Abnormal Lip Positions After Transition of the Incisors
A closed mouth with normal lip contact is associated with nasal breathing, provision of labial support for the maxillary and mandibular incisors, and vertical support for the maxillary incisors. The orofacial region can function and mature normally.
However, there is great variability in lip positions, embracing the way in which upper and lower lips touch each other and the relation between lips and teeth. In this connection important factors are the size, shape, and mutual relations of the bony structures directly behind the lips, the alignment and occlusion of the incisors, and the size and activity of the lips.
After first briefly describing normal lip position, this chapter will cover different lip situations as they relate to various orthodontic deviations; in this regard the emphasis is on Class 11/1 anomalies. Subsequently the discussion leads to changes that occur in lips and lip posture during growth and maturity. The diagnosis and detection of deviant lip positions and preventive and therapeutic measures that can be used are covered.
Postnatally, a baby’s mouth at rest is closed. The jaws are relatively little developed, the alveolar processes are not yet built up, the tongue lies partly between the arches of the jaws, and there is ample lip tissue to maintain mouth closure.
In the period from birth to the first transitional period, normal mouth closure is maintained. The rapid growth of the jaws and development of the teeth seldom give rise to a situation wherein the available tissue is inadequate to provide good lip seal. This problem arises usually only after the maxillary permanent incisors have been in the mouth some time, and the development of the lips is relatively behind that of the dentition. The normal pattern of development is for the permanent incisors to emerge more labially than their predecessors so that, if the development of the lips is slower, the deficiency is emphasised. The mouth then is not closed when at rest; the lips can only meet if active muscle force is used.
