CHAPTER 15 Case Presentations
Management of Complications
Management of Failed Immediately-Loaded Zygomatic Implants
A 64-year-old woman presented with no restorable mandibular dentition and an ill-fitting maxillary full denture. The clinical and radiographic studies demonstrated multiple periodontally involved and nonrestorable teeth. The panoramic study demonstrated advanced resorption of the maxillary alveolar bone and residual alveolar bone in zone I only. The patient’s priority was treatment of the mandibular arch. After fabrication of a full mandibular denture, the mandibular teeth were removed; mandibular implants were placed immediately and the mandibular denture was converted into an immediate-load mandibular provisional, implant-supported bridge. After 3 months of osseointegration, the mandibular implants were checked for the presence of osseointegration and the final profile prosthesis was fabricated and delivered (Figures 15-1 to 15-3).

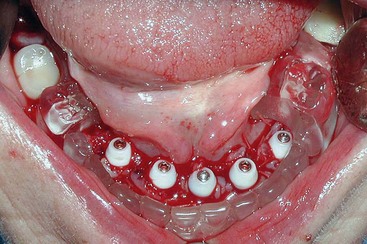
Five years after treatment of the mandible, the patient requested treatment of her maxillary arch with an implant-supported fixed bridge. Because of the presence of zone I bone and an inadequate volume of zones II and III bone, the zygomatic treatment method was used. Using the protocol for the zygomatic method, two premaxillary implants and two zygomatic implants were placed and the patient’s full maxillary denture was converted to a provisional, immediate-load prosthesis (Figures 15-4 to 15-7).
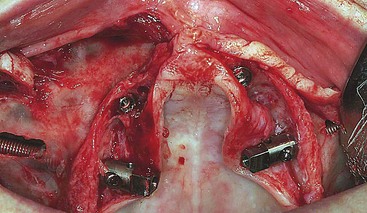
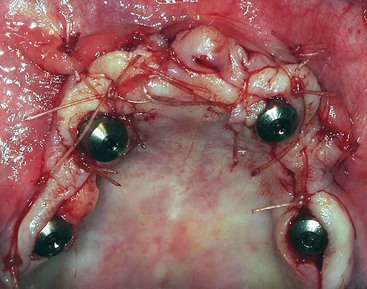



FIGURE 15-7 Completed conversion of the full maxillary denture into an immediate-load maxillary provisional prosthesis.
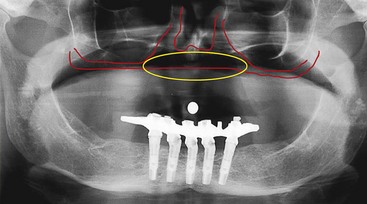
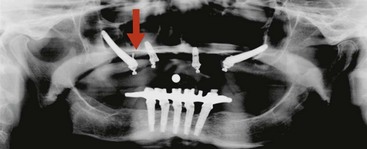
In preparation for replacement of the failed zygoma implant, reformatted views of the patient’s cone beam radiographic study demonstrate the availability of bone above the existing implant. The intention of the procedure was to remove the failed implant, with immediate placement of a new zygoma implant with the apex in the os zygomaticus and above the failed implant apex (Figures 15-8 to 15-16).

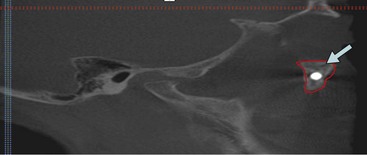
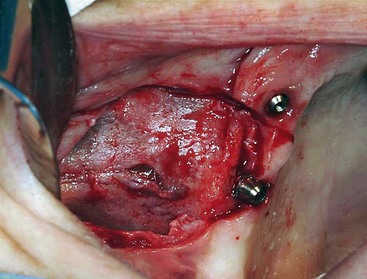


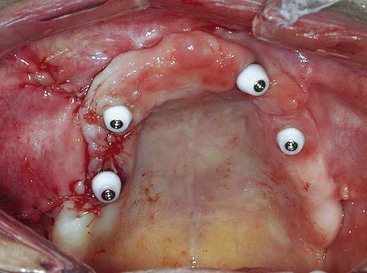
FIGURE 15-15 Closure of the soft tissues after connection and torquing of a new multiunit abutment at 35 Ncm.
To reconnect the immediate-load provisional prosthesis to the new implant, the existing right posterior maxillary titanium cylinder was removed. The provisional prosthesis was connected to the existing three implants by their retention screws and the new implant was “salt and peppered” to the new titanium cylinder. The patient was discharged with the corrected prosthesis. An additional 6 months of osseointegration was allowed prior to checking the right maxillary implant for osseointegration. After osseointegration of all four implants was confirmed, the final metal-based profile prosthesis was fabricated (Figures 15-17 to 15-22).

Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


