12
The Benefits of Consulting with an Ear, Nose, and Throat (ENT) Specialist Before and During Orthodontic Treatment
Summary
The mouth is anatomically at the center of the region in which the otolaryngologist/head and neck surgeon operates. Thus, many interactions between the ear, nose, and throat (ENT) specialist and the orthodontist become natural and often necessary. In this chapter, the anatomical relations between the mouth, nose, ear, and throat are reviewed. The areas of interaction include conditions that usually involve only the orthodontist and the ENT specialist (such as airway obstruction, temporomandibular dysfunction, and possibly conductive hearing loss), or both of them in the context of a cooperative team in the treatment of craniofacial anomalies. Most prominent among conditions requiring interaction is airway obstruction and its consequent effects on facial morphology and function. The evidence for early adenoidectomy and/or tonsillectomy is emerging from recent studies; however, specific guidelines are yet to be formulated. Conductive hearing loss may be improved by maxillary expansion but focused research should validate this potential. Ear pain is a ground for cooperation, particularly when the temporomandibular joint is affected. In the context of a working team, treatment of cleft lip/palate and other craniofacial anomalies engages both specialists at various stages of interventions that usually span the growing years of the patient.
Introduction
The obvious reason for the important interaction between the orthodontist and the otolaryngologist is the critical position of the mouth between the nose and throat. In as much as the jaws extend laterally, the connection extends to the areas of the ears. The scope of interaction between dentists in general and ENT specialists is summarized with respect to each of these anatomical entities in Box 12.1, with the more focused interface with the orthodontists specifically indicated. Certain problems benefit from consultation with the ENT specialist before orthodontic treatment (malocclusions associated with mouth breathing), while others would require consultation before and during treatment (cleft lip/palate).
Box 12.1 Conditions of Potential Interaction between ENT Specialist and Dentists in Head and Neck Areas
Mouth and Jaws
Related to function and facial esthetics
- Cleft palate and cleft lipa
Not related to facial esthetics
- Cold sores
- Periodontal (gum) disease
- Oral ulcers
- Tongue problems
- Halitosis or bad breath
- Temporomandibular dysfunction (TMD)
Nose
Related to breathing
Not related to breathing
- Cosmetic surgery-rhinoplasty
Ear
Related to potential effect of maxillary expansion on Eustachian tube
- Conductive hearing
Related to pain and oral function
- Ear ache (possibly from TMD)
Throat
Related to breathing
- Tonsilsa
- Infections
a Most common areas of interaction between orthodontist and otolaryngologist.
The Anatomical Connection: the Mouth in Its Relation with the Nose, Throat, and Ear
Normal Anatomy
The posterior boundary of the oral cavity comprises two pairs of folds of mucous membrane that cover two palatal muscles, the palatoglossus and the palatopharyngeus (Figure 12.1a). The tonsil lies between these folds, which provide the contour of an opening, the exit from the oral cavity (fauces) to the pharyngeal area. The nasal cavity, extending from the nostrils anteriorly to the choanae posteriorly, is divided into halves by the septum, which is formed by the perpendicular plate of the ethmoid bone above, the vomer bone posteriorly, and by an extensive cartilage anteriorly (Figure 12.1b). The roof of each nasal cavity is formed by the cribriform plate of the ethmoid bone, through which olfactory nerves enter the nasal cavity. The most important features of the lateral walls are the three bony shelf-like conchae or turbinates, which are covered with highly vascular mucous membranes (Figure 12.1c). Air is heated and humidified past the conchae during breathing. Beneath each concha is a meatus that opens the nasal cavity to the paranasal sinuses and the nasolacrimal duct.
Figure 12.1 Anatomical structures in mouth and face: (a) oral and pharyngeal soft tissues; (b–d) sagittal cross-sections through oral and nasal hard tissues near-midline (b), lateral (c) and through nasal and paranasal sinuses (d). (Figure d is adapted from Moore K (1992) Chapter 7, ‘The Head’, Figure 7, in Clinically Oriented Anatomy, 3rd edn. Courtesy of Lippincott, Williams & Wilkins.)