Incomplete lip seal is only seen in a small proportion of children. This situation will improve gradually unless other anomalous circumstances prevail. A few years later the lips have caught up to the underlying tissues in their growth, and a proper seal can be achieved once more.
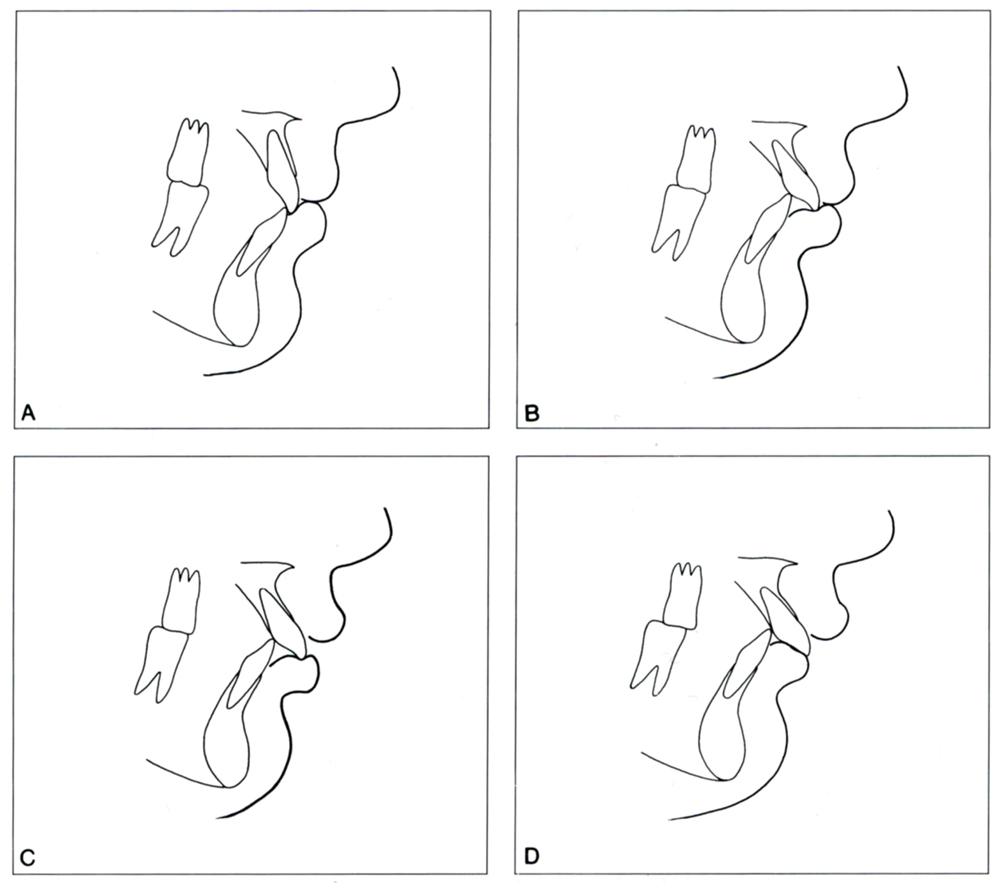
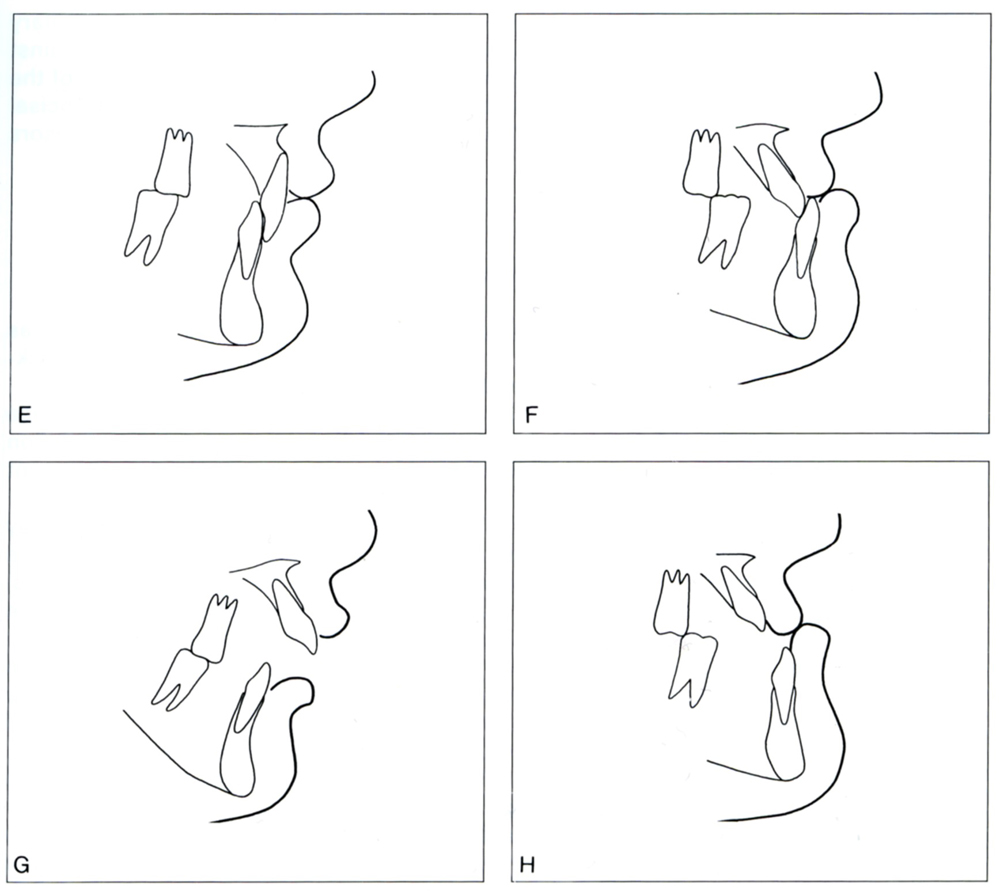
Fig. 12-1 Variations in lip position.
A Normally the upper lip lies against the maxillary incisors and the lower lip lies against the mandibular incisors and the incisal edges and part of the labial surface (1 to 3 mm) of the maxillary incisors. The anterior surface of the lower lip is slightly dorsal to that of the upper Up.
B In mild Class 11/1 anomalies with disto-occlusion of half a premolar crown width (1/2 P. W. -disto) and moderate overjet and overbite, normal lip positions can exist with the lower lip no further dorsal than usual; the plica menta/is is deeper however.
C Class 11/1 anomalies of moderately large extent (3/4 P. W. -disto) and correspondingly increased overjet and overbite can still permit the lower lip to contact the maxillary incisors incisally.
D In serious Class 11/1 anomalies (1 P. W.-disto) with their associated incisor relationships, the lower lip often will be found dorsal to the maxillary incisors. The maxillary incisors can come into supraposition as the result of overeruption.
E Class 11/2 anomalies always show a high lip line. The maxillary central incisors are excessively covered by the lower lip. The lips maintain a positive lip seal at rest. The anterior surface of the upper lip is slightly ventral to that of the lower lip.
F In Class III anomalies the anterior surface of the lower lip is ventral to that of the upper lip. The larger the reversed overjet, the more pronounced is that effect. Even in pronounced Class III anomalies, the lips achieve satisfactory closure in most cases, because the maxillary incisors are everted and the mandibular incisors are retroclined. If the mandible is held in rest position the lower lip is usually less prominent than when the teeth are in occlusion.
