CHAPTER 12 Oral and Maxillofacial Surgery, Oral Pathology, Oral Medicine
Diseases and Surgery Related to the Oral and Facial Areas
Many diseases in various parts of the body have oral implications. In fact, the mouth is a mirror of overall body health. Dentists can tell about general body health by looking in the mouth, observing the condition of the soft and hard tissues, and repeating the examination over a period of weeks or months for comparison. The condition of the teeth and the bone and gums that support them are dependent on numerous conditions, including hereditary factors, diet, oral hygiene, and overall health. You should consult your dentist or dental specialist about any conditions or diseases of the oral cavity or related structures. These practitioners are the most educated and experienced of all health practitioners with regard to that part of the body. In the event that your dentist does not recognize your oral condition, he or she will refer you to the appropriate practitioner for further observation.
WHAT YOU SEE OR FEEL
Conditions, Signs, or Symptoms Related to Oral and Maxillofacial Surgery, Oral Pathology, or Oral Medicine
1. Loose Teeth (Fig. 12.1): When you bite on your teeth, you feel movement, and when you grasp them with your fingers and apply force, you can feel and see movement. Sometimes the looseness may be so severe that you feel that you could extract a tooth yourself or force it out by eating.

Several conditions cause loose teeth. The most common ones are described below:
2. Gums Bleed Easily: Bleeding gums are described in the chapter on periodontics (gum and bone diseases) (p. 129). Usually this condition is a result of periodontal disease. Periodontal (gum) surgery may be possible (p. 135). Tooth extraction is the last and least desirable possibility.
3. Slightly Broken Tooth (Fig. 12.2): A break of the coronal portion of the tooth (tooth part that normally appears when you open your mouth) is usually repairable with relatively simple restorative methods (p. 142).

4. Moderately Broken Tooth (Fig. 12.3): If most of the coronal portion of the tooth is broken off, and the pulp (nerve) of the tooth is visible in the center of the tooth (it is red and may bleed), endodontics (root canal therapy) is usually required (p. 40), and a crown (cap) usually must be placed on the tooth.

5. Severely Broken Tooth (Fig. 12.4): Occasionally, teeth may be broken to the extent that none of the coronal portion shows when you open your mouth. The root portion of the tooth may be visible below the gum line. If such a tooth can be saved, it almost always requires endodontic (root canal) therapy (p. 40), a reinforcement post, and an extensive crown (cap) (p. 146).

FIG. 12.4 Severely broken tooth requiring endodontics (root canal therapy).
(From Tyldesley WR: Colour atlas of orofacial diseases, ed 2, St Louis, 1991, Mosby [Wolfe]. Copyright 1991 by WR Tyldesley.)
If the tooth has fractured vertically into the root (which is segregated into two portions), it almost always requires extraction and the necessary replacement procedures (p. 92). A few heroic bonding procedures may save the tooth.
If the tooth is lost, or if replanting is considered unacceptable, the same replacement procedures for an extracted tooth are necessary (fixed prosthodontics, p. 139).
7. Tooth Appears Gray or Pink (Fig. 12.5): A gray tooth usually has a dead pulp (nerve) and requires endodontic (root canal) therapy (p. 40). A pink tooth may have an enlarged pulp (nerve) and may require endodontic (root canal) therapy (p. 40). In severe situations in which teeth appear gray or pink, extraction may be necessary (p. 92).

