Chapter 16
Impression Materials: Classification and Requirements
16.1 Introduction
Many dental appliances are constructed outside the patient’s mouth on models of the hard and/or soft tissues. The accuracy of ‘fit’ and the functional efficiency of the appliance depends upon how well the model replicates the natural oral tissues. The accuracy of the model depends on the accuracy of the impression in which it was cast.
The impression stage is the first of many stages involved in the production of dentures, crowns, bridges, orthodontic appliances etc. It is of great importance, therefore, that inaccuracies are minimized at this stage, otherwise they will be carried through and possibly compounded later on.
Impression materials are generally transferred to the patient’s mouth in an impression ‘tray’. The tray is required because the materials are initially quite fluid and require support. Once positioned in the patient’s mouth, the materials undergo ‘setting’ by either a chemical or physical process. After ‘setting’, the impression is removed from the patient’s mouth and the model cast using dental plaster or stone.
16.2 Classification of impression materials
Many criteria may be used to classify impression materials. The most widely used and understood method is to classify them according to chemical type. Hence, we have silicone materials, alginates, etc. Most dentists are able to associate a material from a particular chemical group with a particular set of characteristics or properties which render it suitable for some applications but not for others. Other methods of classification are sometimes used and these may be based upon consideration of the properties of the materials either before or after setting.
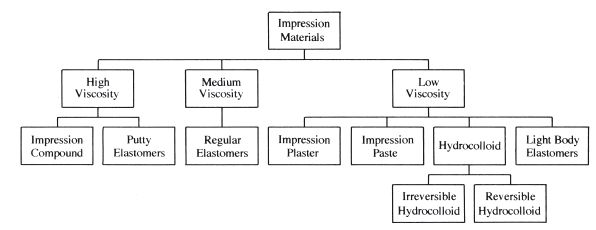
Before setting, the property most normally used to characterise materials is viscosity. This may effect the fine detail which can be recorded in impressions of hard tissues and may influence the degree of tissue compression or displacement achieved with soft-tissue impressions. Thus, materials which are initially very fluid are often classified as mucostatic impression materials because they are less likely to compress soft tissues, whilst materials which are initially more viscous are classified as mucocompressive. It should be remembered however, that viscosity often varies with the applied stress (p. 19). Thus, certain materials which appear fairly viscous whilst under low stress conditions may become more fluid during the recording of the impression, when the material is placed under higher stress. When a substance behaves in this way, it is said to be pseudoplastic. Another complicating factor is the spacing of the impression tray. This controls the thickness of the impression material and hence the pressure transmitted to the underlying tissues. A relatively fluid impression material confined in a close-fitting impression tray will compress the soft tissues to a greater extent than the same material used in a loosely-fitting tray. Classification of materials according to viscosity is not, therefore as simple as it may seem. Figure 16.1 gives a simplified classification according to viscosity in which materials with the highest viscosity are shown at the left of the figure and those with the lowest viscosity are shown on the right. There are often significant variations between different brands of the same type of material and these variations can spread across the divisions between different levels of viscosity.
Fig. 16.1 Classification of impression materials by viscosity at a constant shear rate and temperature (23°C).
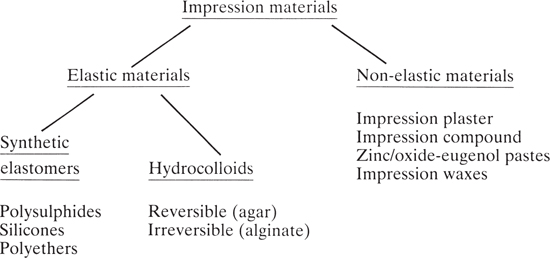
A more widely used classification of materials involves consideration of the properties of the set material. This factor is primarily responsible for governing the principal applications of the materials. The properties which are most important are rigidity and elasticity, since they determine whether an impression material can be used to record undercuts. When standing teeth are to be recorded, or when the patient has deep soft-tissue under-cuts, the set impression material must be flexible enough to be withdrawn past the undercuts and elastic enough to give recovery and an accurate impression. Hence impression materials are classified as being elastic or non-elastic. The term elastic as applied to impression materials is fairly unequivocal since the materials which form this group all possess the ability to be stretched or compressed and give a reasonable degree of elastic recovery following strain. They could be described as possessing rubbery characteristics. The term non-elastic however, is not a particularly good term with which to describe a group of products which in some cases are clearly plastic (e.g. impression waxes) and in other cases are very rigid but show little evidence of plastic deformation (e.g. impression plasters). It may be less confusing if the terms rubbery and non-rubbery were used instead of elastic and non-elastic. However, the latter terms have been used for many years and are therefore likely to be familiar to dentists.
Figure 16.2 lists the major groups of impression materials using the classification referred to above.
Fig. 16.2 Impression materials. Classification according to elastic properties and chemical type.
16.3 Requirements
The requirements of impression materials can be conveniently discussed under four main headings:
Accuracy
In order to record the fine detail of the hard or soft oral tissues, the impression material should be fluid on insertion into the patient’s mouth. This requires a low viscosity or a degree of pseudoplasticity.
The way in which the material interacts with saliva is another factor affecting fine-detail reproduction. Some products are hydrophobic and may be repelled by moisture in a critical area of the impression. This normally results in the formation of a ‘blow hole’ in the impression. For such products, a dry field of operation is essential. Other materials are more compatible with moisture and saliva and no special precautions are necessary.
