Treatment Considerations
Overdenture therapy is indicated1 for:
- Patients who are dissatisfied with complete dentures and demand greater stability and oral comfort.
- Elderly patients who desire a more stable mandibular denture.
- Patients who have congenital or oral and maxillofacial defects and are in need of oral rehabilitation.
For patients with difficulty functioning and adapting to a mandibular conventional denture, two standard-diameter implants at least 10 mm in length are generally sufficient to provide retention and support for an overdenture prosthesis.8,9
Patients who wear conventional dentures for a long period have a greater chance of developing problems, especially with the mandibular prosthesis, due to unfavorable loads and demands on the mandibular ridge. The clinical consequence of these problems translates to a resorption of the alveolar crest, followed by resorption of the basal bone and finally by an alteration of facial-tissue support. Panoramic radiographs can reveal the amount of remaining bone.
Consultation with a surgeon and restorative dentist is recommended.
Patient Presentation
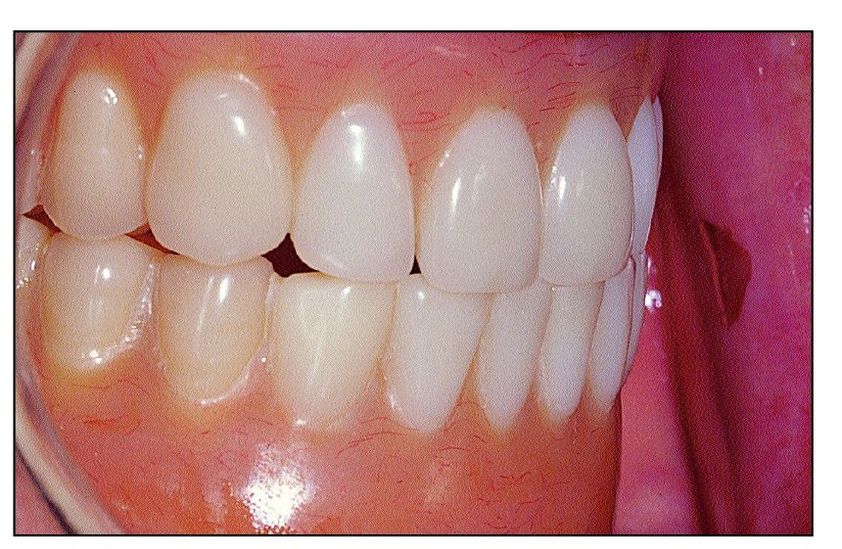
Fig 13-1 A 70-year-old healthy woman has been edentulous since the age of 40 years. She sought treatment because of poor function of her mandibular prosthesis. Her present conventional dentures are 4 years old. In 30 years of wearing conventional dentures, she has never been comfortable with her mandibular denture because it lacks retention and stability, and she has difficulties chewing food.This discomfort has become increasingly apparent in the last 10 years. She is satisfied with the appearance of her maxillary conventional denture and wants to maintain the same tooth arrangement and facial-tissue support
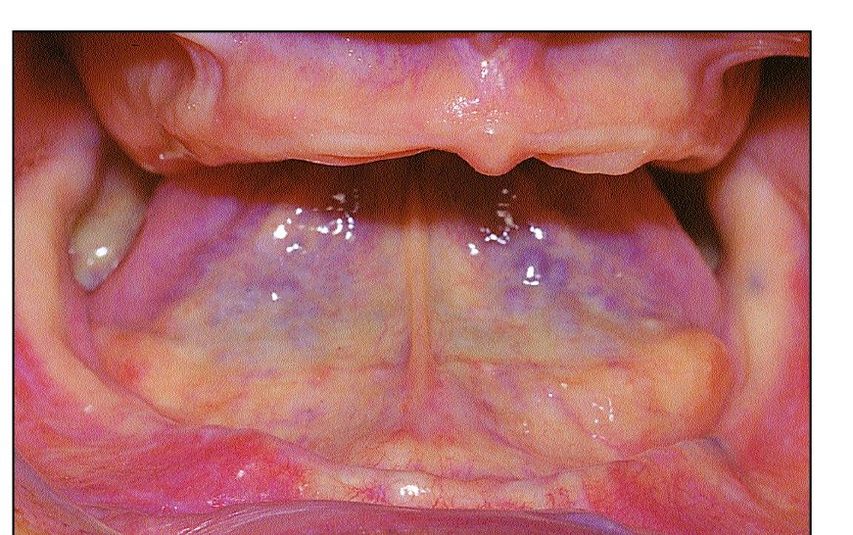
Fig 13-2 Intraoral examination reveals a resorbed and atrophic mandibular ridge that provides minimal denture stability and retention. The midlateral portion of the mandible provides little resistance to dislodgment during denture function.The premolar area is frequently irritated.