8. Swelling in the Jaws or Neck (Fig. 12.6): Swelling in the mouth, upper or lower jaw, or neck that has come on rapidly is probably associated with a diseased tooth. Treatment of the swelling probably requires drainage and endodontics (root canal therapy) on a specific tooth (p. 40). Severely diseased teeth that have caused swelling may require removal of one or more teeth (p. 92).
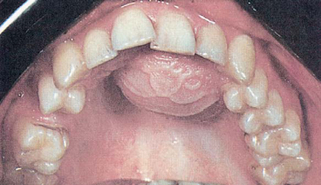
FIG. 12.6 Swelling in palate related to diseased tooth.
(From Tyldesley WR: Colour atlas of orofacial diseases, ed 2, St Louis, 1991, Mosby [Wolfe]. Copyright 1991 by WR Tyldesley.)
Swelling that slowly develops (Fig. 12.7) in the upper or lower jaws or the neck over a period of months or years is usually some form of tumor or cyst, and it should have professional observation as soon as the swelling is recognized. Such swellings are usually not associated with teeth, but they may require a biopsy (small piece of tissue to be observed under a microscope) (p. 91) and/or surgery for removal.

9. Pain in Tooth: A carious (decayed) tooth can cause pain (Fig. 12.8), but it may require only a restoration (filling) or endodontics (root canal therapy) (p. 40) and a restoration (filling), or an extraction (p. 92). Pain in a tooth does not necessarily require an extraction.

FIG. 12.8 Decayed teeth, resulting in severe toothache when the person eats sweets.
(From Tyldesley WR: Colour atlas of orofacial diseases, ed 2, St Louis, 1991, Mosby [Wolfe]. Copyright 1991 by WR Tyldesley.)
10. Sensitivity to Pressure on a Specific Tooth: A pressure-sensitive tooth usually calls for endodontics (root canal therapy) (p. 40). However, the tooth may have had root canal therapy already and may need further endodontic treatment or extraction (p. 92). Pressure sensitivity can also be caused by a heavy occlusion (bite) (p. 74), excessive bruxism or clenching (grinding teeth) (p. 76), or a crack in the tooth (p. 142).
11. Pus Oozing From Gums (Fig. 12.9): Pus oozing from gums usually indicates teeth that are in the late stages of periodontal disease. Such teeth require either periodontal (gum and bone) surgery or tooth extraction.
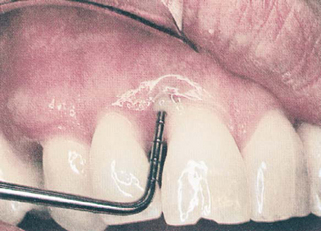
FIG. 12.9 Oozing pus from gums caused by periodontal disease (bone and gum degeneration).
(From Tyldesley WR: Colour atlas of orofacial diseases, ed 2, St Louis, 1991, Mosby [Wolfe]. Copyright 1991 by WR Tyldesley.)
12. Pimple Protruding From Gums (Fig. 12.10): A pimple on the gum usually indicates a dead pulp (nerve) of a tooth; the pimple provides an escape of pus from the root end of the tooth. Such teeth can usually be treated by endodontics (root canal therapy) (p. 40), apicoectomy (surgical removal of a small piece of tooth root and filling of the root canal on the root end) (p. 41), or, in extreme cases, extraction of the offending tooth (p. 92).

FIG. 12.10 Pimple on gum caused by diseased tooth.
(From Tyldesley WR: Colour atlas of orofacial diseases, ed 2, St Louis, 1991, Mosby [Wolfe]. Copyright 1991 by WR Tyldesley.)
13. Decayed Teeth (Fig. 12.11): Dental caries (decay) whether small, medium, or large, can usually be treated by simple restorations (fillings) (p. 170) or crowns (caps) (p. 146). Only long-neglected dental caries (decay) destroys teeth sufficiently to require extraction (p. 92).

14. Crooked Teeth (Fig. 12.12): Crooked teeth should be straightened by orthodontic therapy (p. 107). However, occasionally there are too many teeth for the size of the jaws, or the teeth are too large for the space present, and some teeth must be extracted before orthodontics can be accomplished.

FIG. 12.12 Crooked teeth in a child, requiring extraction of primary (baby) teeth.
(From Cameron A, Widmer R: Handbook of pediatric dentistry, London, 1997, Mosby-Wolfe.)
15. Chronic Tooth Pain (Fig. 12.13): Long-standing chronic pain in a tooth requires definitive diagnosis. The tooth/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


