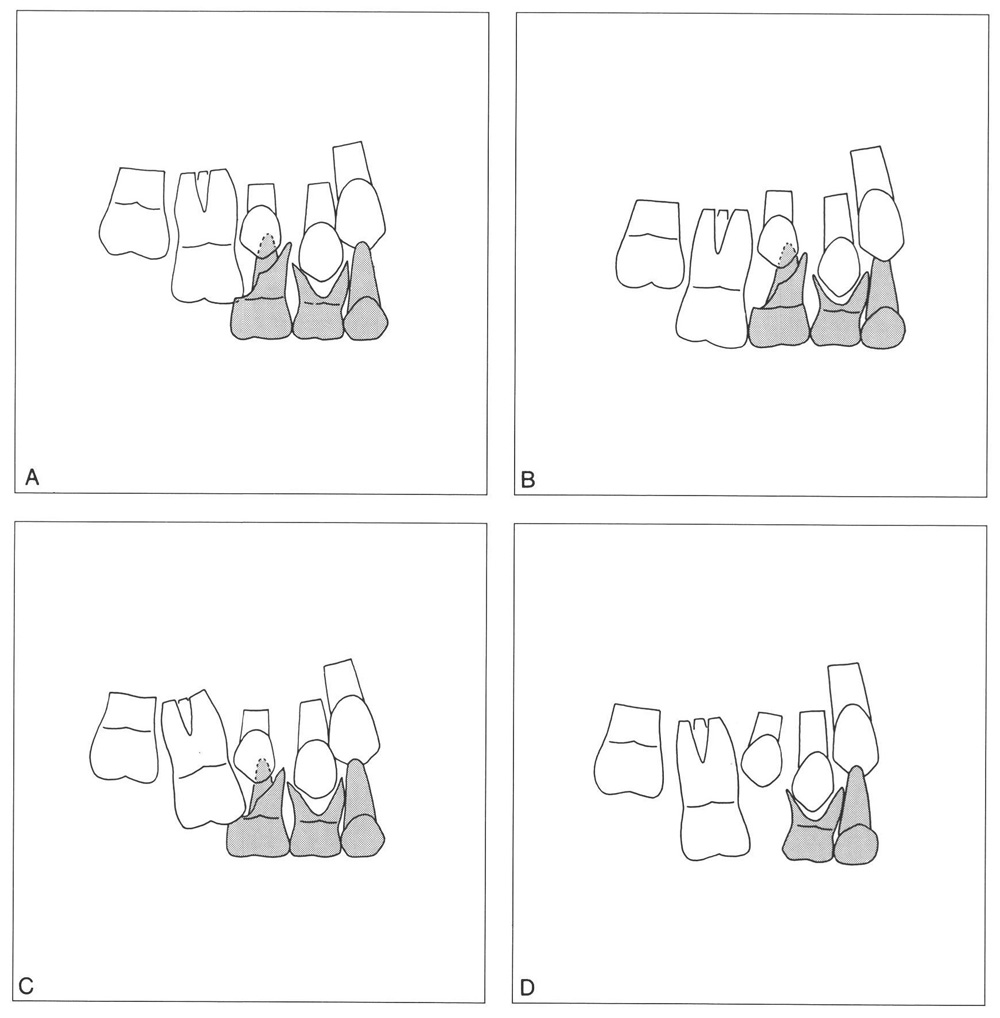
Fig. 16-1 Ectopic eruption of maxillary first permanent molars. (Drawings based on radio-graphs from Bjerklin and Kurol.18)
A The mesio-occlusal marginal ridge of the maxillary first permanent molar is located apical to the crown of the second deciduous molar, the roots of which show atypical resorption.
B Spontaneous correction of the situation in A, a year later. The limited obstruction has been overcome by movement of the first permanent molar.
C Marked mesial angulation with resorption of the second deciduous molar; spontaneous correction cannot be expected.
D After exfoliation of the second deciduous molar, the first permanent molar has emerged along its mesially directed path; the space available for the second premolar is significantly reduced.