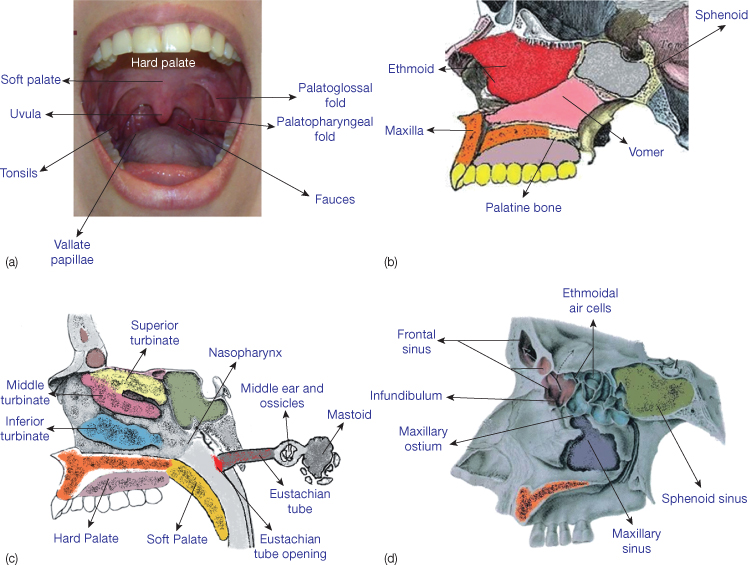
The paranasal sinuses are membrane-lined cavities within the frontal, maxillary, ethmoid, and sphenoid bones (Figure 12.1d). The ethmoid sinus comprises a series of small, interconnected air cells instead of a single hollow space. The sinuses communicate with the nasal cavity at the level of the superior and middle meatuses and lateral walls of the cavity, but not through the inferior meatus in which the nasolacrimal duct opens. Thus tears produced in the eye by the lacrimal (and other) glands are collected into this duct and enter the nasal cavities. Not well known, the function of the paranasal sinuses has been subject to various hypotheses: lightening the housing bones, acting as resonance chambers during speaking (increasing voice resonance), buffering against blows to the face, humidifying and heating the inhaled air, or as we suggest, being part of the oropharyngeal capsular matrix (as defined by Moss, 1969, 1997a,b) to which the adjacent structures adapt to maintain the functional primacy of the matrix (see section on Growth concepts below).
Common Sources of Anomalies in the Oronasal Area
Particularly in children, hypertrophy of the adenoids and tonsils is a primary cause of nasal airway obstruction, leading to mouth breathing, which, in turn, may affect facial morphology. Located in the roof of the nasopharynx, anterior to the basiocciput and inferior to the sphenoid, the adenoids are a mass of lymphoid tissue that merges with the lymphoid tissue of the fossa of Rosenmuller near the opening of the Eustachian tube, which connects to the ear. Development of the adenoids is unique among major tissues of the body: they increase in size to a peak of approximately 200% the adult size around puberty then decrease to near-total regression in most adults (Scammon et al., 1930; Linder-Aronson and Leighton, 1983). The nasopharynx enlarges to accommodate the growing adenoids, thus maintaining a patent nasopharyngeal airway (Diamond, 1980) but any imbalance between the developing airway and the concomitant adenoid growth may result in nasopharyngeal obstruction or reduced potency (Diamond, 1980). Also, some reports indicate that the lymphoid tissues do not follow a specific growth curve, but respond individually to different environmental factors (Pruzansky, 1975). Given their critical anatomical position, hypertrophied adenoids may affect nasal function as well as obstruct the Eustachian tubes, participating in the formation of middle ear effusions. Tonsillar hypertrophy may also lead to airway obstruction. In the rare condition when tonsils touch or meet in the midline, they are called ‘kissing tonsils’.
