Vitamins Required for Oral Soft Tissues and Salivary Glands
• Educate the patient on oral soft tissue changes that occur in a B-complex deficiency.
• Differentiate between scientifically-based evidence versus food fads concerning vitamins.
• Explain to a patient who is a vegan why vitamin B12 is important and identify appropriate sources.
• Compare and contrast the functions and sources of vitamins and minerals important for healthy oral soft tissues, as well as deficiencies, toxicities, and associated symptoms.
• Identify dental considerations for vitamins closely involved in maintaining healthy oral soft tissues.
• Discuss nutritional directions for vitamins closely involved in maintaining healthy oral soft tissues.
 Test Your NQ
Test Your NQ
1. T/F Milk is a good source of riboflavin.
2. T/F Vitamin B6 is the sunshine vitamin.
3. T/F Beriberi is caused by niacin deficiency.
4. T/F Vegans may be prone to vitamin B12 deficiency.
5. T/F Complaints of flushing and intestinal disturbances are symptoms of thiamin toxicity.
6. T/F A smooth purplish red or magenta tongue may be observed in patients with vitamin B6 deficiency.
7. T/F Enriched breads and cereals are good sources of thiamin.
8. T/F Carrots are a good source of folate.
9. T/F Thiamin requirement is determined by one’s energy requirement.
10. T/F The first signs of a nutritional deficiency often occur in the oral cavity.
Physiology of Soft Tissues
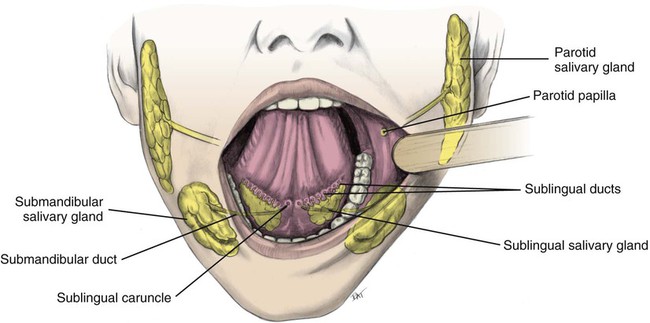
The systemic circulation provides nutrients and removes metabolic waste products from underlying structures and the salivary glands via the blood supply. Figure 11-1 shows healthy gingiva; changes in color, size, shape, texture, and functional integrity of the oral tissues often reflect systemic nutritional disorders. Signs and symptoms in soft oral tissues can be caused by deficiencies of many of the B-complex vitamins, vitamins C and E, iron, and protein (Box 11-1). Nutritional deficiencies result in similar oral signs and symptoms, such as pain, erythema, atrophy of tissues, and infection. Pyogenic (producing pus) and fungating (skin lesions with ulcerations, necrosis, and foul smell) microorganisms cause local infections in cracked epithelial surfaces. Approximately 90% of saliva is produced and secreted by three paired sets of major salivary glands: the parotid, submandibular, and sublingual glands (Fig. 11-2). Additionally, the lips and inner lining of the cheeks are equipped with hundreds of minor salivary glands.

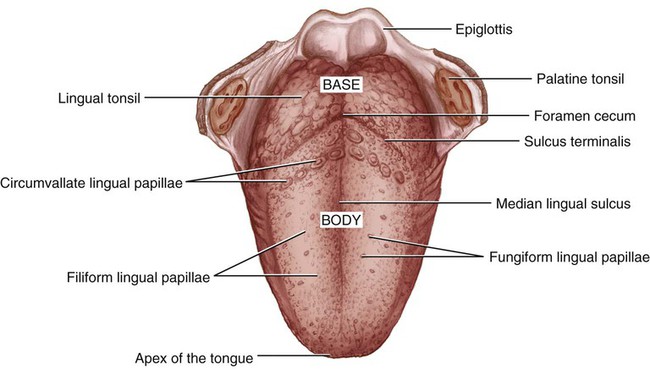
Mucosal cells have a very rapid turnover rate, resulting in complete turnover in 3 to 5 days. Rapid generation of new cells in the oral epithelia provides replacement tissue for trauma resulting from friction of the teeth and mastication. Additionally, hundreds of cells in the filiform papillae and fungiform papillae are in constant transition, from their anabolism until their catabolism (Fig. 11-3). Filiform papillae are smooth, threadlike structures on the dorsum surface of the tongue, whereas fungiform papillae are red, mushroom-shaped structures scattered throughout the filiform papillae.