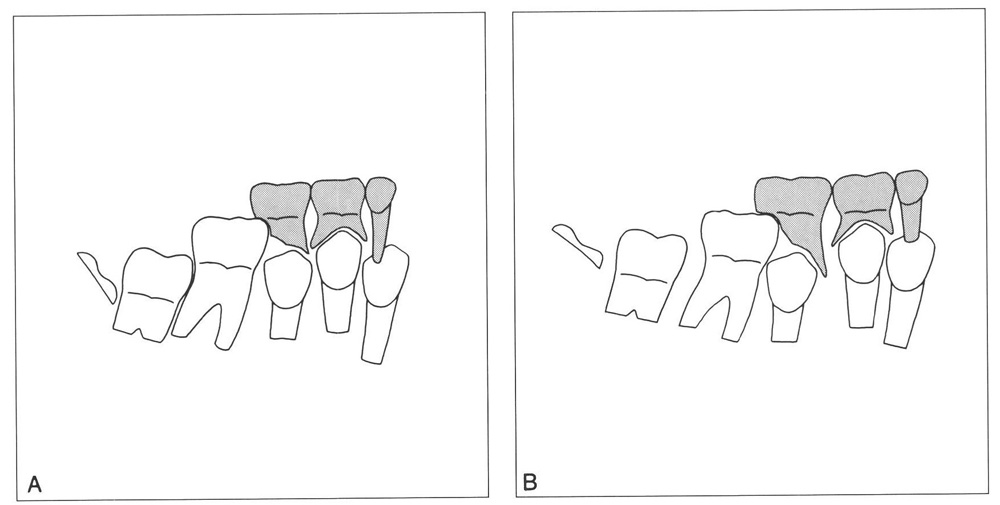
Fig. 16-2 Ectopic eruption of the mandibular first permanent molar, where the phenomenon seldom occurs.
A Because the limited obstruction is associated with crowding in the molar region, spontaneous corrective movement is not possible. The second deciduous molar will only exfoliate when the roots have resorbed.
B Marked obstruction that does not correct itself despite ample space dorsal to the first permanent molar (large posterior section of the apical area).
When ectopic eruption of a first permanent molar is found, an estimate should be made of the likelihood that emergence will happen spontaneously or not occur until after the second deciduous molar has been lost. If it has not fully emerged by the age of 7, most likely no natural correction will take place.18 The best way to judge the situation is by comparing the tooth in question with the corresponding one on the other side. If that had emerged a year or more previously, prognosis for normal eruption will be poor. Radiographs will provide positive information; the extent of the obstruction by the deciduous tooth and the degree of its root resorption are immediately obvious. The approach to follow depends mainly on these conditions.242
If spontaneous correction is not expected, the obstruction should be eliminated. When resorption of the deciduous second molar that is caused by the first permanent molar is only slight, the first molar often can be displaced sufficiently distally by inserting a brass ligature between it and the deciduous molar and tightening it every few days. If the contact point is accessible enough, self-locking separating springs or plastic separating rings can be inserted.
Where the atypical resorption is extensive, extraction of the deciduous molar can be considered. A removable orthodontic appliance can be used to move the permanent molar distally once it has emerged sufficiently. Subsequently a space maintainer should be employed to hold the space that was regained, until the second premolar has emerged (Fig. 16-3).