The tonsils (palatine or faucial tonsils) and the adenoids (pharyngeal tonsils) are part of Waldeyer’s tonsillar ring (or pharyngeal lymphoid ring), named after a nineteenth-century German anatomist. The ring also includes the tubal tonsil, where the Eustachian tube opens in the nasopharynx and the lingual tonsils. As the tonsils and adenoids are located at the gate of the upper respiratory and alimentary tracts, where they are constantly exposed to antigens, they are mostly composed of immunologically reactive lymphoid tissue containing antibody-producing lymphocytes. A number of observations and findings may be noted regarding the associated immunological role (Hata et al., 1996; Valtonen et al., 2000; Kaygusuz et al., 2009):
- Adenoids and tonsils are related to a sounder immune status and general health of patients, carrying out the functions of humoral and cellular immunity.
- Inflammation and/or hypertrophy of adenoids and tonsils are caused by hypofunction of local and systemic immunity.
- There is not enough evidence to corroborate the suggestion that the adenoids and tonsils become a health liability because they may not be able to cope with the various viral infections attacking children in urban areas.
- Though still debated, particularly regarding the timing of surgery relative to patient’s age, more recent findings indicate that removal of the lymphoid tissues has no adverse effect on immunity.
As alluded to in the list above, tonsils and/or adenoids present a health problem when they become the nest of continuous infections and cause airway obstruction. Not only does the blockage induce mouth breathing, but also a nasal twang to the voice, snoring, restless sleep (and associated learning problems if chronic), and facial dysmorphology. Hence, reasons for adenoidectomy often include chronic and recurrent fluid or infections of the ears, chronic or recurrent sinus infections or ‘rhinosinusitis’, and nasopharyngeal blockage. Because tonsillar infection is rarely associated with ear infections, tonsillectomy is usually indicated when tonsils are enlarged.
Often conducted with the assistance of a small mirror and completed on average within 15–20 minutes, adenoidectomy involves ‘shaving’ or curetting the adenoid tissue from the back of the nose. Usually low-grade bleeding is eliminated by cauterization. Though rare, surgical complications include infection of the surgical site (a source of bad breath), minor bleeding, and infrequently velopharyngeal insufficiency, possibly related to neglect of anatomical considerations. Postsurgical pain is more pronounced with tonsillectomy.
Areas of Interaction
Airway Obstruction
Effect on Facial and Occlusal Morphology
The impact of airway impairment on dentofacial morphology has been evaluated extensively (Emslie et al., 1952; Linder-Aronson, 1970; Subtelny, 1975; Linder-Aronson et al., 1986; Behlfelt et al., 1989a,b, 1990; Kerr et al., 1989; Warren, 1990; Tourné, 1991; Woodside et al., 1991a,b; Linder-Aronson et al., 1993; Oulis et al., 1994; Valera et al., 2003; Mattar et al., 2004). In his pioneering work on definition of malocclusion, Edward Angle (1907) emphasized the consideration of not only the ‘peculiarities’ of the occlusion, and the relations of the jaws, but also the ‘condition of the throat and nose [and] habits of the patient’. In a revealing way, Angle accounted for mouth breathing in his classification of two opposite malocclusions. He described the Class II division 1 malocclusion as ‘always accompanied and, at least in its early stages, aggravated, if not indeed caused by mouth breathing due to some form of nasal obstruction’. Also, regarding the etiology of Class III, his only explanation was that: ‘deformities under this class begin at about the age of the eruption of the first permanent molars, or even much earlier, and are always associated at this age with enlarged tonsils and the habit of protruding the mandible, the latter probably affording relief in breathing’.
Though Angle’s specific premises, formulated before the advent of cephalometrics, still require focused study, the prevailing theory regarding the effects of nasal obstruction stipulates that ensuing chronic oral respiration becomes the etiology of occlusal and skeletal deformities. Children with chronic mouth breathing have often been found to have narrow maxillary dental arches (Subtelny, 1975; Oulis et al., 1994), anterior open bite, usually through excessive eruption of posterior teeth and a hyperdivergent skeletal pattern (Subtelny, 1975). Development of malocclusion seems to be related primarily to low posturing of the tongue (and the subsequent adaptation of other facial muscles) that may influence growth of the jaws and the occlusion. The lips, in repose, have been described to part (Subtelny, 1975), although nasal breathing is possible with incompetent lips when the tongue provides an anterior seal (Hepper et al., 1990).