 Dental Considerations
Dental Considerations
• Because of rapid turnover rate of oral tissues, the first signs of nutritional deficiency are frequently evident in the oral cavity. The glossal epithelium is usually the first to be affected, followed by areas around the lips. Assess patients for oral signs of nutritional deficiencies.
• The tongue may become edematous as a result of disease or nutritional deficiency.
• Angular cheilitis or cheilosis (cracks around the corners of the mouth) and glossitis (inflammation of the tongue) are commonly associated with deficiencies of several B-complex vitamins.
• Saliva aids in the ability to speak properly, and taste and swallow foods.
• The composition of saliva affects taste and can be a determining factor in food choices.
• Xerostomia may result in increased incidence of caries, stomatitis (inflammation of oral mucosa), gingival inflammation, and greater susceptibility to oral infections (see Chapter 19).
• Saliva may be used to diagnose some local and systemic diseases and heavy-metal toxicity, such as mercury toxicity.
• Salivary secretion is controlled primarily by cholinergic (nerves stimulated by acetylcholine) parasympathetic (autonomic) nerves; patients taking anticholinergic medications (which usually contain atropine) exhibit decreased salivary flow. These medications may be prescribed for bradycardia (low heart rate), diarrhea, peptic ulcers, and occasionally asthma.
 Nutritional Directions
Nutritional DirectionsThiamin (Vitamin B1)
Physiological Roles
Requirements
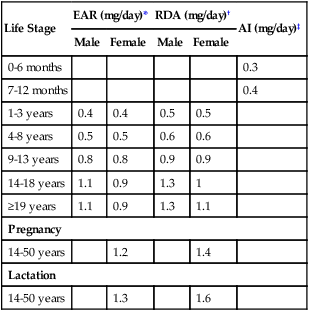
Thiamin is involved in using carbohydrates as kilocalories; the requirement is based on total caloric need. The recommended dietary allowance (RDA) for men (≥14 years old) is 1.2 mg/day and for women (≥19 years old) is 1.1 mg/day (Table 11-1). Participation in rigorous physical activity uses more energy, so more thiamin is required. Also, requirements are increased by pregnancy and lactation, hemodialysis or peritoneal dialysis, fever, hyperthyroidism, cardiac conditions, alcoholism, and the use of loop diuretics. No known adverse effects are evident from excessive thiamin intake, including supplements. Although a tolerable upper intake level (UL) is not established for thiamin, care should be taken when consumption routinely exceeds the RDA.
Table 11-1
Institute of Medicine recommendations for thiamin
| Life Stage | EAR (mg/day)* | RDA (mg/day)† | AI (mg/day)‡ | ||
| Male | Female | Male | Female | ||
| 0-6 months | 0.2 | ||||
| 7-12 months | 0.3 | ||||
| 1-3 years | 0.4 | 0.4 | 0.5 | 0.5 | |
| 4-8 years | 0.5 | 0.5 | 0.6 | 0.6 | |
| 9-13 years | 0.7 | 0.7 | 0.9 | 0.9 | |
| 14-18 years | 1 | 1 | 1.2 | 1 | |
| ≥19 years | 1 | 0.9 | 1.2 | 1.1 | |
| Pregnancy | |||||
| 14-50 years | 1.2 | 1.4 | |||
| Lactation | |||||
| 14-50 years | 1.2 | 1.4 | |||
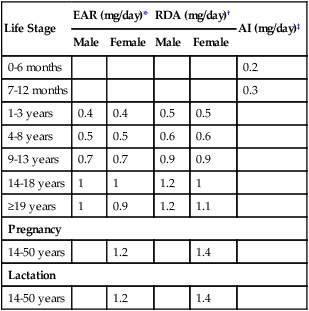
*EAR (estimated average requirement)—the intake that meets the estimated nutrient needs of half of the individuals in a group.