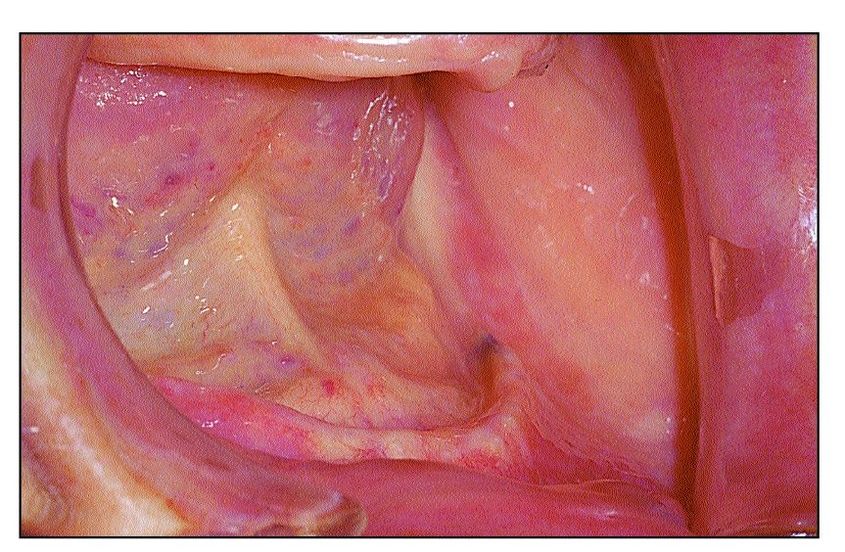
Fig 13-3 The anterior mandibular area has a thin bony ridge. The sagittal interarch relationship is relatively normal but displays a slightly anterior mandible. Interarch space is greater than normal.
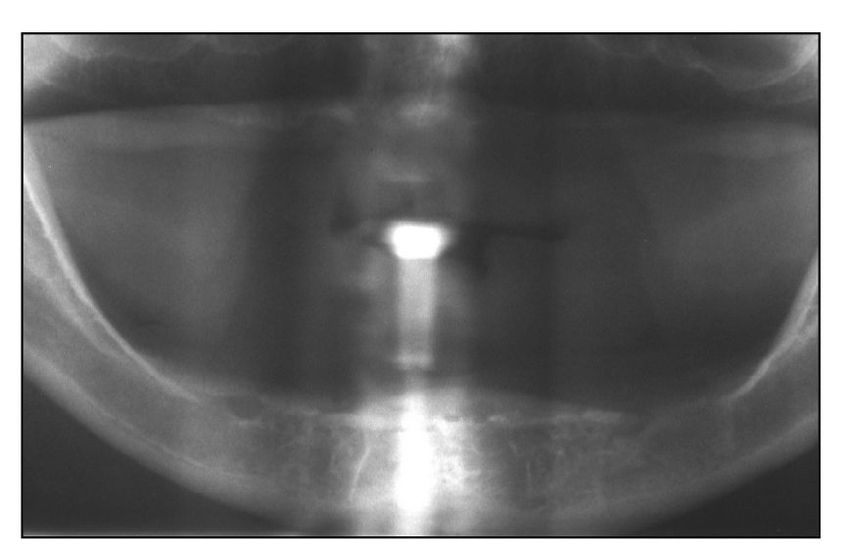
Fig 13-4 The remaining bone corresponds to a type C bone quantity and a type III bone quality.10 The mental foramina were located on the surface of the ridge, which may contribute to this patient’s discomfort during mastication.
