15
Orthodontics and Pediatric Dentistry: Two Specialties, One Goal
Summary
The pediatric dentist and orthodontist share many professional interests by virtue of the fact that they both are treating the same patient often on a regular and sustained basis. Furthermore, the treatment delivered by both specialties often has profound overall effects upon the function and esthetics of these young patients as they approach adulthood. Each clinician has the opportunity to support the other’s therapeutic efforts; however, there appears to be a significant ‘disconnect’ in treatment focus and inter-specialty communication and overall interactivity. Individual patient care suffers as the potential synergistic collaboration of the pediatric dentist and orthodontist is never fully realized. The ongoing sharing of new information between both specialties is critical, as is coordination of pediatric dental and orthodontic treatment. This chapter explores some of the existing problems of communication and inter-specialty interactivity. Several commonly encountered clinical scenarios are presented to illustrate these problems as well as to suggest changes in future pediatric dental and orthodontic education, clinical practice, and ongoing assessments of respective specialty guidelines.
Introduction
The pediatric dentist is a unique dental clinician as he or she is both a primary care dental health provider and specialist. As such, the pediatric dentist has an extraordinary responsibility in treating, triaging, and coordinating dental healthcare for infants, children, and adolescents. The pediatric dentist will most likely interface with the orthodontist on a daily basis far more than any other dental clinician for the obvious reason that many pediatric dental patients will be under the care of both clinicians during the same and often extended time period. Both the orthodontist and pediatric dentist will be applying therapies to their mutual patient and in many instances, these therapeutic decisions will impact on the immediate and long-term esthetic and functional status of their patient. It is the authors’ belief that new and more profoundly effective avenues of communication and interaction between the orthodontist and pediatric dentist need to be established and maintained if individual patients and the public at large are to benefit from modern orthodontic and pediatric dental care. Additionally, achieving meaningful and consequential interactivity and communication between both specialties will require a re-examination of orthodontic and pediatric dental postgraduate curricula as well as existing guidelines that have been established by each respective specialty.
Both specialties need to inculcate core information that crosses traditionally defined borders of academic and clinical interest. Some of these areas might include caries management, enamel decalcification, fluoride use, ectopic and impacted teeth, timing of orthodontic treatment, overall benefit of extraction strategies in orthodontic treatment, management of third molars, dental trauma, patient management, root resorption, and treatment options in cases of missing permanent teeth. Additionally, the pediatric dentist needs more core information on both evidence-based and evidence-‘bolstered’ information about a number of initial orthodontic strategies and midcourse orthodontic treatment changes that might become necessary as a result of adverse dentofacial growth and development and/or poor patient compliance. Similarly, the orthodontist should appreciate the incontrovertible value of faithful routine pediatric dental recall visits of patients undergoing active orthodontic treatment. Both clinicians require a new thinking of integrating ‘best evidence’ with clinical experience and individual patient or parental values. Finally, the orthodontist and pediatric dentist must establish mutually acceptable and practical communication protocols to ensure that any or all of these clinical insights will ultimately result in a consistently higher level of patient care for each individual patient. While it would be impossible for the authors to cover all of the aforementioned clinical situations that the orthodontist and pediatric dentist will encounter in the mixed dentition stage of dental development in one chapter, several commonly encountered clinical entities will be included in an effort to emphasize the importance of clinician interactivity between these two specialties.
Coordinating Orthodontic and Pediatric Dental Appointments in a Group or Solo Practitioner Setting
In order for the pediatric dentist and orthodontist to be optimally supportive of each other’s efforts, several conditions need to be met. An understanding of the overall emphasis of comprehensive care for the pediatric dental and orthodontic patient must be appreciated by both clinicians. Most important is the development and maintenance of ongoing communication paths, so that each clinician is maximally apprised of the treatment that might already be in progress and/or will be contemplated for the immediate or long-term future. There is a growing trend all over the world for the formation of consequential ethical professional partnerships or group types of practice that include the participation of pediatric dentists and orthodontists. One would think that such a consortium or association would facilitate streamlining communication efforts between the orthodontist and pediatric dentist. However, unless such group practices develop new and unprecedented communication avenues, the net result would be no better than what is observed in other types of traditional treatment settings in which the orthodontist and pediatric dentist frequently are virtually working independently in their own milieu, unaware of each other’s treatment plan and its progress.