G Open bite anomalies with disto-occlusion and excessive lower face height often are associated with an open mouth. The lips are slightly active and short, particularly the upper lip.
H Open bites combined with Class III anomalies usually display a closed lip relation. However that is not the case when there is restricted nasal breathing; an open mouth is then a vital need (for adequate respiration).
When there is an adequate overjet and overbite with normal lip posture, the maxillary central incisors are to a large extent covered by the upper lip. The lower lip lies against the mandibular incisors and partly against the incisal edges and labial surfaces of the maxillary incisors. The lip line (stomion) is at a level 1 to 3 mm cervically from the incisal edges of the maxillary central incisors. The lower lip supports the maxillary incisors labially and vertically; the upper lip works only labially (Fig. 12-1A).
12.3 Lip positions in Class 11/1 anomalies
The mouth is closed until the first transitional period, in Class 11/1 cases as well as normal ones. In rare instances with a pronounced overjet (e.g., excessive thumb-sucking) the lower lip can be found to lie palatal to the maxillary deciduous incisors.
After emergence of the maxillary permanent incisors an abnormal lip position can arise from a large overjet (Fig. 12-1B to D). Moreover, the lower lip can take up a position between the maxillary and mandibular incisors, which influences further development in a deleterious way (Fig. 12-1D).
The lip position found after transition of the incisors will depend on a complex interplay of facial growth, development of the dentition, and functional influences. The picture is more simply and clearly interpreted by dividing the whole into a number of factors. These are set out in drawings (Figs. 12-2 to 12-13). In succession there are: the morphology of the craniofacial skeleton (Fig. 12-2); direction of growth in the face (Fig. 12-3); quantity of lip tissue (Fig. 12-4); height of the lip line (Fig. 12-5); path of eruption of the incisors (Fig. 12-6); diastemata in the deciduous dentition (Fig. 12-7); size ratio between crowns of deciduous and permanent incisors (Fig. 12-8); rotations of permanent incisors (Fig. 12-9); early resorption and exfoliation of deciduous teeth (Fig. 12-10); increase of the intercanine width (Fig. 12-11); deviant habits (Fig. 12-12); and premature loss of deciduous molars (Fig. 12-13).