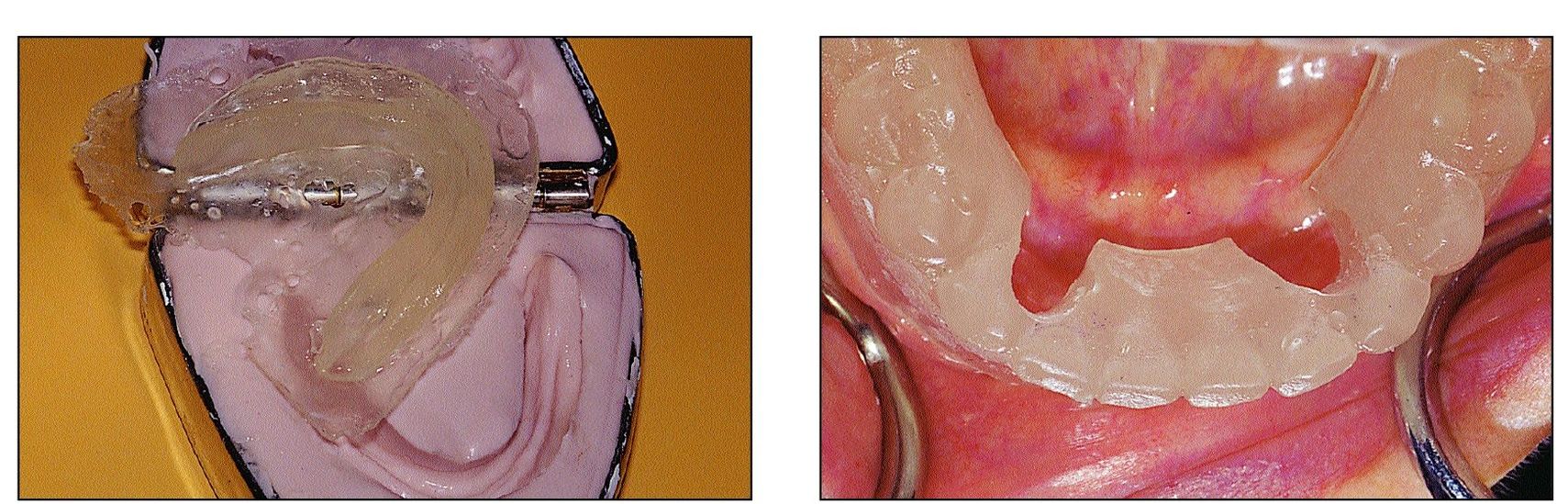
Figs 13-5 and 13-6 A surgical stent is fabricated by duplicating the mandibular denture with orthodontic resin (left). Two vertical grooves are drilled on the lingual surface in the canine areas (right).The anterior position of the implants permits rotation of only the posterior segment of the overdenture. It is important that the rotation axis created by the two implants be parallel to a line through the retromolar pads to allow the overdenture to rotate freely
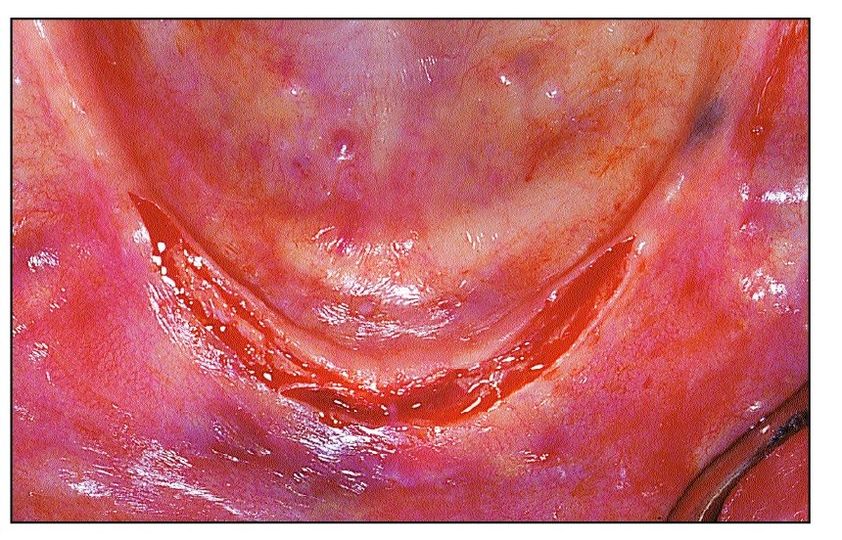
Fig 13-7 A midcrestal incision is made and extended between the first premolar areas. The incision may be limited by the presence of the mental foramina.
