CHAPTER 15
Isolated Zygoma and Zygomaticomaxillary Complex (ZMC) Fractures
Christopher J. Haggerty
Private Practice, Lakewood Oral and Maxillofacial Surgery Specialists, Lees Summit; and Department of Oral and Maxillofacial Surgery, University of Missouri–Kansas City, Kansas City, Missouri, USA
Reduction of Isolated Zygomatic Arch Fractures
Reduction of the zygomatic arch to correct functional and cosmetic deformities.
Indications
- Loss of arch projection
- Comminuted arch
- Entrapment of the coronoid process (limited opening)
Contraindications
- Fractures over 20 days old; may require osteotomy
- Minimally displaced fractures with no symptoms
- Elderly and medically compromised patients
Quinn Approach to the Arch
- The procedure may be performed with local anesthetic alone, intravenous (IV) sedation, or general anesthesia.
- Local anesthetic is infiltrated within the tissue overlying the lateral ascending ramus and coronoid process.
- A #15 blade or electrocautery is used to initiate a 2–3 cm intraoral vestibular incision overlying the ascending ramus. Layers transected include mucosa, subcutaneous tissue, muscle, and periosteum.
- A periosteal elevator is used to elevate in a subperiosteal plane along the lateral aspect of the vertical ascending ramus and coronoid process.
- Through the intraoral incision, an instrument (Seldin retractor, urethral sound, and Henahan retractor) is placed between the coronoid process and the zygomatic arch.
- Lateral pressure is applied to the arch until the medially displaced arch is reduced (Figure 15.1).
- The oral mucosa is closed with resorbable sutures.
- An external splint (tongue blade, finger splint, or metal eye patches) may be fixated to the arch if desired.
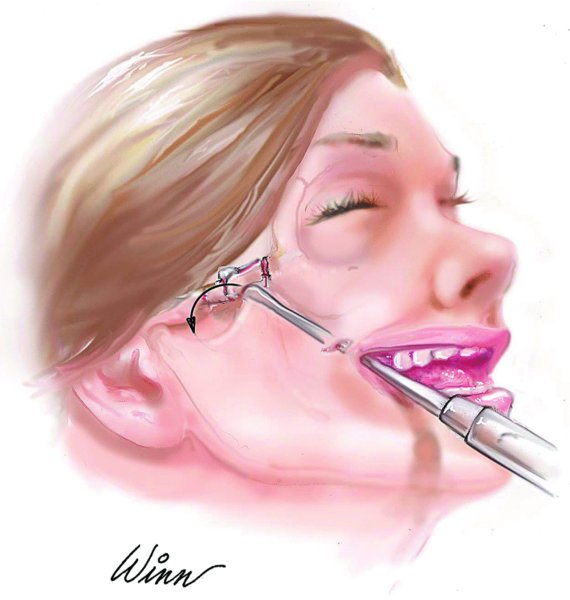
Figure 15.1. Quinn approach.
Gillies Approach to the Arch
- Preoperative antibiotics are used to cover contamination from skin or scalp flora. Preoperative steroids are administered to decrease postoperative soft tissue edema. General anesthesia is recommended.
- The patient is placed supine and rotated within a Mayfield headrest.
- After prepping and draping, the hair is parted, and a sterile marking pen is used to draw a 2–3 cm horizontal temporal line 3 cm inferior to the anterior temporal crest.
- Local anesthetic containing a vasoconstrictor is injected into the overlying tissue to aid in hemostasis.
- A skin incision is initiated with a #10 blade to the level of the temporoparietal fascia (superficial temporal fascia). A periosteal elevator or a Henahan retractor is used to dissect through the temporoparietal fascia to the glistening white temporalis fascia (deep temporal fascia) overlying the temporalis muscle.
- A horizontal incision is made through the temporalis fascia, and the temporalis muscle is exposed.
- Either a Rowe zygomatic elevator or a urethral sound is inserted between the temporalis muscle medially and the temporalis fascia laterally (Figure 15.2) until it reaches the medial aspect of the zygomatic arch.
- Lateral pressure is applied to the arch until the medially displaced arch is reduced (Figure 15.3).
- The incision is closed in a layer fashion.
- An external splint (tongue blade, finger splint, and metal eye patch) may be fixated to the arch if desired.
