15 Lip Reduction (Reduction Cheiloplasty)
Lip augmentation was addressed in Chapter 14, and for thoroughness I thought that lip reduction and shortening, though much rarer procedures, should also be discussed. Lip enhancement is the mainstay of the minimally invasive portion of most cosmetic facial surgery practices, but not all patients seeking cosmetic lip enhancement desire larger lips. A few seek cosmetic consultation for lip reduction, and the cosmetic facial surgeon should be versed in this treatment option as well. In my personal experience, most patients presenting for lip reduction are of African American heritage, but I have performed this procedure on patients from other ethnic groups, including Caucasians. Of interest is the fact that I am now seeing Caucasian patients on a regular basis who have been overtreated with fat or permanent lip fillers and are requesting cosmetic lip reduction for iatrogenic macrocheilia.
Diagnosis and Consultation
Macrocheilia is defined as excessive lip size. Various ethnic groups share the characteristic of larger lips, including African American, Asian, and other groups (Figure 15-1), so for the remainder of this chapter, racial lip differences with larger lip anatomy will be referred to as ethnic lips. This would apply to lips that are larger than the Caucasoid lip and more frequently treated with cosmetic lip reduction, or reduction cheiloplasty.

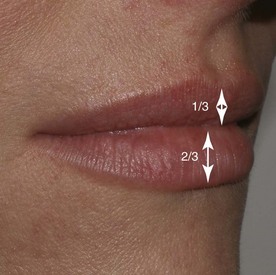
In the Caucasian patient, the upper lip constitutes a third of the total lip volume, and the lower lip constitutes about two-thirds, with a ratio of about 1 : 1.61,2 (Figure 15-2). African American lips are generally larger in all dimensions, and the upper and lower lip volumes are frequently nearly the same in many patients. Ethnic lips are also more protrusive, due in part to more soft-tissue mass. On average, chin and lip soft-tissue thickness is approximately 12 mm in Caucasians and 15 mm in African Americans.3 Vermilion height norms vary in different ethnicities: African American males have 13.3-mm upper lips and 13.2-mm lower lips, and African American females have 13.6-mm upper lips and 13.8-mm lower lips. North American Caucasian vermilion heights for upper and lower lips are 8.0 and 8.7 mm for males and 9.3 and 9.4 mm for females.4,5 Normally there is a 0 to 3-mm intralabial gap between the lips in repose. Patients with a larger intralabial space may not be good surgical candidates.
The importance of ruling out dentofacial deformities as contributing factors to macrocheilia cannot be overstressed, and orthodontic, oral, and maxillofacial consultation and a lateral cephalogram may be of assistance. Many African Americans exhibit a skeletal bimaxillary protrusion in which the angulation of maxillary and mandibular alveolar bone and teeth protrude anteriorly, influencing lip posture (Figure 15-3). If dentofacial abnormalities are not recognized, lip reduction may be contraindicated and worsen the cosmetic deformity by overly reducing lip size and exposing the dentofacial deformity. Microgenia can frequently accompany a bimaxillary protrusive profile, and the lack of chin prominence can make the lower lip appear larger.

Differential Diagnosis
Macrocheilia can be due to ethnic variation, dentofacial deformities (pseudomacrocheilia), pathology such as lymphatic disorders or hemangiomas, and medical disorders. Medical causes include Melkersson-Rosenthal syndrome, which is a rare neurologic disorder characterized by recurring facial paralysis, swelling of the face and lips (usually the upper lip), and development of folds and furrows in the tongue.6 Ascher’s syndrome is a rare disease first described in 1920 by an ophthalmologist by the same name. The disease is characterized by a double upper lip, blepharochalasis, and nontoxic thyroid enlargement.7 These two medical entities oftentimes go undiagnosed, and the astute surgeon should always consider systemic disease as a contributing factor. Additionally, some patients have lower-lip ptosis due to orbicularis oris dysfunction or central nervous system problems; orbicularis oris function should always be evaluated. Patients who cannot retract their lower lip or those with lip incompetence from poor muscle tone or other causes are not candidates for reduction cheiloplasty.
Lip Anatomy and Histology
The anatomy of the lip is very unique in that there is a triple transition from hair-bearing skin to vermilion tissue to oral mucosa. The hair-bearing skin terminates at the cutaneous/vermilion junction. The vermilion tissue consists of a very thin keratinized stratified squamous epithelium with extensive interdigitations with the underlying dermis (Figure 15-4). The vermilion is devoid of hair follicles, sweat glands, and sebaceous glands (although they may be sparsely present). The lack of sebaceous glands causes the vermilion to dry and crack, and hence the lips must remain moistened with saliva. The vermilion derives its color from the rich vascular plexus in the underlying dermis. This area is also highly sensitive, owing to its rich sensory innervation.
The thin, keratinized stratified squamous epithelium of the exposed vermilion transitions into a thick, nonkeratinized stratified squamous epithelium and becomes the intraoral mucosa (Figure 15-5). Under this thicker epithelium lies a submucosa containing numerous accessory salivary glands, including serous, mucous, and mixed seromucous glands.
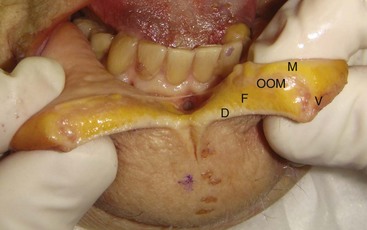
The bulk of the lip volume is made up of the circumoral orbicularis oris muscle, which blends laterally into the complex modiolus, a convergence of the perioral mimetic muscles. The orbicularis muscle lies more to the posterior region of the lip, curls over the vermilion surface, and ends at the vermilion/cutaneous junction.(Figure 15-6).
Lip-Reduction Procedure
Procedure
Reduction cheiloplasty has been described over the last 50 years by numerous authors from multiple countries.8–18 Like any procedure, many nuances exist from surgeon to surgeon, but in reviewing the literature, the basis of the described procedures are very similar and involve removing a fusiform or elliptical-shaped section of tissue and closing the defect to change the posture of the lip.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