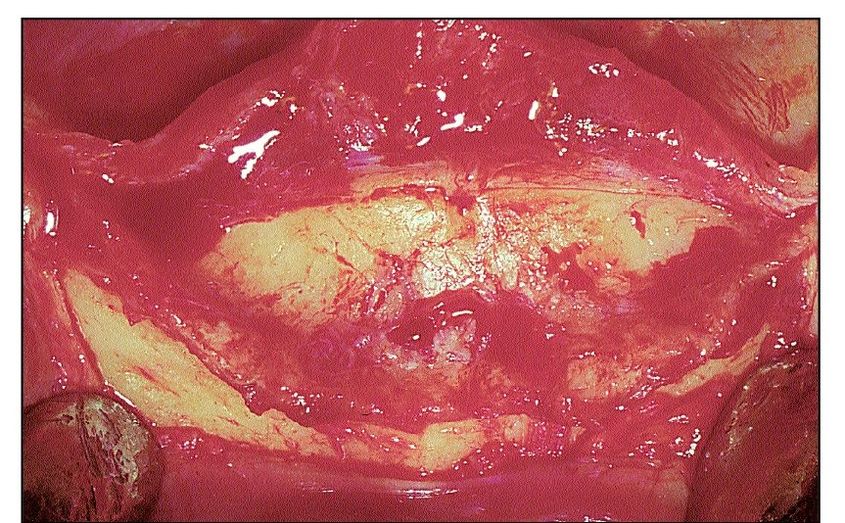
Fig 13-8 Buccal and lingual full-thickness flaps are elevated to expose the residual osseous crest. This surgical approach allows visibility of the ridge morphology and enables the surgeon to modify its shape prior to implant placement.
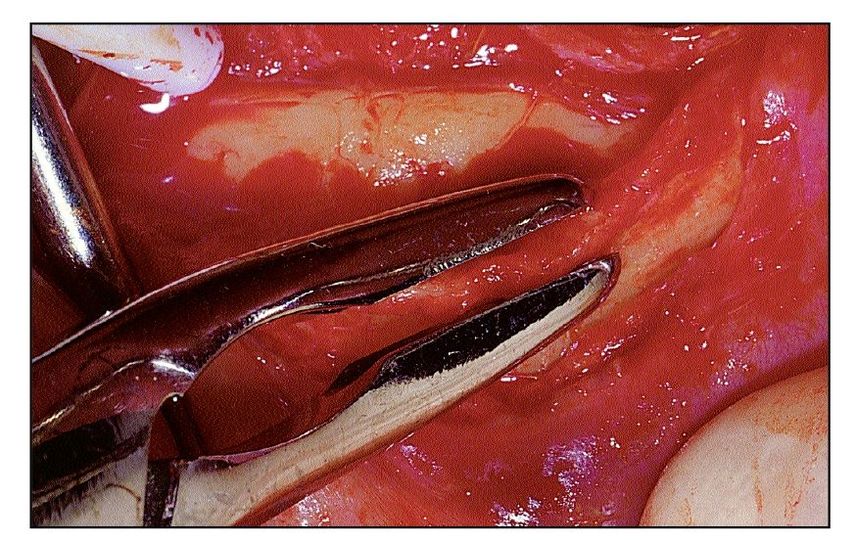
Fig 13-9 The residual osseous crest may need to be eliminated. This provides a more favorable recipient site and minimizes the chance of labial or lingual bony dehiscences.
Fig 13-10 The surgical stent allows for appropriate orientation during preparation of the implant site In this case, both implant sites were prepared for placement of solid screws 10 mm in length.