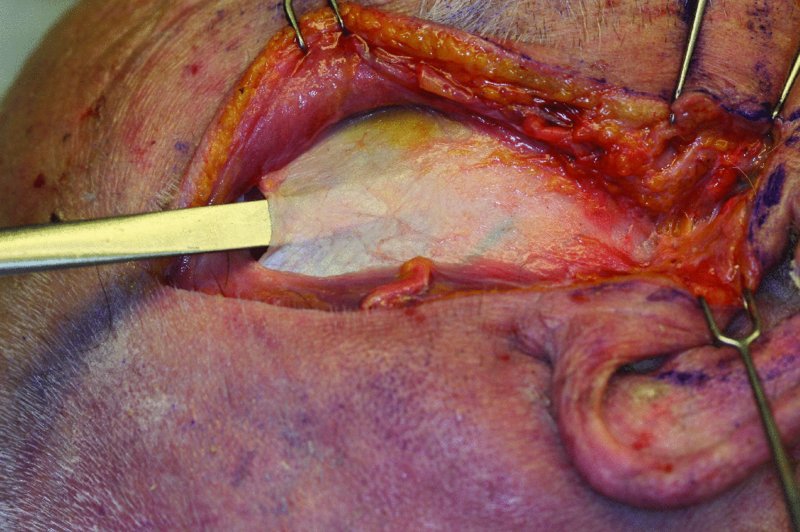
Figure 15.2. Cadaver dissection illustrating the placement of an instrument deep to the temporalis fascia (deep temporal fascia) and superficial to the temporalis muscle.
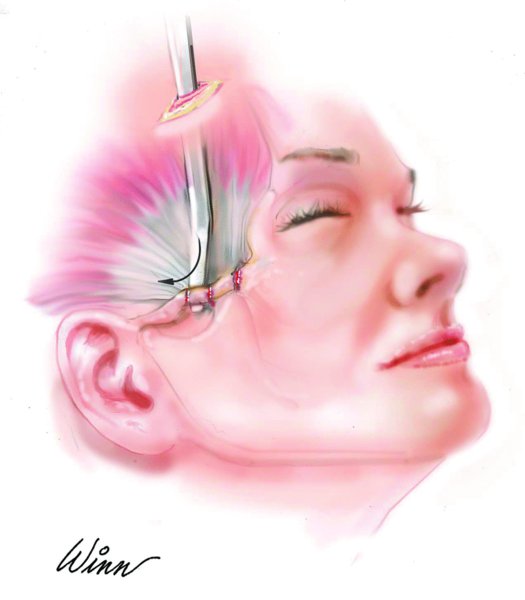
Figure 15.3. Gillies approach.
Reduction of Zygomaticomaxillary Complex Fractures
Reduction of the bones of the ZMC to reestablish facial projection, orbital volume, and aesthetics.
Indications
- Limited opening (trismus)
- Flattening of the malar eminence
- Flattening of the zygomatic arch
- Antimongoloid slant
- Enophthalmus
- Altered globe position
- Persistent anesthesia or paresthesia
- Superior orbital fissure (SOF) syndrome
- Extraocular muscle entrapment
Contraindications
- Fractures over 20 days old: may require osteotomy
- Minimally displaced fractures with no symptoms
- Blindness or open globe injury to the contralateral eye
- Traumatic hyphema; surgery typically delayed until hyphema resolves
- Elderly and medically compromised patients
Anatomy
The frontal branch of the facial nerve provides motor innervation to the frontalis, corrugators, and procerus and often to a portion of the orbicularis oculi muscle. Damage to the frontal branch results in the inability to raise the affected eyebrow or wrinkle the affected forehead. The path of the frontal branch can be identified by drawing a line from the tragus to a point 2.0 cm cephalic to the bony superolateral orbital rim. The frontal branch lies within or just deep to the temporoparietal fascia (superficial temporal fascia) and is in close proximity to the periosteum overlying the zygomatic arch (Figure 15.4). The frontal branch is often depicted as being contained within a box 0.8 cm to 3.5 cm (average 2.0 cm) anterior to the anterior extent of the external auditory canal.
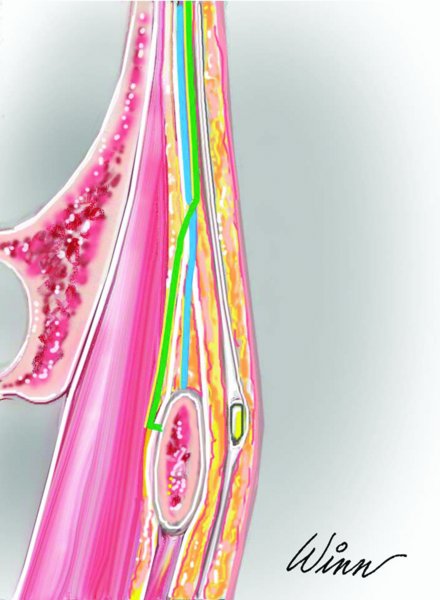
Figure 15.4. The blue line represents the subfascial approach and the green line represents the deep subfascial approach. Modified from Kenkere, D., Srinath, K.S. and Reddy, M., 2013.