It seldom occurs that just one of the 12 factors will lead to positioning of the lower lip palatal to the maxillary incisors. Rather, such a situation mostly occurs because of a combination of several factors that are interdependent or causally related. For example, there is a connection between the available room in the maxillary dental arch and the increase in intercanine width. In addition, the path of emergence of the maxillary central incisors depends on the height of the lip line.60 Further, the bulk of lip tissue is related to the form of the craniofacial skeleton and the direction of growth. Some factors can exercise favourable influence whereas others are deleterious. Mutual effects can either enhance or neutralise each other. When many unfavourable factors are involved, the lower lip will most likely come to rest against the palatal surfaces of the maxillary incisors. What may appear to be trivial details can tip the scales one way or the other.
If the lips are closed, the location of the anterior aspect of the lower lip is determined not by the mandibular incisors but by the maxillary incisors. The size of the overjet appears to have no demonstrable influence on the anteroposterior relation of the anterior surfaces of the upper and lower lips when there is a normal lip seal. However, the depth of the plica mentalis does increase proportionately as the overjet becomes larger.35
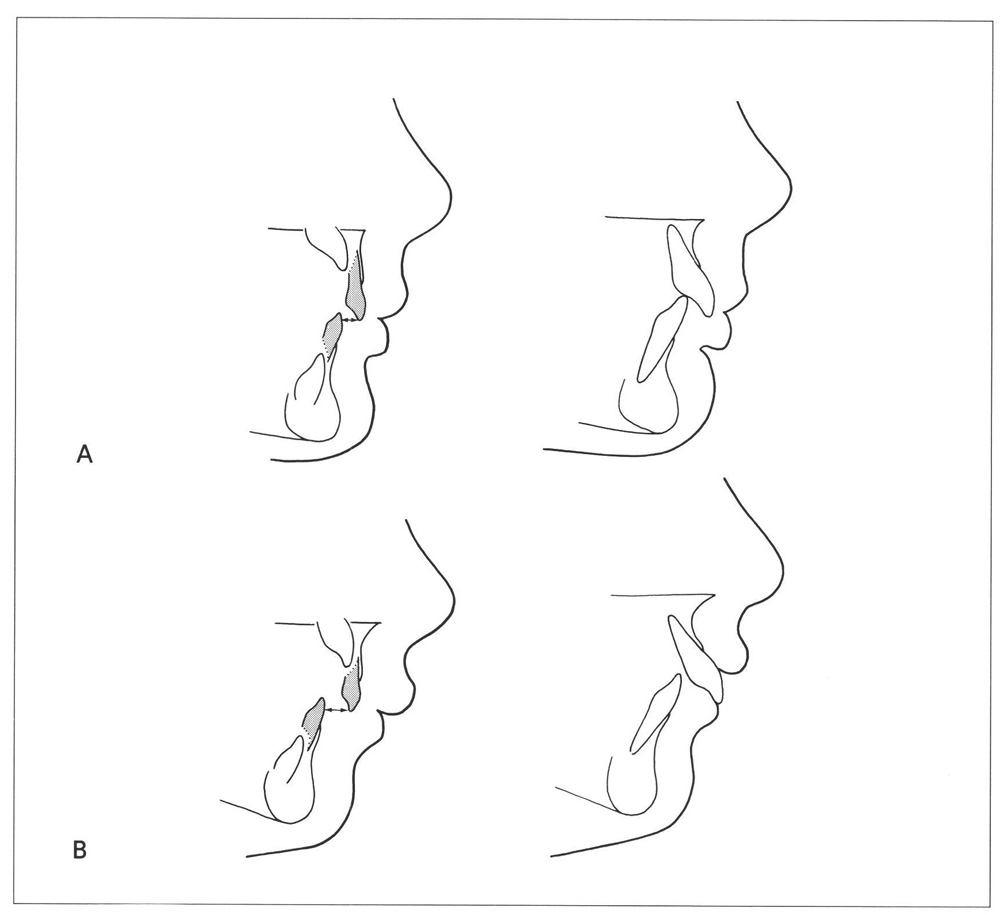
Fig. 12-2 Influence of craniofacial morphology on lip position in Class II/1 anomalies. (From Van der Linden.219)
A With a mild distorelation of the jaws, a shallow lower face height, and a low mandibular plane angle, a closed lip relation will usually remain after incisor transition.
B With a pronounced distorelation of the jaws, an increased lower face height, and a steep mandibular plane angle there is a great likelihood that the lower lip will lie dorsal to the maxillary incisors after incisor transition.
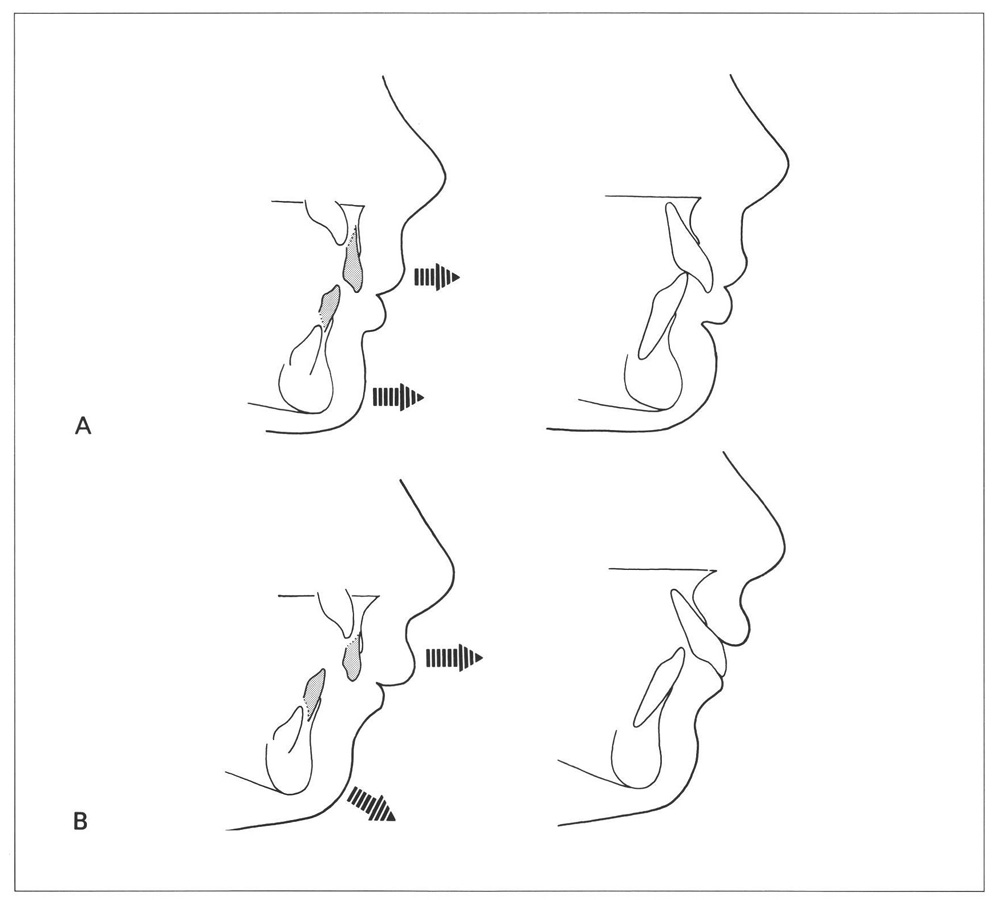
Fig. 12-3 Influence of facial growth direction on lip position in Class II/1 anomalies. (From Van der Linden.219)
A Where growth of the lower face is principally horizontal, and where the mandible grows more ventrally than the maxilla, a closed lip posture will remain after incisor transition.