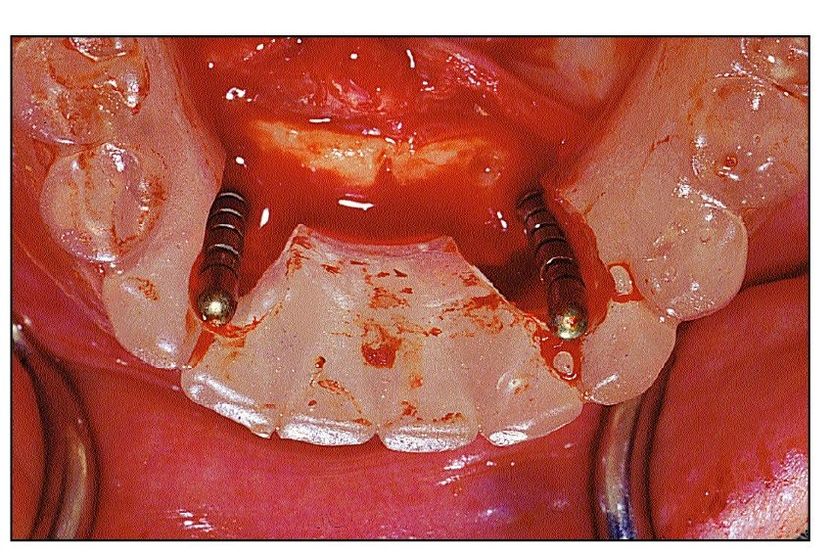
Fig 13-11 Alignment pins (2.2-mm diameter) are inserted into the partially prepared implant sites to verify the orientation relative to the surgical stent.
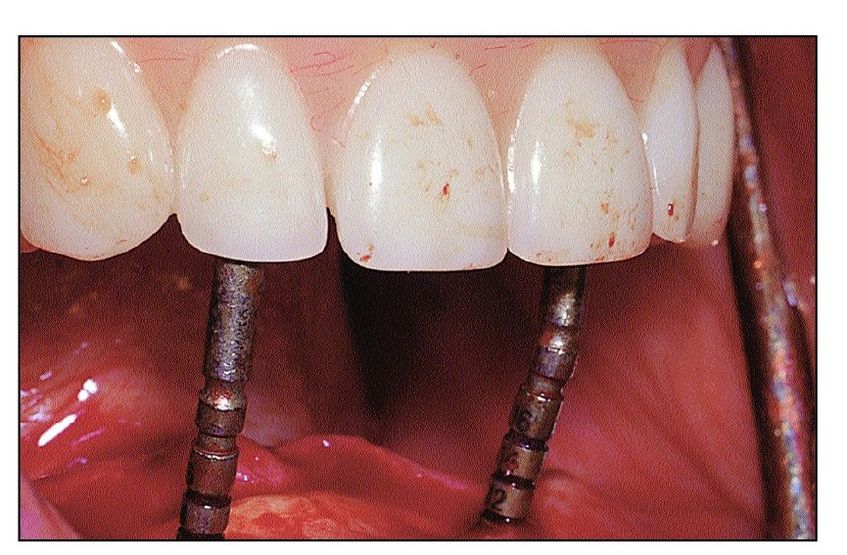
Fig 13-12 Alignment pins also allow the surgeon to evaluate the longitudinal axis of the implants in relation to the incisal edges of the maxillary denture.
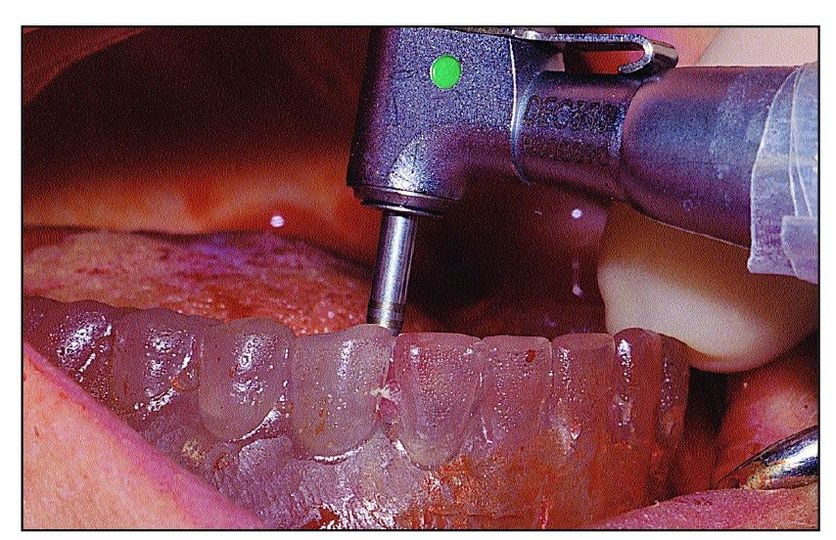
Fig 13-13 The implant sites are then enlarged with a 2.8-mm pilot drill and a 3.5-mm spiral dill, successively. Drilling depth was controlled via clearly visible laser markings on the drilling instruments. The depth can then be verified with a depth gauge. Final site preparation is completed with tapping of the implant site. The screw tap and depth gauges are also marked to allow determination of insertion depth.
