Clinical Practice Guidelines for Developing Class III Malocclusion
Junji Sugawara
Class III malocclusion can be defined as a skeletal facial deformity characterized by a forward mandibular position with respect to the cranial base and/or maxilla (Fig. 15-1). This facial dysplasia can be classified as mandibular prognathism, maxillary retrognathism, or a combination of both, depending on the variation of the anteroposterior jaw relationships. Vertically, it can also be divided into three basic types depending on the vertical disproportions: long, average, and short face (see Fig. 15-1). In this chapter, Class III malocclusion will refer only to anteroposterior dysplasia. Class III malocclusion represents patients with anterior crossbite and a skeletal Class III jaw disharmony (Fig. 15-2). Pseudo–Class III malocclusion, which is characterized by an anterior crossbite and a skeletal Class I relationship, is excluded from this category.
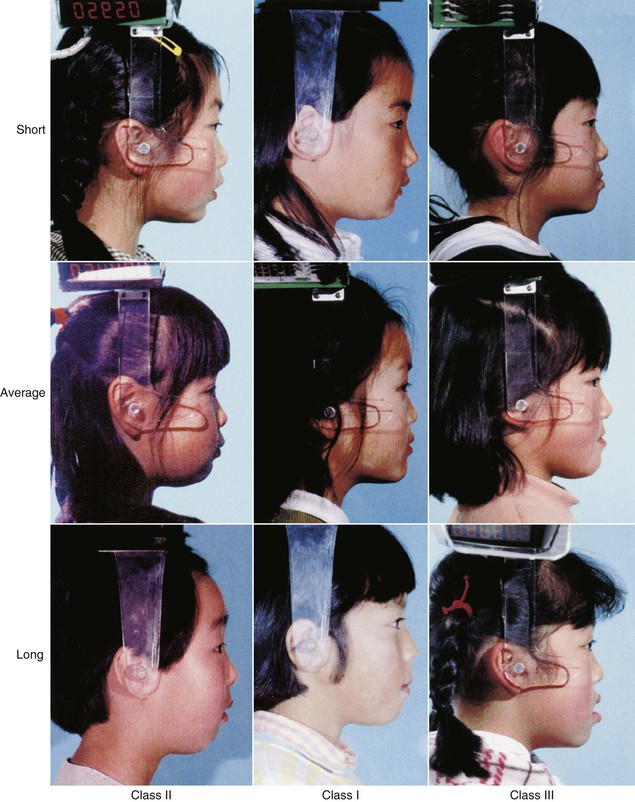
Figure 15-1 Classification of facial types.

Figure 15-2 Occlusion of each skeletal facial type.
It has been believed that Class III malocclusion may be caused by excessive growth of the mandible with respect to the maxilla and/or cranial base. However, the results of our longitudinal studies show similar maxillary and mandibular incremental changes during the prepubertal, pubertal, and postpubertal periods when compared to Class I subjects. Therefore it would be rational to assume that the skeletal framework of Class III malocclusion must have been established early before the prepubertal growth period. In addition, the manner of mandibular growth during the postpubertal period seems to be quite critical in Class III treatment, because the maxillary growth changes are almost negligible and only the mandible is displaced in a downward–forward direction according to its growth potential.
Concerning mandibular growth control that can possibly alter the skeletal framework of Class III patients, our aforementioned studies on the short-term and long-term effects of chin cap force indicate that the skeletal framework is greatly improved during the initial stages of chin cap therapy. However, such changes are rarely maintained during the pubertal growth period and, when growth is complete, results suggest that treatment with chin cap force seldom alters the inherited prognathic characteristics of Class III profiles.
Considering the scientific evidence, we have produced a clinical practice guideline for managing Class III patients and practiced in accordance with this guideline for more than 10 years. The principal role of the guideline is to make provisions so that almost all patients achieve functional occlusion and esthetic dentition until adulthood and lifelong stability thereafter. In addition, it aims to assure the quality of orthodontic treatment and to provide risk management strategies for unexpected situations occurring during treatment and management.