B Where the growth of the face is more vertical, the lower lip can come to rest dorsal to the maxillary incisors, particularly when the mandible grows less ventrally than does the maxilla.
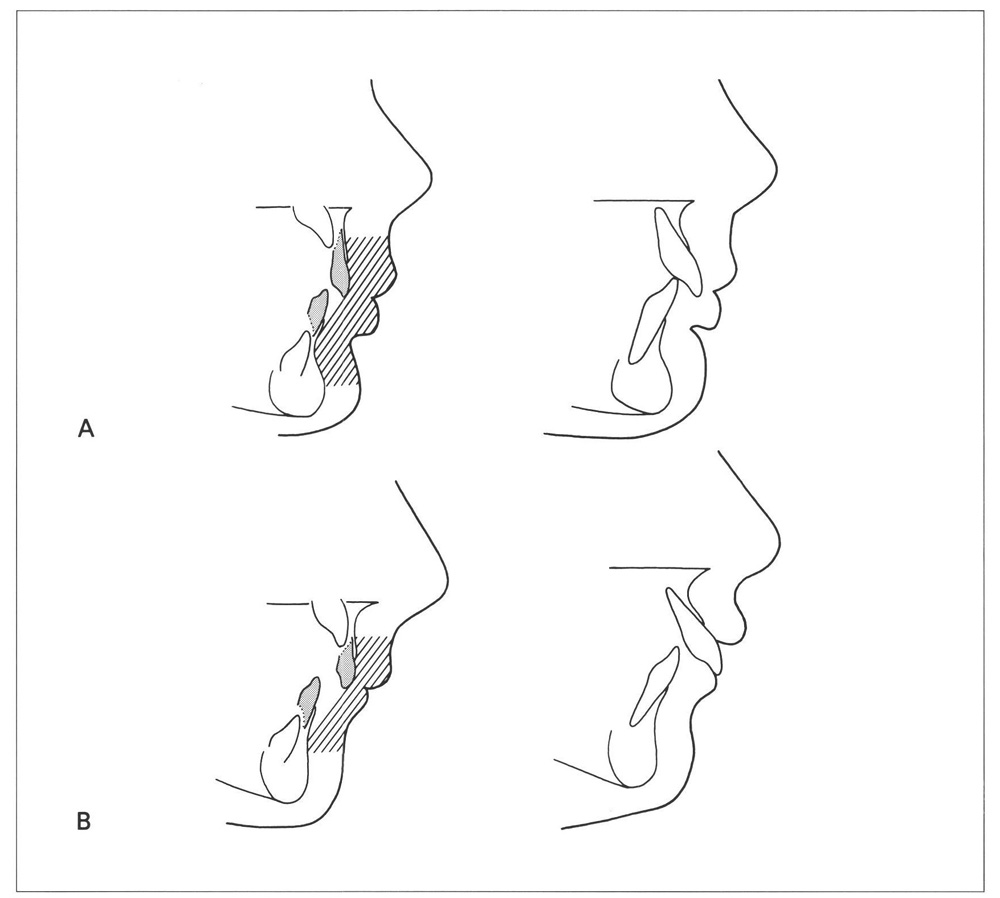
Fig. 12-4 Influence of the bulk of lip tissue on lip positions in Class II/1 anomalies. (From Van der Linden.219)
A Children with voluminous lips will continue to cover their permanent maxillary incisors with their lips even though they have assumed a more labial position than their predecessors.
B If the lips are proportionately short and thin, the tendency for the lower lip to fall behi/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