A glaring, but rather basic example of this point is the pediatric dental recall visit schedule for patients undergoing orthodontic treatment. It is a frequent complaint of the pediatric dentist that some patients undergoing orthodontic treatment do not faithfully keep their regular pediatric dental recall appointments during the often-extended period of orthodontic treatment. The reason for this occurrence might be a misunderstanding of parents who mistakenly confuse monthly visits to the orthodontist as substitutes for semi-annual or annual visits to the pediatric dentist while their child is undergoing orthodontic treatment. The pediatric dentist might therefore be denied an opportunity to observe important developmental changes in the dentition and beyond during orthodontic treatment. It is the authors’ belief that the orthodontist should bear responsibility in assisting the pediatric dentist in ensuring that all patients are receiving regularly scheduled pediatric dental appointments during orthodontic treatment.
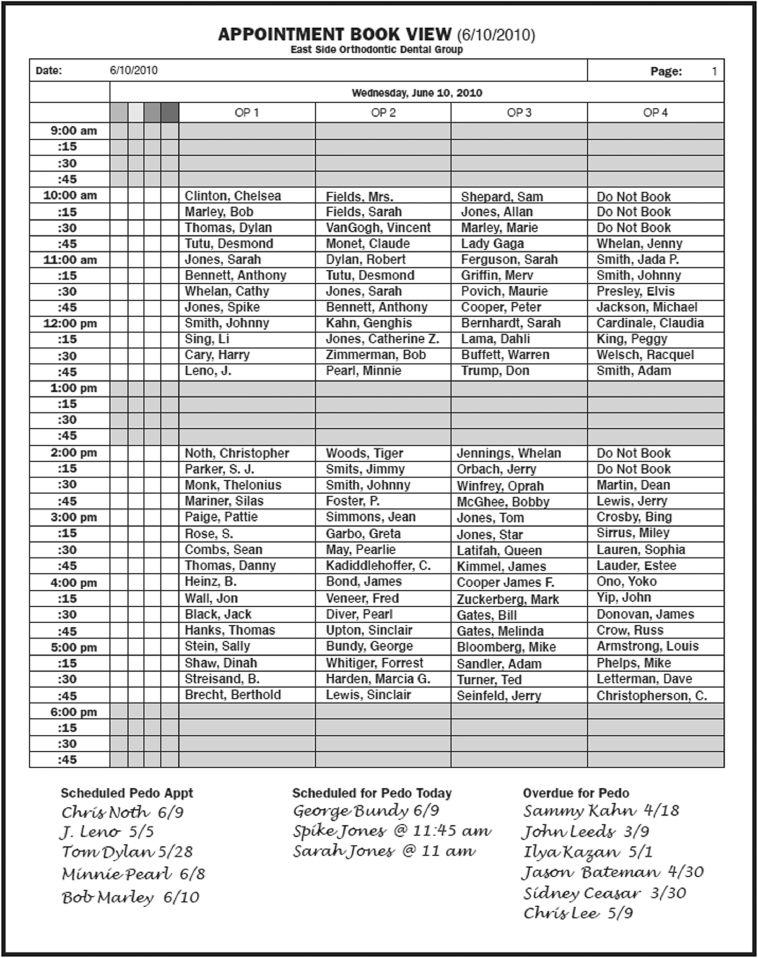
Figure 15.1 shows a typical orthodontic appointment schedule in a group orthodontic/pediatric dental practice. At the bottom of the page there are several columns that were derived from scheduling information supplied to the orthodontist from the pediatric dental section of the practice. The first column at the bottom of the page has a list of patients who will be seen by the orthodontist and already have pediatric dental appointments scheduled. This section is helpful in coordinating orthodontic treatment and pediatric dental treatment in the near future. For example, timely prescriptions (removal of primary or permanent teeth, oral hygiene recommendations and/or concerns, etc.) can be prepared in advance of the individual patient’s pediatric dental appointment. The second column has a list of patients who will also be seen by the pediatric dentist that particular day. This information may help overall pediatric dental concerns as posterior orthodontic bands can be removed, a thorough caries check can be performed, and the bands can be replaced that very same day. Additionally, oral hygiene concerns or any unusual in-treatment findings can be discussed directly with the pediatric dentist and dental hygienist. The third column shows patients who the orthodontist will be seeing, but are overdue for their pediatric dental appointments. It is perhaps, this particular column that is most important, for it identifies patients undergoing orthodontic treatment and who are not being seen by the pediatric dentist during the course of orthodontic treatment. Identifying these potentially ‘high risk patients’ gives the orthodontist an opportunity to have frank conversations with the parents of these patients about the importance of regular pediatric dental appointments during the course of orthodontic treatment, and encourage them to make pediatric dental appointments while they are being seen that day for their child’s orthodontic appointment. This protocol has greatly improved oral hygiene efforts and decreased the incidence of white spot lesions and any associated liability in our practice during orthodontic treatment, as the orthodontist, pediatric dentist, patient, and parent are optimally apprised of any adverse conditions during orthodontic treatment, and appropriate strategies (bolstered oral hygiene instruction, use of fluoride varnishes, etc.) can be administered on a regular and thoroughly coordinated basis.