The fine detail recorded in an impression will only be transferred to the gypsum cast if there is adequate ‘wetting’ of the impression surface by the freshly mixed dental stone or plaster. In cases where the impression is made from a hydrophobic material the hydrophilic slurry of calcium sulphate hemihydrate in water may not be able to approach closely enough to the surface of the impression (on a microscopic scale). This can result in blow holes and loss of fine detail. The ability of impression materials and gypsum products to reproduce detail in the cast is normally determined by measuring the contact angle which a drop of aqueous calcium sulphate solution makes with the surface of the impression material. A low contact angle is favourable as it indicates good wetting.
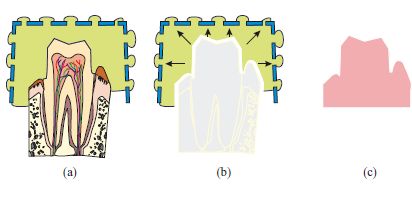
The ‘setting’ of impression materials, whether it involves a chemical reaction or simply a physical change of state, generally results in a dimensional change which, naturally, affects accuracy. For most materials, the dimensional change is a contraction and, providing the impression material is firmly attached to the impression tray, this produces an expansion of the impression ‘space’ and an oversized die, as illustrated in Fig. 16.3. Materials which expand during setting result in undersized dies or casts. The effect on the accuracy of fit of the resultant restoration depends on the type of restoration and the complexity of shape involved. For the simple crown preparation, illustrated in Fig. 16.3, the oversized die will result in a ‘loose-fitting’ crown. For greatest accuracy, the dimensional change should be minimal.
Fig. 16.3 Diagram illustrating the effect of setting contraction. (a) If the impression material is bonded to the tray, contraction occurs towards the tray. (b) Contraction results in an oversized impression space. (c) This results in an oversized die.
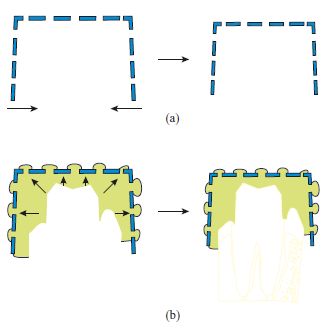
On being withdrawn from the patient’s mouth, which is typically at a temperature of 32–37°C, into the dental surgery, at a temperature of around 23°C, the impression undergoes approximately 10°C cooling. This results in thermal contraction, the magnitude of which depends on the value of coefficient of thermal expansion of the impression material and impression tray to which it is attached. It is difficult to calculate the precise value of the thermal contraction or to predict accurately the direction in which it operates since the contraction of the tray and that of the material act in opposite directions, providing the impression material remains attached to the tray. This is illustrated in Fig. 16.4. The effects of thermal changes are minimized if the values of coefficient of thermal expansion of the impression material and tray material are small.
Fig. 16.4 Diagram illustrating the effects of thermal contraction. (a) The tray contracts and reduces the impression space. (b) The impression material contracts towards the tray (providing it is bonded) and increases the impression space.
It is important that the impression material remains attached to the impression tray during the recording of the impression. Partial detachment may cause gross distortions of the impression which may remain undetected and will almost certainly lead to ill-fitting appliances or restorations. Manufacturers of impression materials often supply tray adhesives which are used to enhance bonding. Additional retention is achieved by using perforated trays.
In addition to the requirements given above, there are two further requirements which apply specifically to materials used for recording undercuts. These materials must have adequate elastic properties and adequate tear resistance, coupled with a rigidity which is low enough to enable the impression to be removed.
Figure 16.5 shows diagramatically the way in which a set material is placed under stress during the withdrawal of the impression. The thickest parts of the impression are compressed against the tray when they pass the widest part of the tooth crown. As the impression is withdrawn it is likely that the material is also subjected to tensile stresses as the trapped material is stretched. If a material is rigid after setting it may not be possible to remove it from undercut areas. This obviously has a negative effect on the ability to achieve an adequate impression, but more seriously may undermine the viability of the remaining teeth as they may be subjected to a considerable stress if an attempt is made to remove the impression.
Fig. 16.5 Diagram illustrating how an impression material is placed under stress during removal from an undercut area. (a) Impression in place before removal. (b) During removal – the impression material is subjected to both compressive and tensile stresses.
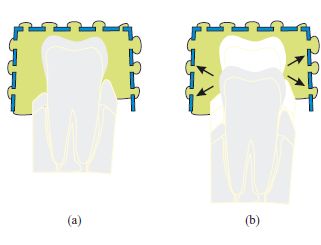
Figure 16.6 gives a series of diagrams to illustrate what happens when an impression of an undercut tooth is recorded with (a) an elastic material, (b) a plastic material, and (c) a viscoelastic material. The impression recorded with the elastic material accurately records the true shape of the tooth with the correct degree of undercut. The impression recorded with the plastic material has been grossly distorted during removal and has not recorded any undercut. The impression recorded with the viscoelastic material gives a distorted shape. The degree of distortion depends on the severity of the undercut, the thickness of the impression material and the time for which the impression is maintained in a compressed state (Fig. 16.5b) as well as the viscoelastic properties of the material itself. The behaviour of viscoelastic materials is described on p. 15–16, where the influence of time as an important parameter is discusse/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