Airway obstruction has been mostly associated with adenoid hypertrophy, and thus the use of the term ‘adenoid facies’ (apparently coined over 100 years ago (Proffit, 2007), synonymous with ‘long face syndrome’ (Tomes, 1872; Angle, 1907; Hershey et al., 1976) and ‘high-angle’ facial pattern. Children who need adenoidectomy have been reported to have longer facial height, steeper mandibular plane angles, and a more retrognathic mandible than corresponding controls (Linder-Aronson, 1970; Linder-Aronson et al., 1986, 1993; Kerr et al., 1989; Woodside et al., 1991a,b). Likewise, children with enlarged tonsils have been reported with more retrognathic and posterosuperiorly inclined mandibles, greater anterior total and lower facial heights, and increased mandibular plane angles (Behlfelt et al., 1989a).
Methods of Evaluating Airway Obstruction
Tonsillar hypertrophy is more readily diagnosed clinically and its cephalometric determination is mostly corroborative (Figure 12.2a). Cephalometric imaging and the more intrusive endoscopic examination are more reliable in the diagnosis of adenoid hypertrophy. Cephalometric assessment of palatal airway may be through subjective rating or direct measurement of defined distances.
- Various grading systems are available based on direct observation of the adenoid within the pharyngeal space. One such system stratifies three grades by estimating the space the adenoid occupies between the posterior cranial base and the soft palate:
- Grade 1 – less than 50% of the airway is blocked
- Grade 2 – more than 50% but less than 100% of airway is obstructed
- Grade 3 – a near-total to total obstruction is observed (Figure 12.2b–d).
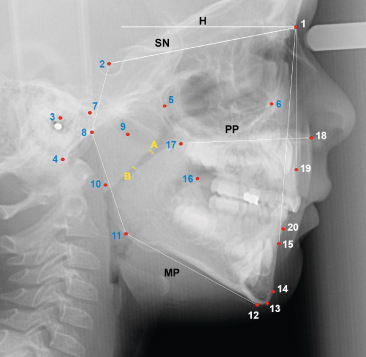
- The adenoids have been evaluated from a two-dimensional cephalometric record that simplifies the imaging of three-dimensional structures. Cephalometric assessment has been reported to have moderate to high correlations with the diagnosis of actual obstruction (r 0.60–0.88) by endoscopic evaluation or actual size of excised lymphoid tissue (Major et al., 2006). Measurements of the shortest distance between adenoid and soft palate (SAD), and the distance between the maximum convexity point and soft palate (CAD) have correlated best with actual size (Figure 12.3).
Figure 12.2 (a) Enlarged tonsils (arrow) on lateral cephalogram. The tonsil extends posteriorly and inferiorly. (b–d) Lateral cephalograms of three children with chronic mouth breathing showing different grades of airway obstruction relative to adenoid size: (b) grade 1 (less than 50% obstruction of airway) in a girl aged 12 years and 3 months; (c) grade 2 (more than 50% obstruction but less than 100% airway obstruction) in a boy aged 4 years and 4 months; and (d) grade 3 (total obstruction) in a boy aged 4 years and 9 months.
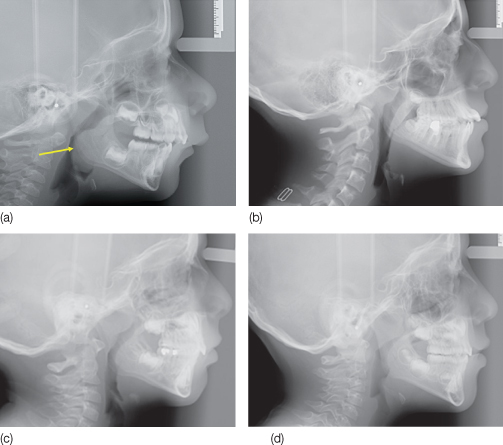
Figure 12.3 Cephalometric landmarks, planes, and measurements in study of craniofacial morphology related to adenoid hypertrophy. Linear measurements of the palatal airway (between the adenoids and soft palate). ‘A’ is the distance between most convex contour of the adenoid and soft palate (CAD); and ‘B’ is the shortest distance between adenoid and soft palate (SAD). Various hard tissue landmarks (1-20) were used for linear and angular measurements. Key findings included the increased posteroinferior inclination of the palatal plane (PP) relative to the horizontal (H) oriented on natural head position, augmented hyperdivergence between PP and MP (mandibular plane through Me and Go), as well as increased angle between MP and SN.