The clinical practice guideline for the correction of developing Class III malocclusion is outlined below, with particular consideration given to Class III facial growth and the long-term effects of chin cap orthopedic force for controlling Class III mandibular growth. In addition, treatment progress and the results of representative Class III patients who were managed in accordance with the clinical practice guideline are reported. Figure 15-3 shows the clinical practice guideline for growing and developing Class III patients and represents our present concept of their treatment and management.1
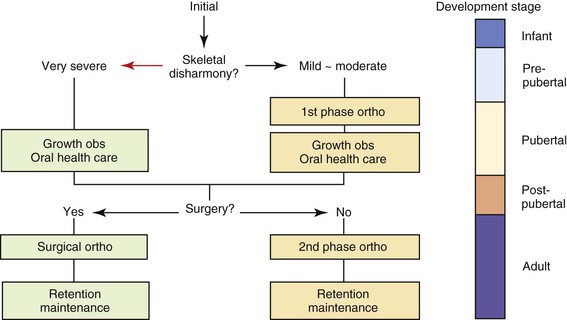
At the initial diagnosis in the deciduous dentition or early mixed dentition, patients receive a differential diagnosis and are divided into two groups according to the extent of their three-dimensional jaw disharmonies. Long-term management is usually recommended for patients diagnosed with mild or moderate skeletal Class III and this management is clearly separated into two treatment phases (see Fig. 15-3). The early mixed dentition is the most desirable time for the first phase of orthodontic treatment (although not all patients seek consultation early enough for this) and the second phase of treatment is generally applied during or after the postpubertal period. The growth observation period runs from the end of the first phase of treatment to the beginning of the second phase.
The treatment objectives of the first phase are:
1. To maintain good oral hygiene with the help of dental caries risk tests
2. To correct functional deviation of the mandible and to stabilize the jaw position
3. To improve the three-dimensional jaw deformity as much as possible
4. To correct and control the deviation of the dental midline
5. To accomplish desirable anterior occlusion for establishing anterior guidance in the future
6. To establish bilateral posterior support
In contrast, the treatment objectives of the second phase of treatment are:
1. To achieve a balanced soft tissue profile
2. To establish final functional occlusion
3. To regulate temporomandibular joint (TMJ) and oral functions
Patients with extremely severe skeletal Class III malocclusion, in whom orthognathic surgery is indicated, usually skip the first phase of treatment and their orthodontic problems cannot be addressed until the postpubertal period. It is important to collect growth data from these patients to establish an individual growth database that can be used to determine the timing of orthognathic surgery and to professionally control oral hygiene during the observation period.
Most Class III patients are managed according to one of the two pathways described above but occasionally a patient is managed in a modified manner. For instance, it is possible that patients diagnosed as requiring jaw surgery at the initial examination can be camouflaged with usual second-phase orthodontic treatment. Conversely, some patients may need to change from the right to the left side of the clinical practice guideline (see Fig. 15-3) if they experience abnormal jaw growth.
The reasons for proposing this clinical practice guideline for the correction of growing Class III malocclusion can be narrowed down to two points: Class III facial growth and chin cap orthopedic effects.
Class III Facial Growth
Most malocclusions and dentofacial deformities do not result from some pathological process but rather from a moderate distortion of normal development. Class III malocclusion appears to develop from an interaction between environmental and innate factors. An understanding of craniofacial growth behavior in Class III patients will help in determining the treatment timing and biomechanics. However, little is known about the craniofacial growth pattern of Class III malocclusion in comparison to normal patients. Early studies were largely based either on cross-sectional2 and semilongitudinal samples3 or on longitudinal data4,5 that encompassed too few subjects to be statistically valid.
In 1981 Mitani6 published a longitudinal study on Class III growth during the prepubertal period. Since then, our research group has conducted several longitudinal studies7–12 using the growth records of patients who were waiting for orthognathic surgery. The craniofacial growth of skeletal Class III Japanese female subjects during the prepubertal, pubertal, and postpubertal periods, which was one of the sources that informed the development of the clinical practice guideline, is shown in Figure 15-4.
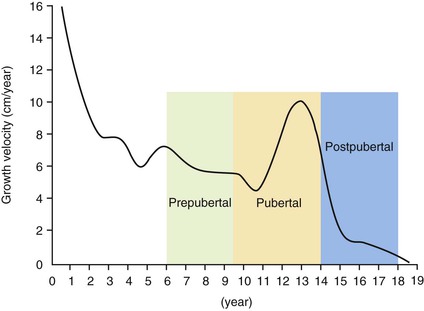
Figure 15-4 Growth curve showing the development stages.
Prepubertal Growth Period
Mitani6 compared growth changes between Class III and Class I patients during the prepubertal growth period. The investigation was based on two groups of Japanese girls: an experimental group of 18 girls (Class III group) and a control group of 22 girls (Class I group). Each set of serial lateral cephalometric head films consisted of a 4-year series from ages 7 to 10 years. All Class III subjects exhibited Class III malocclusion and all Class I subjects showed excellent or mild Class I malocclusion. None of the Class III subjects underwent any growth-related orthopedic treatment before or during the study period.