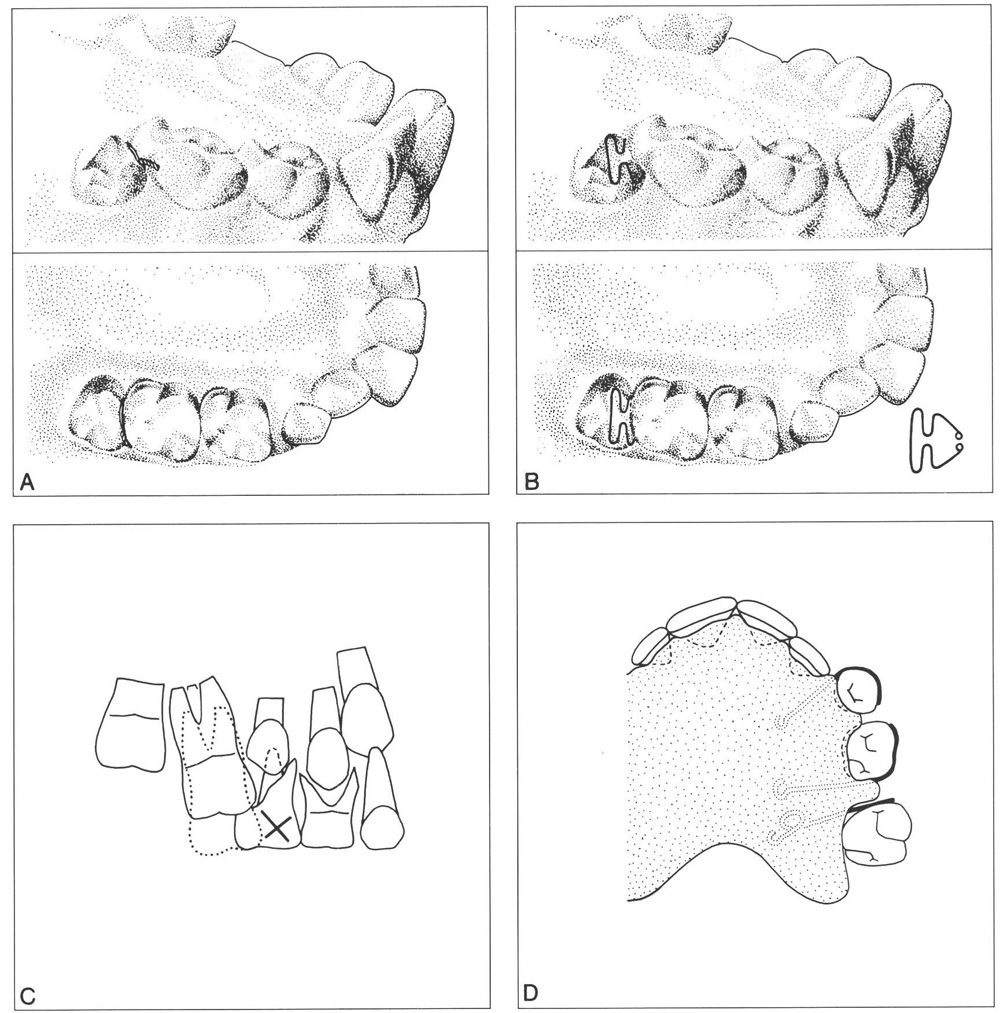
Fig. 16-3 Methods for correcting ectopic eruption of maxillary first permanent molars.
A Where the atypical resorption of the second deciduous molar is limited, a soft brass ligature (0.4 to 0.6 mm in diameter) can be used to clear the obstruction. The wire should be tightened every few days.
B The necessary space can also be gained using self-locking separating springs or plastic separating rings.232
C Where the obstruction is considerable, removal of the second deciduous molar should be considered. Subsequently, the first permanent molar will arrive too far mesially in the dental arch.
D For distal movement of the first permanent molar an acrylic resin removable appliance can be used. In certain cases, a simple lip bumper (.045-inch arch) or a headgear placed on the first permanent molars can serve well.
One can also conserve the second deciduous molar and use it as anchorage for a force uprighting the first permanent molar and moving it distally. An advantage of this approach is that no retention is necessary afterwards if the deciduous tooth remains (Fig. 16-4).
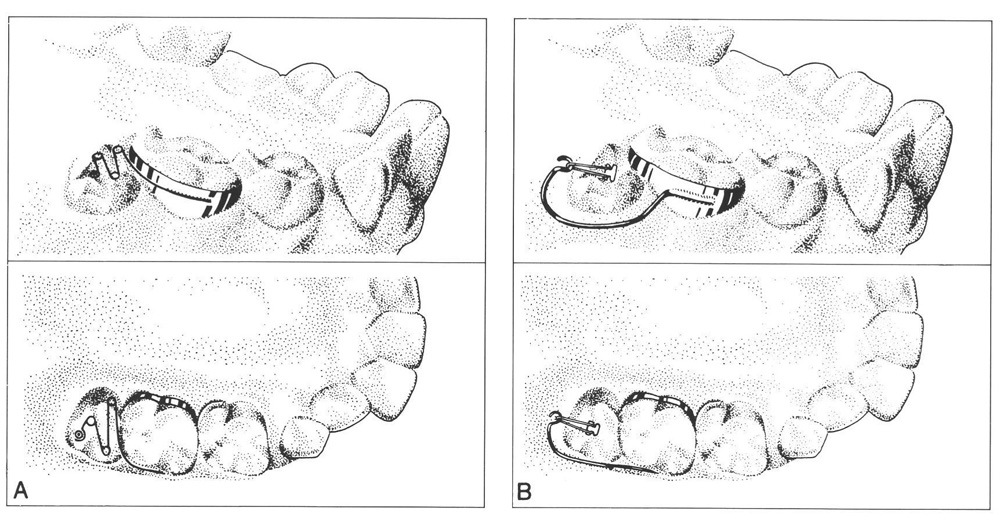
Fig. 16-4 Techniques for obtaining distal movement of a severely obstructed ectopic erupting first permanent molar, when removal of the second deciduous molar is not desired.
A A spring is soldered to a band fitted to the second deciduous molar. A fter the band has been cemented, the spring is hooked under a button bonded on the occlusal surface of the first permanen t molar.79, 163
B A strong extension of orthodontic wire is fixed to the band on the second deciduous molar. A hook has been bonded to the first permanent molar and an elastic band is stretched between the two.114
A first permanent molar can also be uprighted and moved distally by use of two bonded brackets between which a wire is attached that exerts the required force.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