In a study of the correspondence among and between subjective and linear measurements of palatal airway on lateral cephalographs, Bitar et al. (2010) found a high correlation between SAD and CAD (r 0.915), and moderate to high correlations between the palatal airway grading (1–3) and SAD and CAD measurements (r −0.73 and −0.79, respectively), accounting for correspondence of evaluation in more than 50% of the population.
Developing technologies should improve imaging and appraisal of hypertrophied tissues and their proportionate relations to the nasal passages. When cephalometric adenoid rating is negative, the ENT specialist may resort to other means of assessment (endoscopy) to investigate other obstructive causes (e.g. enlarged turbinates).
The determination of mouth breathing is often based on subjective reporting by the patient or parents, usually incorporated in the health history questionnaire, with inquiry on respiratory mode during the day and at night. The high correlation observed in the aforementioned study between the subjective ratings, commonly utilized by otolaryngologists and the cephalometric measurement of airway clearance (SAD, CAD), indicates the significance of the radiographic record. Three-dimensional imaging of nasopharyngeal space and structures yields more accurate information (Grauer et al., 2009), but its potential association with mouth breathing requires quantitative assessments of respiration. Various means to generate objective evidence, such as rhinometry, nasal flow, and nasal resistance, have yet to be proven effective or practical for determining or predicting mouth breathing. New devices need additional validation (Fujimoto et al., 2009; Ovsenik, 2009). The variety in frequency, duration, and intensity of mouth breathing is probably the reason for variation in outcome of these quantitative measurements. Yet, objective measures are preferable to simply subjective reports or assessments.
Time and Sequence of the Effect of Obstruction on Facial Alterations
In a recent study (Bitar et al., 2010), we analyzed the cephalographs of 200 Caucasian children (ages 1.71–12.62 years, nearly 50% of them <5 years). They were diagnosed as chronic mouth breathers by the pediatric otolaryngologist who referred them for cephalometric appraisal of adenoid hypertrophy. Facial dysmorphology was observed as early as the second year of life in the youngest patient evaluated (1.71 years). Posteroinferior tilt of the maxilla (average inclination of palatal plane to horizontal: −7.68° ± 3.44°; norm: 0° ± 2.5° (Ricketts, 1981), possibly the initial response to functional alteration, occurred separately or together with one or all of the following modifications, compatible with a hyperdivergent vertical pattern: increased palatal to mandibular plane angle; increased lower face height, steep mandibular plane, mandibular antegonial notching, increased gonial angle, and elongated and thinner symphysis (Figures 12.3 and 12.4). The palatal tilt reached severe levels (8–9°) between ages 4 and 5 years. The occlusion ranged from normal with adequate overjet/overbite to malocclusions that contained one or more of these characteristics: posterior crossbite, increased overjet, Class II molar relationship, open bite, and anterior crossbite.
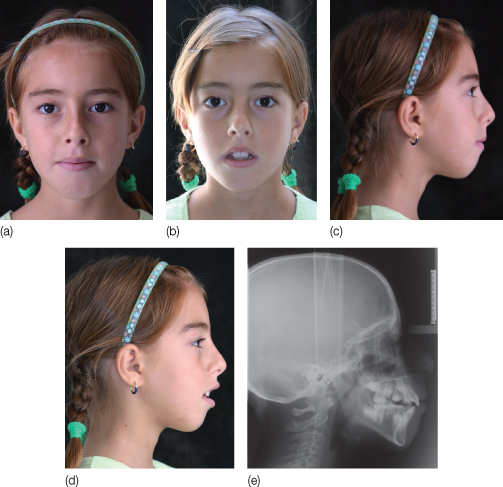
Figure 12.4 Morphological characteristics of the ‘long face’ syndrome in a 10 years and 10 months old girl with chronic mouth breathing. Extraoral photographs (a–d) reveal lip incompetency, increased lower facial height, narrow nose base width and shadows under the eyes from chronic venous congestion. (e) Lateral cephalograph of the same patient shows characteristic findings of adenoid facies: palatal plane (ANS-PNS) tipped posteroinferiorly, steep mandibular plane (MP: menton-gonion), angular notching, reduced inclination of anterior slope of chin, increased lower face height.