†RDA (recommended dietary allowance)—the intake that meets the nutrient needs of almost all (97% to 98%) individuals in a group.
‡AI (adequate intake)—the observed average or experimentally set intake by a defined population or subgroup that seems to sustain a defined nutritional status, such as growth rate, normal circulating nutrient values, or other functional indicators of health. An AI is used if insufficient scientific evidence is available to derive an EAR. For healthy human milk–fed infants, the AI is the mean intake. The AI is not equivalent to a RDA.
Data from Institute of Medicine (IOM), Food and Nutrition Board: Dietary reference intakes for thiamin, riboflavin, niacin, vitamin B6, folate, vitamin B12, pantothenic acid, biotin, and choline, Washington, DC, 1998, National Academy Press.
Sources
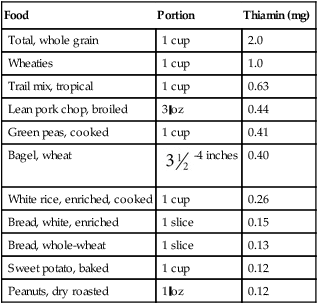
Thiamin is widely distributed in foods, and intake of a variety of foods, including enriched grains or whole grains, can ensure adequate amounts (Table 11-2). Approximately 40% of thiamin intake is provided by enriched breads, cereals, and pasta. (Because of enrichment, enriched breads may contain almost twice as much thiamin as whole grains). In the meat group, pork is an exceptionally good source. Other good sources include nuts and legumes. Following the guidelines for MyPlate and eating a variety of foods ensures adequate intake.
Table 11-2
Thiamin content of selected foods
| Food | Portion | Thiamin (mg) |
| Total, whole grain | 1 cup | 2.0 |
| Wheaties | 1 cup | 1.0 |
| Trail mix, tropical | 1 cup | 0.63 |
| Lean pork chop, broiled | 3 oz | 0.44 |
| Green peas, cooked | 1 cup | 0.41 |
| Bagel, wheat |  -4 inches -4 inches |
0.40 |
| White rice, enriched, cooked | 1 cup | 0.26 |
| Bread, white, enriched | 1 slice | 0.15 |
| Bread, whole-wheat | 1 slice | 0.13 |
| Sweet potato, baked | 1 cup | 0.12 |
| Peanuts, dry roasted | 1 oz | 0.12 |
Data from U.S. Department of Agriculture, Agricultural Research Service. USDA national nutrient database for standard reference, release 26, 2013. Nutrient Data Laboratory Home Page. Accessed August 30, 2013. Available at: http://www.ars.usda.gov/nutrientdata
Hypo States
Whether or not a thiamin deficiency is evident in oral tissues is controversial. Some clinicians have associated a flabby, red, and edematous tongue with thiamin deficiency (Fig. 11-4). The fungiform papillae become enlarged and hyperemic (engorged with blood).

 Dental Considerations
Dental Considerations
• A careful medical, social, and dietary history, including a clinical assessment of the oral cavity, alcohol consumption, and activity level, help identify early stages of thiamin deficiency.
• Risk of alcohol abuse or dependence is based on how much and how often an individual drinks. Moderation is considered 4 to 14 drinks per week for men and 3 to 11 drinks per week for women; five or more drinks per occasion is considered excessive for any adult.
• Vitamin deficiencies seldom occur in isolation. If a deficiency is suspected, symptoms of other vitamin B deficiencies also may be present.