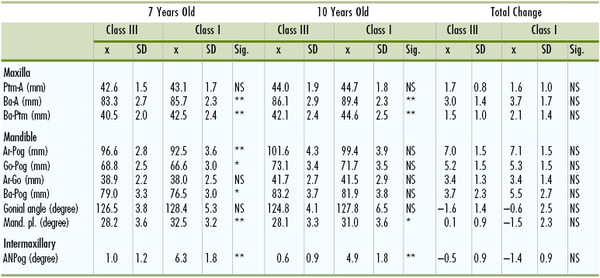
Table 15-1 shows mean and standard deviations of linear and angular measurements at the ages of 7 and 10 years and the overall changes during this period. No significant difference was found between the two groups with regard to the size of the maxilla (Ptm-A). However, the maxilla, as measured from basion to Ptm (Ba-Ptm), was more retruded among the Class III group (p <0.01). The incremental changes in both groups for these two measurements were relatively similar.
TABLE 15-1
Results of Measurements for Class III (n = 18) and Class I (n = 22) Groups During Prepubertal Growth Period in Japanese Females
* p <0.05.
** p <0.01.
A, A point; Ar, articulare; Ba, basion; Go, gonion; Mand. pl., mandibular plane; NS, not significant; Pog, pogonion; Ptm, pterygomaxillary fissure; SD, standard deviation; Sig., significance.
Reprinted with permission from Mitani H. Prepubertal growth of mandibular prognathism. Am J Orthod. 1981;80:546–553.
Comparison of the annual size increase in the mandible showed that the total mandibular length (Ar-Pog) of the Class III group maintained greater values than the Class I group until the age of 10 years. There was no significant difference between the means of the two groups for the total incremental changes in any measurements.
The ANPog angle showed a significant difference in facial convexity between the two groups. The amount of reduction in convexity was slightly greater in the Class I group than in the Class III group with age but there was no significant difference between the two groups.
In conclusion, skeletal Class III malocclusion showed an incremental growth change similar to the Class I group during the prepubertal period. These results suggest that the morphological pattern of the prognathic face associated with mandibular excess is probably established in early life. Once established, the annual growth increment is quite similar to that in an individual with a normal or Class I face before puberty.
Pubertal Growth Period
Bandai et al.12 reported on the craniofacial growth pattern of skeletal Class III malocclusion during the pubertal growth period (9 to 14 years) in Japanese girls. The Class III group comprised 16 Class III girls selected from patients waiting for surgical orthodontic treatment. All patients exhibited a large reverse overjet and none underwent orthodontic or growth-related orthopedic therapy before or during the study period. The Class I group comprised 18 Class I girls who served as control subjects. A few of these patients underwent first-phase orthodontic treatment for the alignment of incisors only. The pubertal growth peak of all subjects, which was individually evaluated by ossification events of hand-wrist roentgenograms12,13 and the incremental curve of body height,14 was observed around the middle of the period studied. Serial lateral cephalometric head films were used over a period of 5 years from 9 to 14 years of age.
Table 15-2 shows the mean and standard deviations of linear and angular measurements at the ages of 9 and 14 years and the overall changes during this period. Figure 15-5 depicts the longitudinal changes of the skeletal profile in each group. These skeletal profiles were constructed with 13 cephalometric landmarks measured in terms of the x–y coordinates.
TABLE 15-2
Measurements for Class III (n = 16) and Class I (n = 18) Groups During Pubertal Growth Period in Japanese Females
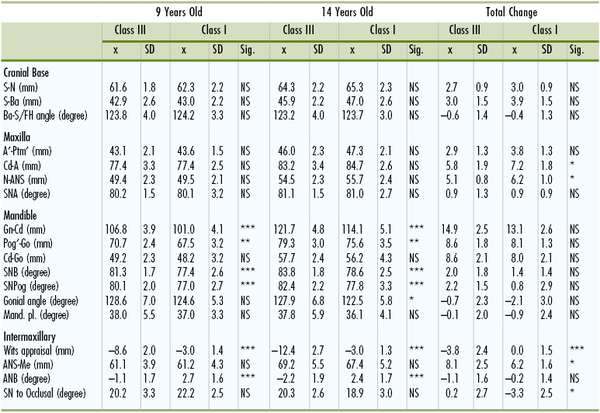
* p <0.05.
** p <0.01.
*** p <0.001.
A, A point; ANB, A point nasion B point; ANS, anterior nasal spine; Ba, basion; Gn, gnathion; Go, gonion; Mand. pl., mandibular plane; Me, menton; N, nasion; NS, not significant; Pog, pogonion; Ptm, pterygomaxillary fissure; S, sella; SD, standard deviation; Sig., significance; SN, sella-nasion; SNA, sella-nasion A point; SNB, sella-nasion B point.
