CHAPTER 14 Pediatric Dentistry
Dentistry for Children
Pediatric dentistry has evolved because of the special psychological challenges of children and the occasional peculiar clinical conditions that are present in children. most dentistry performed for children is rendered by general dentists, but many situations are treated best by a pediatric dentist (children’s specialist). your general dentist can advise you on whether your child should see a pediatric dentist, or you may prefer to find a pediatric dentist just because most of them have practices that are oriented completely toward the special needs of children.
WHAT YOU SEE OR FEEL
Conditions, Signs, or Symptoms Related to Pediatric Dentistry
1. Holes in Primary (Baby) Teeth, Often Discolored (Black, Gray, Brown, Yellow, Chalky)
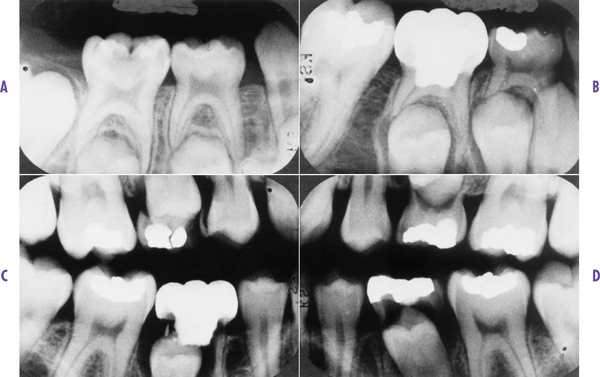
(FIG. 14.1). Dental caries (decay) in children is similar to adult tooth decay. However, in children the disease may be in the primary (baby) teeth. These smaller teeth do not have a great amount of enamel on them, and the decay process can progress rapidly. When decay is found at an early stage, typical fillings can be placed in the primary teeth with reasonable assurance of years of longevity. When dental caries has progressed to involve the dental pulp (nerve) (FIG. 14.2), either a root canal can be done on a permanent tooth (p. 40), or a pulpotomy (p. 124) can be done on a primary tooth.

FIG. 14.1 Decayed primary (baby) teeth.
(From Cameron A, Widmer R: Handbook of pediatric dentistry, London, 1997, Mosby-Wolfe.)
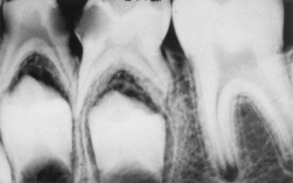
FIG. 14.2 Tooth decay with pulp (nerve) involvement. Note dark holes in teeth.
(From McDonald RE, Avery DR: Dentistry for the child and adolescent, ed 7, St Louis, 2000, Mosby.)


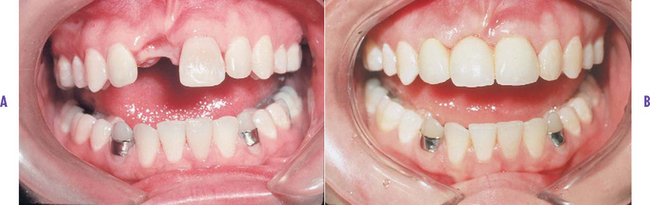
FIG. 14.4 Tooth restoration in the front teeth of an adolescent. You can’t tell which teeth are restored.

FIG. 14.5 Stainless steel crowns (caps) are unpleasant in appearance, but they serve well.
(From Mcdonald RE, Avery DR: Dentistry for the child and adolescent, ed 7, st Louis, 2000, Mosby.)
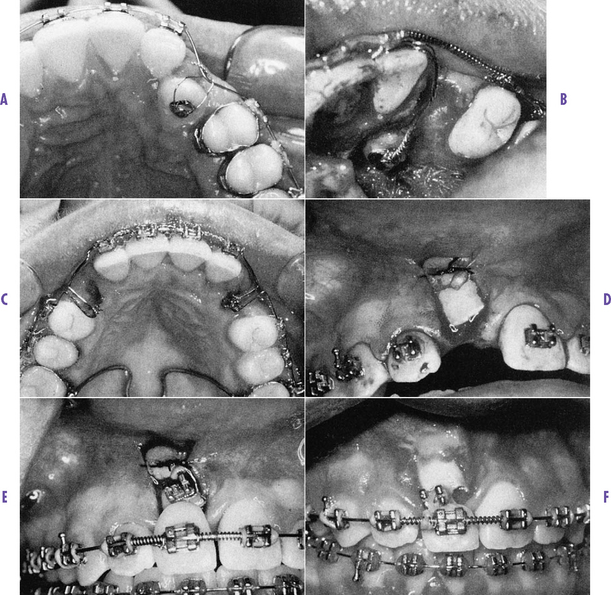
2. Permanent Tooth Won’t Erupt (Come into Mouth)
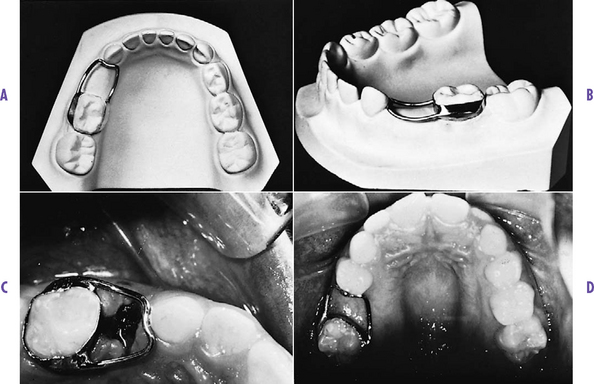
(FIG. 14.8). After the primary teeth exfoliate (come out), the permanent teeth are usually present within a few days or weeks. However, permanent teeth occasionally are slow to come in for several reasons: premature loss of primary teeth stimulated by trauma; abnormal positioning of permanent or primary teeth, not allowing permanent teeth to erupt (FIG. 14.9); and lack of formation and presence of permanent teeth. Usually it is of little concern when teeth are slow to erupt, but occasionally there is a problem. If you have any question, you should consult a professional. Alternatives include the following:

FIG. 14.8 Unerupted teeth.
(From Koch G et al: Pedodontics: a clinical approach, Copenhagen, 1991, Munksgaard.)

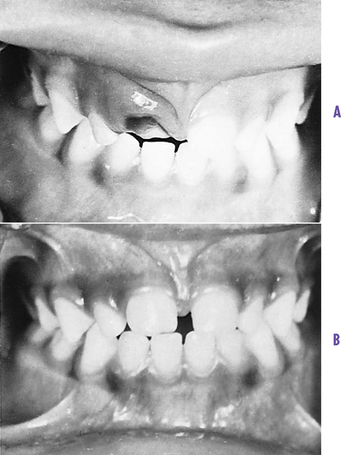
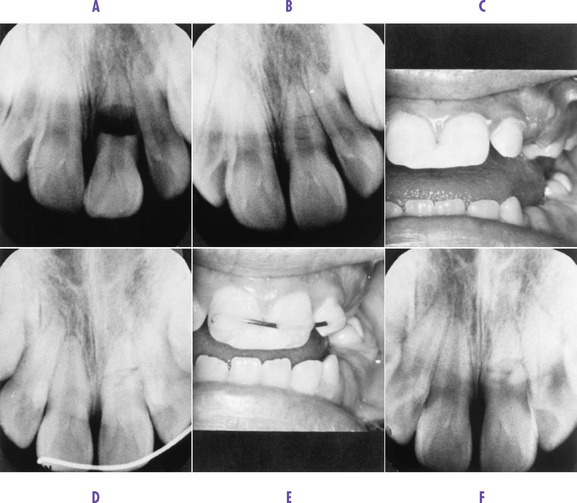
3. Dark-Colored Primary Tooth
(FIG. 14.12). Children often suffer an accidental blow to a primary tooth. Sometimes the parent may not even know it happened. Later the tooth turns dark. Usually the tooth pulp (nerve) (FIG. 14.13) has been injured, and the dark coloration is caused by degenerative pigments in the blood supply to the nerve inside the tooth. This condition may or may not be painful. Alternatives include the following:

FIG. 14.12 A and B, Dark primary (baby) tooth caused by trauma.
(From McDonald RE, Avery DR: Dentistry for the child and adolescent, ed 7, St Louis, 2000, Mosby.)

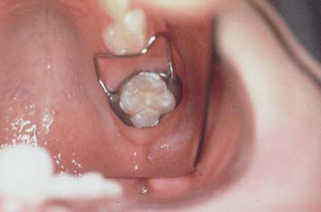
4. Primary or Permanent Tooth Accidentally Forced into Gum Tissue and Bone
(FIG. 14.15). A primary or permanent tooth may be accidentally pushed forcefully into the underlying bone and soft tissue. If the child is only a few years old, there may be a problem with the underlying partially developed permanent tooth; the primary tooth could injure the developing tooth bud of the permanent tooth. However, if the child is older, and depending on which tooth is involved, the underlying permanent tooth may not be damaged. Damage to an underlying permanent tooth cannot be determined completely until the suspect tooth erupts later. If the primary tooth is severely fractured under the gum, it may need to be removed. If the tooth is a permanent one, the damage is usually related only to the tooth receiving the blow. Alternatives include the following:
5. Infant or Young Child With Multiple Decayed Teeth, Especially in Front of Mouth
(FIG. 14.17). This condition is often called the bottle mouth syndrome or baby bottle syndrome. It involves allowing the child to suck a bottle of any sugar-containing substance for hours at a time. Teeth are usually decayed slightly to severely and require selection of one of the alternatives described previously in the first section “Holes in Primary Teeth” (p. 113).

Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