The research suggests formulations regarding the association between airway status and craniofacial morphology and growth, as well as clinical implications that require additional research for validation.
Growth Concepts Revisited
Facial dysmorphology related to nasal obstruction apparently starts in structures closest to the obstruction: a posteroinferior tilt of the maxilla.
Occlusal variations among the investigated children (Bitar et al., 2010) are similar to the experimental findings of Harvold et al. (1972, 1973, 1981) in monkeys at comparable ages. Harvold et al. obstructed inspiration but allowed slight air escape during expiration in growing monkeys between ages 2 and 6 years, most of them (34/42) in the late deciduous and mixed dentitions (ages 2–4 years). The response differed considerably, each animal finding its ‘own most convenient way to secure the oral flow, and then develop a dental occlusion in accordance with this new function’ (Harvold et al., 1981). Therefore, oral respiration induced mesioclusion, maxillary protrusion with distoclusion, open bite, dual bite and some common cephalometric traits: increased face height, steeper mandibular inclination, and a larger gonial angle. The array of occlusal and cephalometric changes was similar in these animals and the investigated children, whose various malocclusions were also probably related to individual adjustments in respiration.
Our findings qualify the variable relation between nasal obstruction and facial growth in line with Moss’s functional matrix theory, which stipulates that facial growth is related to the function of the various components in the head and neck region (Moss, 1969, 1997a,b). The oropharyngeal space is a primary entity (capsular matrix related to respiration) that influences the position and behavior of the surrounding soft tissues, which in turn shape the associated skeletal units. Impingement on the oropharyngeal space leads to adaptive reorganization of the latter. Thus, the adaptation begins with and may be restricted to the posteroinferior maxillary tilt, probably because of its proximity to the obstructed pharynx.
The greater amplitude of adaptation in younger ages suggests that growth at early ages (≤5 years) is affected with more deviation from the norm. The adjustment may also start with mandibular remodeling favoring an increase in the gonial angle and mandibular plane inclination. Additional or more severe morphological changes would be associated with more severe airway blockage, the long face syndrome representing the extreme expression of sustained functional disturbance. Conversely, any degree of adaptive morphological change may result in a level of restoration of nasal breathing. Accordingly, as airway obstruction ranges from total to partial, and adaptation to either is an individual response to preserve the oropharyngeal matrix, the variation in malocclusions is not surprising. The association between amount of blockage and specific signs of malocclusion remains unknown. The severity and extent of dysmorphology would depend on the timing, duration, and rate of oral breathing and associated functional changes, given that a percentage of nasal breathing may coexist with mouth breathing (Fields et al., 1991).
As suggested by Angle, and also observed in a number of patients, a forward positioning of the mandible enlarges the airway and enhances breathing through the consequent increase of airflow, in a manner akin to mandibular manipulation in the treatment of sleep apnea (Liu et al., 2000). If sustained, the ensuing anterior crossbite may induce maxillary retrognathism that otherwise would not exist. This phenomenon reflects intra-growth orthopedics (maxillary retrognathism) generated by the transfer of functional forces through a non-therapeutic occlusal ‘environmental induction’ (anterior crossbite) (Ghafari, 2004).