Figure 15.1 Appointment schedule of an orthodontic/pediatric dental group, which faithfully tracks the individual orthodontic patient’s pediatric dental appointments during orthodontic treatment.
For those solo orthodontic practitioners who might be interested in a more proactive method of encouraging their patients to keep routine pediatric dental appointments during orthodontic treatment, a similar strategy can be employed. Figure 15.2 is a chart that the orthodontist sends to the pediatric dentist along with a note that the listed patients are under the care of the orthodontist, and Figure 15.3 is the returned chart with any of the patients listed who are overdue for their pediatric dental appointments. The orthodontist can now speak to the parents at their child’s next orthodontic appointment and inform them that one of the requirements of quality orthodontic treatment is to ensure that patient’s overall pediatric oral health needs are met during the course of orthodontic treatment. This single measure is well appreciated by the referring pediatric dentist and represents the orthodontist’s ‘team’ participation in the overall care of the orthodontic/pediatric dental patient.
Figure 15.2 A list of orthodontic patients (and their commencement date of active orthodontic treatment) who are also being treated by the pediatric dentist, Dr John Doe.

Figure 15.3 The returned list indicating which patients are overdue for their pediatric dental appointments.

Identifying Orthodontic and Pediatric Dental Problems Earlier Than Later
The pediatric dentist is often the first clinician to recognize malocclusions in the mixed dentition. Figure 15.4 is a chart that should assist the pediatric dentist and dental hygienist in quickly assessing any deviations from the ideal or norm and serve as a useful adjunct to the routine overall pediatric dental examination as well as an important vehicle of communication to the referred orthodontist. The orthodontist, similarly, can utilize this check-off assessment chart to further augment his or her traditional orthodontic examination and study of current orthodontic diagnostic records. The pediatric dentist should obtain a panoramic radiograph as an integral part of any initial orthodontic examination in the mixed dentition. Without the use of such a screening image, missing, supernumerary or ectopic teeth and a number of other salient underlying deviations and/or frank pathology will go unnoticed. Radiographs obtained by the pediatric dentist or orthodontist need to be shared so that each clinician is maximally informed at each juncture of patient assessment efforts. Routine yearly panoramic images obtained by the treating orthodontist should also be sent to the pediatric dentist. The modern age of digital or electronic capabilities make this a seamless routine for both clinicians and should be faithfully included in each other’s basic communication protocols.
Figure 15.4 Orthodontic status assessment chart that can be incorporated into the examination protocol of a pediatric dental practice.