Reprinted with permission from Bandai (Sakamoto) E, Sugawara J, Umemori M, et al. Craniofacial growth of mandibular prognathism in Japanese girls during pubertal growth period: longitudinal study from 9 to 14 years of age. Orthod Waves. 2000;59:77–89.
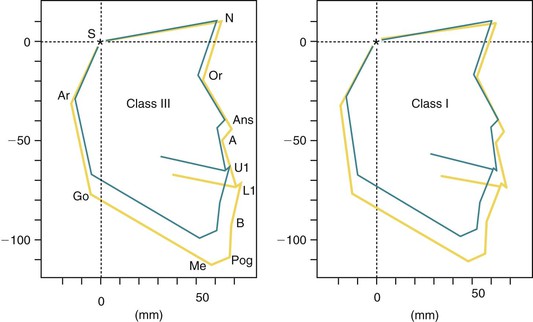
Figure 15-5 Longitudinal changes in the skeletal profiles of Class III and Class I groups. A, A point; Ans, anterior nasal spine; Ar, articulare; B, B point; Go, gonion; L1, lower incisor; Me, menton; N, nasion; Or, orbitale; Pog, pogonion; S, sella; U1, upper incisor.
No significant difference between the two groups was found in the total increase of any cephalometric measurements or in any measurements regarding the maxilla at ages 9 and 14 years. Although the midfacial length (Cd-A) and upper facial height (N-ANS) of the Class III patients were significantly smaller (p <0.05) than those of the Class I group, the average incremental changes in the maxillary length (A′-Ptm′) showed no significant difference between the two groups.
The mean values of the total mandibular length (Gn-Cd) and the body length (Pog′-Go) of the Class III group were significantly greater (p <0.001) than those of the Class I group, whereas the ramus height (Cd-Go) was not. The average mandibular growth changes measured at Gn-Cd were 14.9 mm in the Class III group and 13.1 mm in the Class I group, showing no significant difference between the two groups.
The principal skeletal frameworks of the two groups were maintained during the pubertal period. The occlusal plane angle (SNOP) of Class III subjects remained unchanged. However, in Class I subjects it showed counterclockwise rotation during this growth period. There was a significant difference (p <0.001) in the total change of Wits appraisal between the two groups.
In conclusion, Class III malocclusion showed neither excessive mandibular growth nor deficient maxillary growth when compared to Class I subjects during the pubertal growth period. The skeletal malocclusion seems to have been established before the pubertal growth period and maintained thereafter. Meanwhile, the dentoalveolar disharmony is aggravated and becomes more severe during this period, as shown by the difference in occlusal plane angle and the Wits appraisal.
Postpubertal Growth Period
Several studies7–10 have reported on the craniofacial growth pattern of Class III malocclusion during the postpubertal period using longitudinal data. Mitani et al.10 studied the serial lateral cephalometric head films of skeletal Class III and Class I malocclusion in Japanese females over a period of 3 years during the postpubertal period. Cephalograms were taken at the age of 14 and 17 years. The Class III group comprised 20 female subjects selected from a file of patients waiting for surgical orthodontic treatment and 20 female subjects were used as control. The criteria for case selection were the same as in the studies described above, with the exception of maturational stage. Maturational stages and physiological ages of all subjects were evaluated individually by the ossification events taken from hand-wrist radiographs.13–17
Table 15-3 shows mean and standard deviations of linear and angular measurements for female subjects. During the observation period, a comparison of the maxillary measurements showed that neither the size (Ptm-A) nor the position (SNA, Ba-Ptm) of the maxilla showed any significant difference between the two groups. The total change in maxillary measurements also showed no significant difference between the two groups.
TABLE 15-3
Results of Measurements for Class III (n = 20) and Class I (n = 20) Groups During Postpubertal Growth Period in Japanese Females
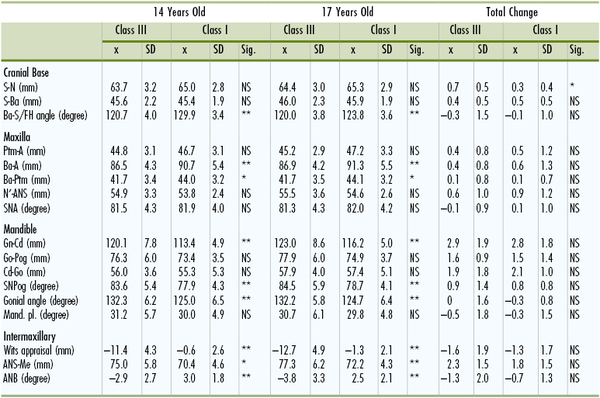
* p <0.05.
