12 Inflammatory Salivary Gland Disorders
Mucocele
Clinical Findings
• Mucoceles are most common in the first 3 decades of life.
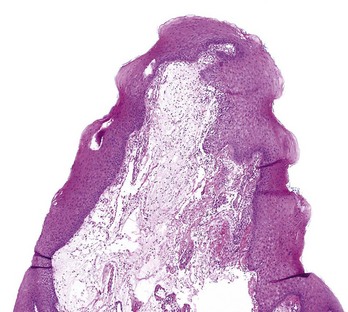
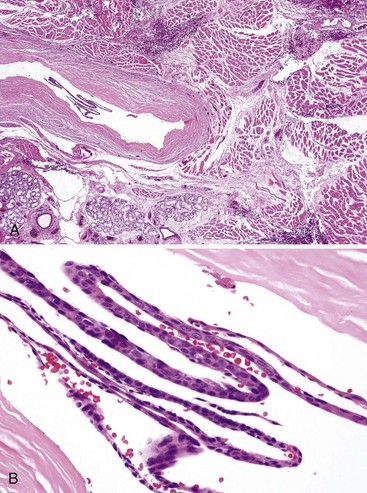
• Dome-shaped, bluish, sessile nodules, mucoceles are commonly located on the lower labial mucosa (70% to 90%), ventral tongue (ranula), buccal mucosa, and floor of mouth; they wax and wane and are usually painless (Fig. 12-1, A-C); 44% of mucoceles resolve spontaneously.
• Superficial mucoceles are seen in patients with hyposalivation; they are most frequent on the palate (such as in patients with chronic graft-versus-host disease) and resemble painless blisters or vesicles, often leading to a clinical misdiagnosis of herpes infection (see Fig. 12-1, D); the latter are almost always extremely painful.

Etiopathogenesis and Histopathologic Features
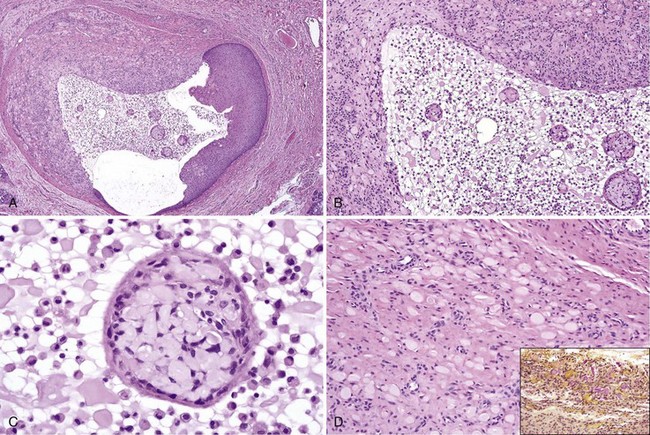
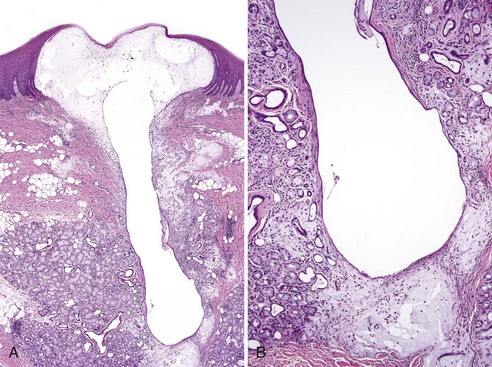
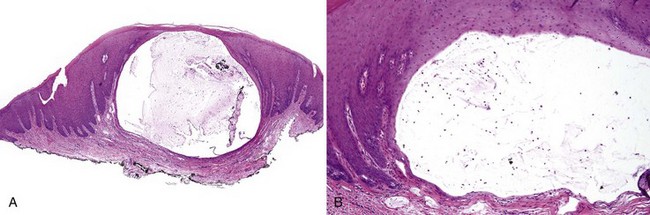
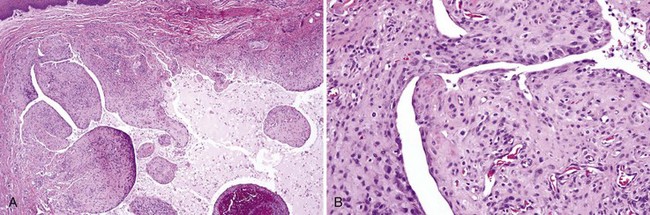
• Cystlike cavity fills with mucin with variable numbers of neutrophils, muciphages, and, sometimes, eosinophilic spherules surrounded by condensed granulation tissue containing muciphages; these globules are mucicarmine positive and may represent mucin condensations; a feeder duct exhibiting squamous metaplasia may be seen; mucin may be inconspicuous within the wall (Figs. 12-2 and 12-3).