• Because thiamin is essential for carbohydrate metabolism, a thiamin deficiency is closely linked to aberrations of brain function. For patients who are confused or have altered thought processes, assess nutrient intake.
• Carbohydrate loading or a very-high-carbohydrate diet and high physical activity slightly increase the thiamin requirement. (Generally, increased food intake results in increased thiamin consumption.)
• Thiamin deficiency has been reported in patients after gastrectomy and bariatric surgery (gastric bypass) related to decreased absorption.
• Although immediate clinical response to thiamin therapy is often dramatic, ultimate recovery may be incomplete, and relapses may occur, especially if precipitating factors persist.
• Massive amounts (1000 times greater than the RDA) of thiamin suppress the respiratory system and cause death.
 Nutritional Directions
Nutritional Directions
• Raw fish contains an active enzyme, thiaminase, which destroys thiamin.
• Baking soda added to cooking water to enhance the color of vegetables destroys thiamin.
• Overcooking and high temperatures destroy thiamin.
• Antacids reduce use of thiamin.
• Some diuretics can increase thiamin excretion.
• The RDA is higher than the average need for an individual. If the amount consumed is slightly under the listed RDA, most individuals will still be healthy. However, the lower the requirement of a vitamin or mineral, the greater the risk of a deficiency.
Riboflavin (Vitamin B2)
Physiological Roles
Requirements
As shown in Table 11-3, the Institute of Medicine (IOM) recommends an intake of 1.3 mg/day for men (14 years old and older) and 1.1 mg/day for women (19 years old and older). This level is influenced by individual energy requirements. Additionally, when nitrogen balance is positive, more riboflavin is retained. No UL has been established.
Table 11-3
Institute of Medicine recommendations for riboflavin
| Life Stage | EAR (mg/day)* | RDA (mg/day)† | AI (mg/day)‡ | ||
| Male | Female | Male | Female | ||
| 0-6 months | 0.3 | ||||
| 7-12 months | 0.4 | ||||
| 1-3 years | 0.4 | 0.4 | 0.5 | 0.5 | |
| 4-8 years | 0.5 | 0.5 | 0.6 | 0.6 | |
| 9-13 years | 0.8 | 0.8 | 0.9 | 0.9 | |
| 14-18 years | 1.1 | 0.9 | 1.3 | 1 | |
| ≥19 years | 1.1 | 0.9 | 1.3 | 1.1 | |
| Pregnancy | |||||
| 14-50 years | 1.2 | 1.4 | |||
| Lactation | |||||
| 14-50 years | 1.3 | 1.6 | |||
*EAR (estimated average requirement)—the intake that meets the estimated nutrient needs of half of the individuals in a group.
†RDA (recommended dietary allowance)—the intake that meets the nutrient needs of almost all (97% to 98%) individuals in a group.
‡AI (adequate intake)—the observed average or experimentally set intake by a defined population or subgroup that seems to sustain a defined nutritional status, such as growth rate, normal circulating nutrient values, or other functional indicators of health. An AI is used if insufficient scientific evidence is available to derive an EAR. For healthy human milk–fed infants, the AI is the mean intake. The AI is not equivalent to a RDA.
Data from Institute of Medicine (IOM), Food and Nutrition Board: Dietary reference intakes for thiamin, riboflavin, niacin, vitamin B6, folate, vitamin B12, pantothenic acid, biotin, and choline, Washington, DC, 1998, National Academy Press.
Sources
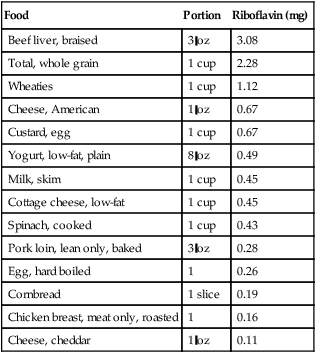
Although milk and milk products are excellent sources of riboflavin, approximately 30% of the dietary intake is furnished by foods in the grain group (Table 11-4). Meat, poultry, and fish also provide about one-fourth of the dietary requirement.