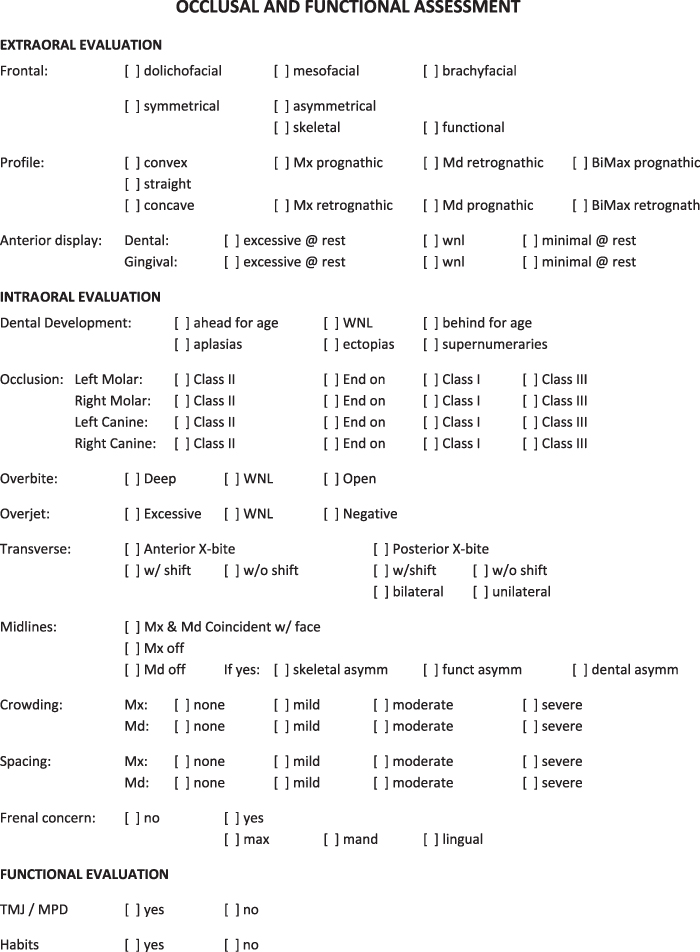
Figure 15.5 is a panoramic radiograph of a patient undergoing orthodontic treatment in the mixed dentition. Despite the less than average quality of this panoramic radiograph, the pediatric dentist viewing this radiograph noticed possible developmental caries in the mandibular second molars. Further specific periapical radiographs were then taken, the parents were apprised of this finding early on, and the matter was reassessed and managed after the eruption of the mandibular second molars. After confirmation of caries, the teeth were appropriately and conservatively restored (Figure 15.6). Figure 15.7 is an intraoral view of a patient, HW, in the mixed dentition, who, after examination by the pediatric dentist, was considered to have seemingly unremarkable orthodontic issues that would require later rather than earlier (i.e. orthodontic treatment in the permanent rather than mixed dentition stage) orthodontic treatment. The screening panoramic radiograph, however (Figure 15.8), suggested otherwise. The path of eruption of the canines and several other teeth was notably altered. There is considerable evidence, not only from the authors’ clinical observations, but from other investigators as well, to support the supposition that the majority of observed ectopically developing maxillary canines that are predisposed to becoming frank impactions can be conservatively managed by appropriate orthodontic intervention if such treatment is commenced earlier rather than later (Leonardi et al., 2004; Baccetti et al., 2009). HW was comprehensively treated utilizing maxillary expansion, removal of the maxillary primary canines, and fixed edgewise orthodontic appliances. Figure 15.9 is an in-treatment panoramic radiographic view and Figure 15.10 is an intraoral view of the maxillary canines mid-treatment and already well positioned into the dental arch. The overall pediatric dental and orthodontic management of this patient was considerably helped by the recognition of the benefits of panoramic ‘screening’ radiographs obtained in the mixed dentition for pediatric dental patients.
Figure 15.5 Panoramic radiograph obtained during the course of orthodontic treatment suggests developmental caries in the unerupted mandibular second molars.

Figure 15.6 Removal of caries and restoration of the mandibular second molars.
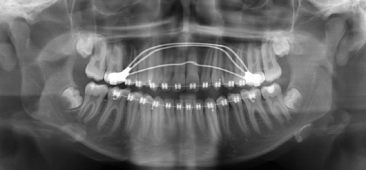
Figure 15.7 Intraoral view of a young patient (HW) undergoing a clinical examination, with what appears to be minor deviations from the expected ‘norms’.

Figure 15.8 Panoramic radiograph of HW revealed altered path of eruption of canine and other teeth.

Figure 15.9 In-treatment radiograph of HW with initial orthodontic objectives of redirecting the ectopic path of eruption of the maxillary permanent canines.
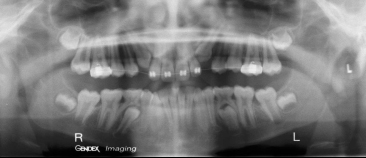
Figure 15.10 In-tre/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