Clinical Implications
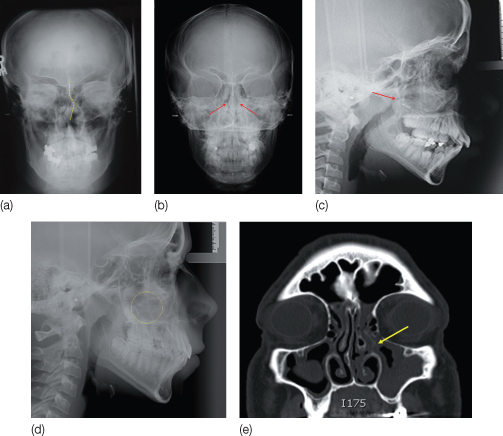
The critical clinical issue is determining the optimal time of lymphoid tissue removal to enhance nose breathing and prevent potential, or reverse existing, abnormal facial growth. The above findings emphasize the need for pediatricians and pediatric otolaryngologists to examine children for impaired nasal respiration early in childhood, and ascertain their breathing mode at night from the parents. Otolaryngologists and orthodontists should appreciate the early impact of enlarged adenoids and tonsils, the most common obstructive agents of the posterior pharyngeal airway. Other causes that raise nasal resistance may involve the hard tissues such as a deviated septum, turbinate irregularities and congenital or traumatic asymmetries of the nasal cavity, or the soft tissues such as catarrhal and allergic rhinitis and nasal polyps (Figure 12.5) (Timms, 1981).
Figure 12.5 (a) Septal deviation: S-shaped deviation of nasal septum shown on a posteroanterior cephalograph. (b) Bilateral obstruction of the airway in a patient aged 10 years and 7 months, by the hypertrophied inferior turbinates (right and left, arrows) shown on a posteroanterior cephalograph. (c) The lateral cephalometric radiograph of the same patient shows the posterior extension of the inferior turbinate toward the posterior wall of the nasopharynx (arrow), causing the obstruction of the airway. On endoscopic otolaryngological examination, the diagnosis of inferior turbinate hypertrophy was confirmed, and medication (nasal topical steroids) improved breathing. (d) Cephalometric radiograph of a 14-year-old chronic mouth-breathing patient with hyperdivergent vertical pattern but positive clinical overbite (30%). Note the hypertrophic adenoids, and a unilateral nasal polyp (yellow circle) that contributed to nasal obstruction. (e) The computed tomography (CT) scan shows the extension of the polyp (arrow) from the sinus.
Otolaryngology
The prevailing practice among otolaryngologists is to delay removal of the pharyngeal lymphoid tissues because of their role in immunological defenses, and the peculiar adenoid growth between ages 3 and 16 years, that is, the increase in size in preschool and primary grade years followed by a decrease during pre- and early adolescence (Linder-Aronson and Leighton, 1983). Commonly, otolaryngologists follow the guidelines for adenotonsillectomy, in general as supported by the American Academy of Otolaryngology. The indications include:
- Hypertrophy causing upper airway obstruction (sleep apnea), severe dysphagia, sleep disorders, or cardiopulmonary complications
- Peritonsillar abscess unresponsive to medical management and drainage documented by the surgeon, unless surgery is performed during an acute stage
- Patients having three or more infectious episodes related to the tonsils and/or adenoids per year despite adequate medical therapy
- Recurrent acute otitis media or chronic serous otitis media. Adenoidectomy should not be performed with the insertion of the first set of myringotomy (ear) tubes unless there is another indication for adenoidectomy besides chronic otitis media. However, repeat surgery for chronic otitis media should consist of adenoidectomy with myringotomy (with or without tube placement). Adenoidectomy for the treatment of otitis media in children under the age of 2 years has not been found to be beneficial (Mattila, 2006).
- Unilateral tonsil hypertrophy presumed euplastic. Most asymmetries can be followed conservatively without other indications for potential surgery such as abnormal appearance, symptoms, or history
- Hypertrophy causing malocclusion or adversely affecting orofacial growth, documented by the orthodontist
- Chronic or recurrent tonsillitis associated with the streptococcal carrier state and not responding to β-lactamase-resistant antibiotics.
- Persistent foul taste or breath caused by chronic tonsillitis and not responsive to medication.
Development of long-face features may be minimized or reversed through resumption of normal breathing, possibly aided by orthodontic/orthopedic treatment. Post-treatment studies of adenoidectomy (Linder-Aronson et al., 1986; Woodside et al., 1991a; Bahadir et al., 2006) record a more anterior direction of symphyseal growth, reversal of the tendency to posterior mandibular rotation, increased amount of mandibular growth, and no difference in direction of maxillary growth. Yet, individual growth direction after adenoidectomy has been shown to be more variable than in control children with clear airways matched for age and ge/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