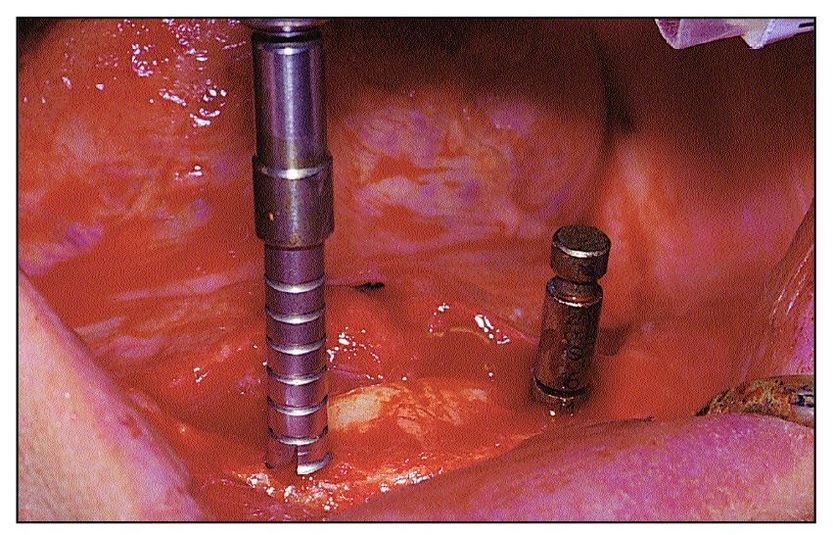
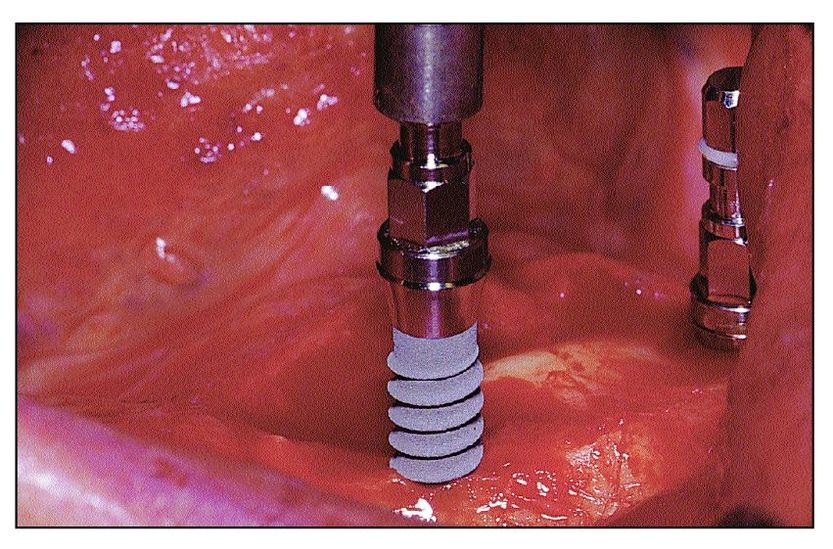
Fig 13-14 Two 4.1 mm × 10 mm solid screw implants with a sandblasted, large-grit, acid-etched (SLA) surface are inserted into their respective sites witharatchet, under constant irrigation.
Fig 13-15 For ball-retained mandibular overdentures supported by two implants, implant placement is limited such that the SLA surface is submerged just below the ridge crest.11 Overseating of the implant in the recipient site should be avoided in order to maximize the length of the transgingival portion of the implant collar.
Only gold members can continue reading.
Log In or
Register to continue