15 The maxillary antrum
ASSUMED KNOWLEDGE
It is assumed that at this stage you will have knowl-edge/competencies in the following areas:
INTENDED LEARNING OUTCOMES
At the end of this chapter you should be able to:
THE IMPORTANCE OF THE MAXILLARY ANTRUM TO DENTAL SURGERY
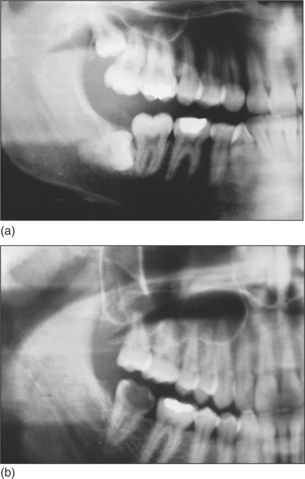
The maxillary sinus is often referred to as the maxillary antrum (or more simply the ‘antrum’). It is important to the dental surgeon because of its close relationship to the posterior maxillary teeth (generally from first premolar to third molar). The proximity varies between individuals (Fig. 15.1) but tends to increase with age as the antrum enlarges. The antrum can encroach into alveolar bone after tooth extraction, and periapical bone loss resulting from dental disease may further decrease the amount of bone separating it from the teeth. This close anatomical relationship can lead to diagnostic difficulties because both the antrum and the maxillary teeth are innervated by branches of the maxillary division of the trigeminal nerve. In addition, infection may spread from the periapical region of the posterior maxillary teeth to the antrum (and in the opposite direction) and the antrum is at risk of iatrogenic damage during certain dental procedures.
Summary of the importance of the maxillary antrum to dental surgery
DISTINGUISHING SIGNS AND SYMPTOMS OF DENTAL PATHOLOGY FROM THOSE OF SINUSITIS
Maxillary sinusitis is usually related to impaired antral drainage, which may be caused by:
Accumulated secretions become infected, allowing a collection of pus to develop in the antrum.
THE INVESTIGATION OF ANTRAL DISEASE
A diagnosis of sinusitis can usually be made from the findings of the history and examination. The teeth and surrounding tissues should be examined for disease (although remember that sinusitis may itself have a dental cause). Transillumination, using a torch shone from inside the mouth, may demonstrate antral congestion but this is a rather crude test and may fail to detect tumours. Radiographs are not usually required to confirm the diagnosis of sinusitis as the diagnosis can be made on clinical grounds alone. Radiographs are only required to exclude the possibility of dental disease, trauma or pathology within the antrum. If pathology or trauma is suspected, occipitomental radiographic views are often taken in specialist centres. A ‘fluid level’ may be visible which represents a collection of pus, although following trauma it may be due to the presence of blood and suggests that there is a fracture of the wall of the antrum. Opacities due to polyps, cysts, thickened antral lining, tumours and radio-opaque foreign bodies may also be demonstrated.
Other useful radiographs include:
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