** p <0.01.
A, A point; ANB, A point nasion B point; ANS, anterior nasal spine; Ba, basion; Gn, gnathion; Go, gonion; Mand. pl., mandibular plane; Me, menton; N, nasion; NS, not significant; Pog, pogonion; Ptm, pterygomaxillary fissure; S, sella; SD, standard deviation; Sig., significance; SNA, sella-nasion A point.
Reprinted with permission from Mitani H, Sato K, Sugawara J. Growth of mandibular prognathism after pubertal growth peak. Am J Orthod Dentofacial Orthop. 1993;104:330–336.
Comparison of the mandibular measurements showed that the total lengths (Gn-Cd) of the Class III group were significantly greater than those of the Class I group, whereas the ramus height (Cd-Go) and the body length (Go-Pog) exhibited no significant difference between the two groups. There was no significant difference between the two groups in any of the changes in mandibular measurements during the time periods studied.
No significant difference was observed between the two groups in the total changes in A point nasion B point (ANB) angle and Wits appraisal. Differential growth between the maxilla and the mandible was observed in each group but the changes were minimal. The skeletal frameworks of the two groups were maintained during the postpubertal period.
In conclusion, the Class III group showed an incremental growth change similar to the Class I group. The morphological characteristics of the skeletal Class III malocclusion are maintained during the postpubertal period.
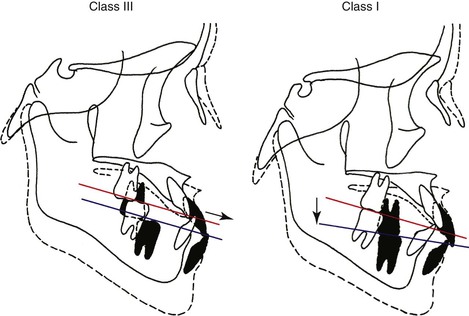
Clinical Implications
The results of our longitudinal studies6–12 on Class III facial growth suggest that Class III malocclusion is established early and before the prepubertal growth period. The authors11,12 speculated the reason why Class I subjects with growth changes similar to those of Class III subjects could maintain a normal occlusion. This phenomenon may be attributed to the rotational change of the occlusal plane (Fig. 15-6). Namely, in the Class I group the occlusal plane is displaced in a downward-forward direction with counterclockwise rotation. Therefore the anteroposterior relationship between the bimaxillary apical bases evaluated on the occlusal plane (Wits appraisal) is harmoniously maintained despite differential jaw growth. However, in Class III subjects the amount of maxillomandibular differential growth is not compensated for by the counterclockwise rotational change of the occlusal plane. The dentoalveolar disharmony evaluated by Wits appraisal is significantly aggravated due to lack of homeostasis of the neuromuscular system, which functions to maintain a stable intercuspal position in normal occlusion. These results may point to the benefit of early orthodontic intervention that may minimize the amount of apical base discrepancy that seems to be aggravated with growth.
Orthopedic Effects of Chin Cap Therapy
The orthopedic effects of chin cap appliances, which were thought to improve facial growth in Class III patients with mandibular excess, became the object of orthodontists’ attention in the 1960s. Since then, chin cap therapy has been widely recognized as a method for treating developing Class III malocclusion in young patients. A number of clinical and experimental studies2,17–26 have reported that chin cap force has several short-term orthopedic effects: (1) redirection of mandibular growth, (2) backward repositioning of the mandible, (3) retardation of mandibular growth, and (4) remodeling of the mandible and the TMJ.
Sugawara et al.27 reported long-term growth changes in patients treated with chin cap therapy at different ages and with various treatment schedules. The possibility that these effects may induce permanent skeletal changes and alter the prognathic skeletal profile, particularly when applied at an early age,20,28 has kept attention on chin cap therapy. However, little is known about whether the improved skeletal profile can be maintained until craniofacial growth is complete. Most studies have been based on either relatively short-term results that are of too short a duration to determine the final result or long-term results that encompass too few subjects to be statistically valid. The short-term and long-term results of chin cap therapy on the developing Class III malocclusion are reviewed below.
In this study it was hypothesized that (1) early application of chin cap force is more effective for correction of skeletal discrepancies and (2) the short-term effects of chin cap therapy are maintained after complete growth. This study involved 63 Japanese girls who showed anterior crossbite and Class III skeletal pattern before treatment and who were divided into three groups according to their age at the start of chin cap therapy: age 7 (before the pubertal growth spurt), age 9 (/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