Combined Maxillary Vestibular, Lateral Brow, and Transconjunctival Approach
- Preoperative antibiotics are used to cover contamination from sinus flora.
- The patient is placed supine within a Mayfield headrest. Ophthalmic ointment and corneal shields are placed bilaterally.
- After prepping and draping, local anesthetic containing a vasoconstrictor is infiltrated within the tissue overlying the zygomaticofrontal suture, the zygomaticomaxillary suture, and the inferior orbital rim from a transconjunctival approach.
- Maxillary vestibular incision: A #15 blade or electrocautery is used to initiate the intraoral maxillary vestibular incision (see Figure 15.5 in Case Report 15.1). Layers transected include mucosa, subcutaneous tissue, muscle, and periosteum. A periosteal elevator is used to expose the maxilla from the pterygoid plates laterally and to the pyriform aperture medially. Dissection proceeds cephalically and may include the inferior orbital rim if necessary.
- Lateral brow incision: Palpation over the lateral bony rim will reveal the zygomaticofrontal suture and fracture. An incision with either a blade or a needle-tip Bovie is concealed within the hair bearing portion of the lateral eyebrow and is carried down to periosteum (Figure 15.6, Case Report 15.1). Periosteal dissection continues along the lateral orbital rim and may be connected to the transconjunctival incision if desired, thus allowing access to the entire inferior and lateral orbital rim (Figure 15.7, Case Report 15.1). Alternatively, in females with a high arching lateral brow, a superior blepharoplasty incision may be used.
- Transconjunctival incision: A Bame or Desmarres retractor is placed to evert the lower lid, and a Jaeger or malleable retractor is used to place gentle posterior pressure on the globe itself. A blade is used to create a mucosal incision 2 mm posterior to the orbital septum and lateral to the medial puncta. A malleable retractor is used to retract the orbital fat as the orbital rim is approached. Care is taken to avoid damage to the inferior oblique muscle, which is located between the middle and nasal fat pads. Damage to this structure will result in diplopia and restricted ocular motility.
- Additional medial orbital wall exposure can be obtained by using a transcaruncular incision. A #15 blade is used to extend the original incision along the entire medial aspect of the orbital rim posterior to the inferior and superior puncta and canilicular system.
- Exposure of the entire lateral orbital wall can be obtained with a lateral canthotomy. Stevens scissors are inserted within the palpebral fissure deep to the conjunctiva of the lateral-inferior orbital rim. Layers transected include the skin, subcutaneous tissue, orbicularis oculi muscle, orbital septum, inferior limb of the lateral canthal tendon, and conjunctiva.
- With exposure of the fracture sites, fracture reduction is performed. For grossly displaced fractures or for fractures that are difficult to align, a Carroll–Girard screw can be inserted transorally or transcutaneously to engage the malar eminence. The Carroll–Girard screw provides excellent three dimensions control over the fractured ZMC and aids in the manipulation and reduction of the ZMC fractures.
- Prior to any plating, the reduced fractures are all visualized to ensure ideal reduction. The zygomaticosphenoid suture should be evaluated along the internal surface of the lateral orbital wall to ensure appropriate fracture reduction prior to employing rigid internal fixation.
- Displaced ZMC fractures are typically plated in the following sequence: the zygomaticofrontal suture (Figure 15.7, Case Report 15.1), the comminuted zygoma and/or zygomaticotemporal suture, the zygomaticomaxillary suture (Figure 15.8, Case Report 15.1), the orbital rim, and lastly the orbital floor–medial orbital wall (Figure 15.9, Case Report 15.1). Plating sequence variations exist dependent on individual surgeon preferences and the nature/displacement of the fractures.
- Following fracture plating, extraocular muscle function is evaluated for entrapment while the patient is under general anesthesia with a forced duction test. If any restrictions in extraocular mobility are detected, the fixation points should be reevaluated and adjustments made accordingly.
- All incisions are irrigated and closed in layers, and appropriate topical antibiotics and dressings are placed.
- If a lateral canthotomy was performed, the inferior limb of the lateral canthus is reapproximated, and a meticulous closure of the orbicularis oculi and skin follows. No sutures are required in closing the transconjunctival incision.