• Mucin may be present diffusely in the connective tissue (Fig. 12-4); lesions not removed intact manifest as fragments of granulation tissue with muciphages (Fig. 12-5); ventral tongue lesions tend not to have a thick wall of granulation tissue (Fig. 12-6).
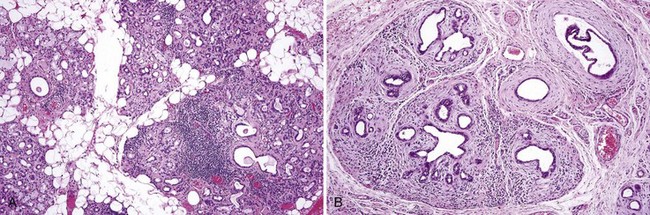
• Minor salivary glands exhibit variable degrees of obstructive changes, namely acinar atrophy, ductal dilatation with inspissated secretions, periductal hyalinization, interstitial fibrosis, and interstitial lymphoplasmacytic infiltrate (Fig. 12-7).
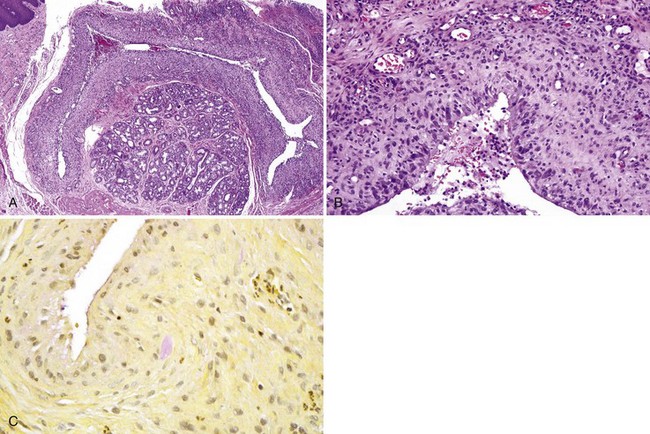
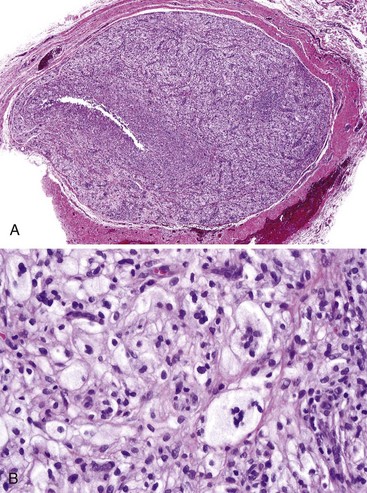
• Organizing mucoceles consist of a solid mass of granulation tissue with muciphages; mucin generally is inconspicuous, and a mucin pool is absent (Fig. 12-8); muciphages may sometimes have clear cytoplasm (Fig. 12-9).
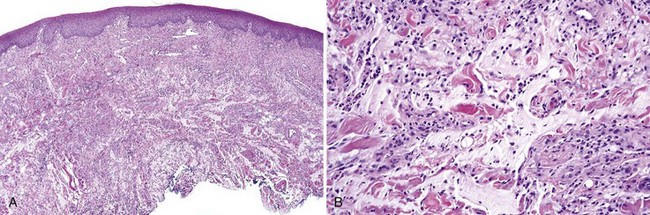
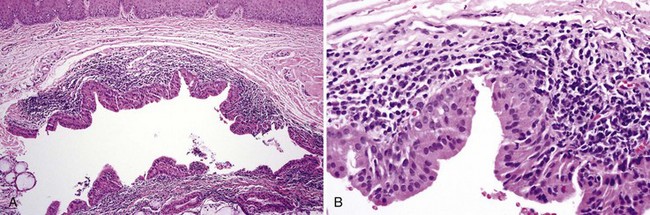
• Superficial mucoceles contain mucin pools that abut the overlying atrophic epithelium; a collarette of epithelium forms part of the wall of the mucocele (Figs. 12-10 and 12-11).
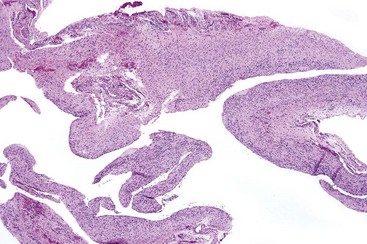
• Papillary synovium–like areas are sometimes seen (Fig. 12-12).
Differential Diagnosis
• An organizing mucocele with a predominance of clear cells may resemble salivary gland neoplasm such as mucoepidermoid carcinoma or even clear cell carcinoma, but there is lack of stromal invasion by nests of neoplastic cells.
• Obstructive changes are often diffuse and should not be confused with autoimmune sialadenitis seen in Sjögren syndrome, in which obstructive changes are minimal and the lymphocytic infiltrate is strikingly periductal, at least in early stages (see later); focal periductal lymphocytic infiltrates are not uncommon in obstructive sialadenitis.
Bermejo A, Aguirre JM, Lopez P, Saez MR. Superficial mucocele: report of 4 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1999;88:469-472.
Campana F, Sibaud V, Chauvel A, et al. Recurrent superficial mucoceles associated with lichenoid disorders. J Oral Maxillofac Surg. 2006;64:1830-1833.
Chi AC, Haigney RJ2nd, Spagnoli DB, et al. Papillary synovial metaplasia-like change in oral mucoceles: a rare and previously undescribed histopathologic variant of a common oral lesion. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010;109:268-273.
Chi AC, Lambert PR3rd, Richardson MS, Neville BW. Oral mucoceles: a clinicopathologic review of 1,824 cases, including unusual variants. J Oral Maxillofac Surg. 2010;69:1086-1093.
Minguez-Martinez I, Bonet-Coloma C, Ata-Ali-Mahmud J, et al. Clinical characteristics, treatment, and evolution of 89 mucoceles in children. J Oral Maxillofac Surg. 2010;68:e2468-e2471.
Sugerman PB, Savage NW, Young WG. Mucocele of the anterior lingual salivary glands (glands of Blandin and Nuhn): report of 5 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2000;90:478-482.
Treister NS, Cook EFJr, Antin J, et al. Clinical evaluation of oral chronic graft-versus-host disease. Biol Blood Marrow Transplant. 2008;14:110-115.
Salivary Duct Cyst (Salivary Retention Cyst, Sialocyst)
Etiopathogenesis and Histopathologic Features
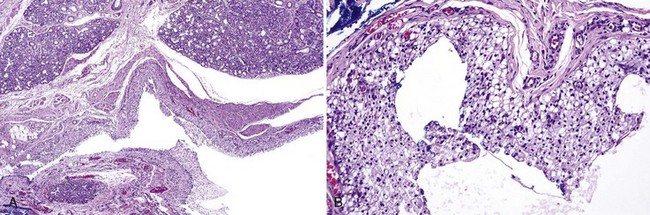
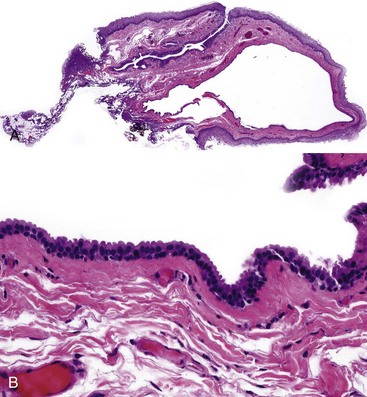
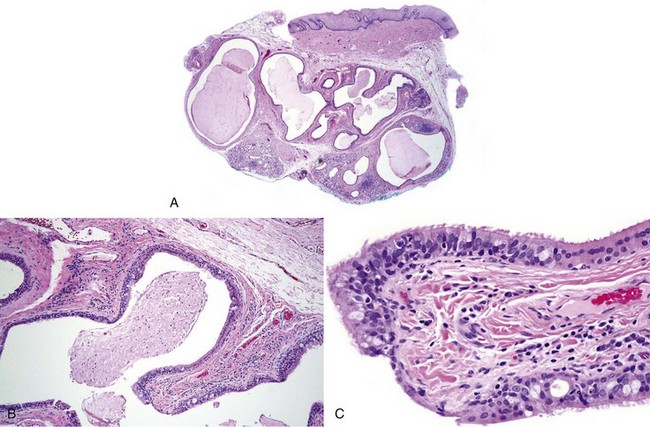
• These cysts consist of cystically dilated excretory salivary duct that may be lined by a double layer of low cuboidal-to-columnar cells or may exhibit metaplastic change—squamous, ciliated cell, or oncocytic (oncocytic sialocyst); it may have slight papillary projections in the lining (Figs. 12-13 to 12-15); a sialolith may be present; variable lymphoplasmacytic infiltrate present.
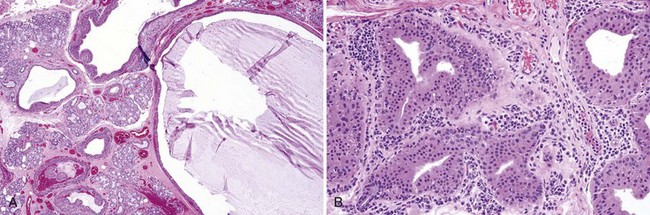
• Oncocytic sialocystosis (papillary or otherwise) shows multiple cystic structures in both extralobular and intralobular locations; surrounding minor glands exhibit obstructive changes (see Mucocele) (Figs. 12-16 and 12-17); should not be overdiagnosed as papillary cystadenoma.
Differential Diagnosis
• Multifocality and lack of encapsulation or significant adenomatous component differentiates sialocystosis from cystadenoma, although distinction may be difficult (see Chapter 13).
• Gingival cyst of the adult is often mistaken for salivary duct cyst, but the latter does not occur on the attached gingiva, which has no salivary glands.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