Figure 15.5. Le Fort I fractures and a fracture of the right zygomaticomaxillary buttress exposed via a maxillary vestibular incision.
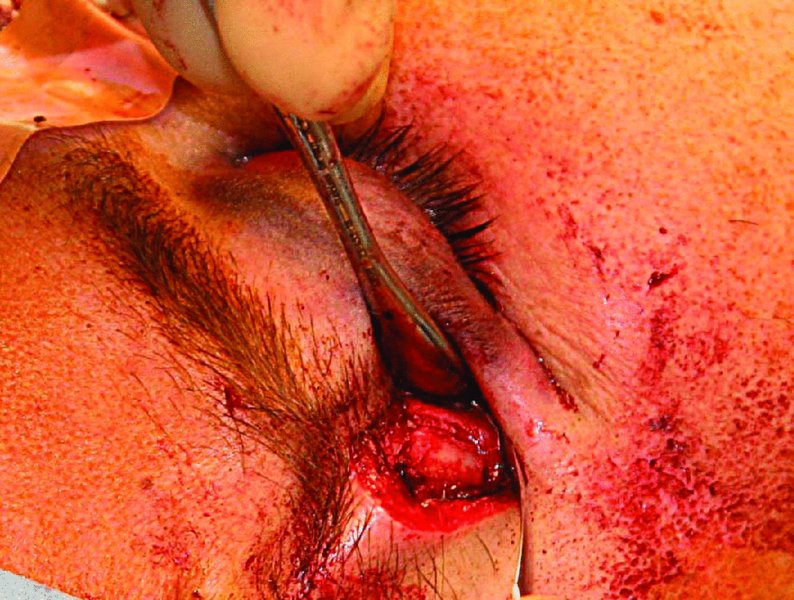
Figure 15.6. A lateral brow incision is used to expose the zygomaticofrontal suture.
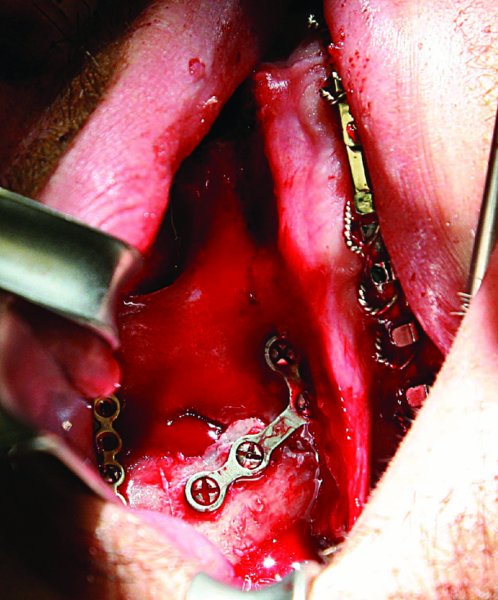
Figure 15.7. Intraoral plating of the zygomaticomaxillary buttress.
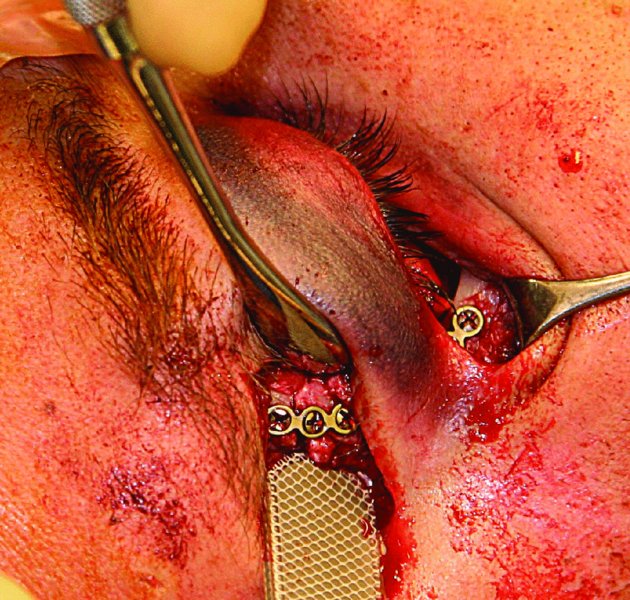
Figure 15.8. Plating of the comminuted lateral orbital rim. The lateral brow incision can be combined with the transconjuntival incision to allow for wide surgical exposure of the entire lateral orbital rim.

Figure 15.9. The inferior orbital rim and orbital floor/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