Table 11-4
Riboflavin content of selected foods
| Food | Portion | Riboflavin (mg) |
| Beef liver, braised | 3 oz | 3.08 |
| Total, whole grain | 1 cup | 2.28 |
| Wheaties | 1 cup | 1.12 |
| Cheese, American | 1 oz | 0.67 |
| Custard, egg | 1 cup | 0.67 |
| Yogurt, low-fat, plain | 8 oz | 0.49 |
| Milk, skim | 1 cup | 0.45 |
| Cottage cheese, low-fat | 1 cup | 0.45 |
| Spinach, cooked | 1 cup | 0.43 |
| Pork loin, lean only, baked | 3 oz | 0.28 |
| Egg, hard boiled | 1 | 0.26 |
| Cornbread | 1 slice | 0.19 |
| Chicken breast, meat only, roasted | 1 | 0.16 |
| Cheese, cheddar | 1 oz | 0.11 |
Data from U.S. Department of Agriculture, Agricultural Research Service. USDA national nutrient database for standard reference, release 26, 2013. Nutrient Data Laboratory Home Page. Accessed August 30, 2013: http://www.ars.usda.gov/nutrientdata
Hypo States
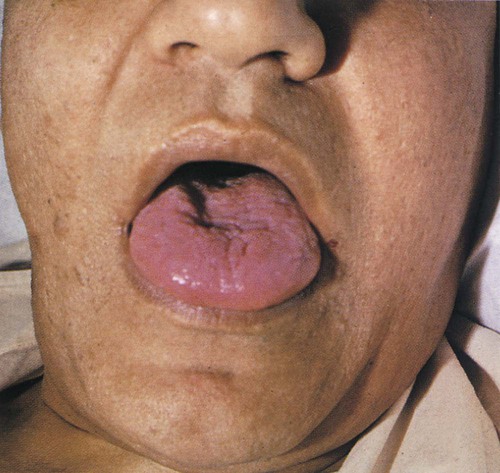
Symptoms associated with riboflavin deficiency, or ariboflavinosis, include angular cheilitis (Fig. 11-5), glossitis (Fig. 11-6), dermatitis, and anemia. With consistently inadequate intake, these symptoms may be observed within 8 weeks. Along with angular cheilosis, the lips may become extremely red and smooth. Fungiform papillae become swollen and slightly flattened and mushroom-shaped during early stages of riboflavin deficiency; the tongue has a pebbly or granular appearance. Severe chronic deficiencies lead to progressive papillary atrophy and patchy, irregular denudation of the tongue. The tongue may become purplish red or magenta in color because of vascular proliferation and decreased circulation. In more advanced cases, the entire tongue may become atrophic and smooth (Fig. 11-6). These symptoms, especially glossitis and dermatitis, may be secondary to vitamin B6 deficiency.

 Dental Considerations
Dental Considerations
• Hyperthyroidism, fevers, the added stress of injuries or surgery, excessive alcohol consumption, and malabsorption syndromes increase riboflavin requirements. Assess patients with these conditions for signs of deficiency: cheilitis, papillary atrophy, glossitis, and dermatitis.
• Congenital facial abnormalities may occur if the mother is deficient in riboflavin at the time of conception.
• Bilateral cheilosis may not be due to riboflavin deficiency; consider improperly constructed dentures, fungal (candidiasis) or yeast infection, and aging that may contribute to cheilosis.
• Phenothiazines and antibiotics increase excretion of riboflavin, so monitor for a deficiency in patients on long-term therapy.
 Nutritional Directions
Nutritional Directions
• Enriched products provide more riboflavin than their whole-grain counterparts.
• Lighted display cases have the potential to cause decomposition of riboflavin when milk is marketed in translucent plastic containers.
• A mixed diet that contains a pint of low-fat milk and 4 to 6 oz of meat daily ensures adequate riboflavin intake.
• Vegans and those who consume minimal or no dairy products are at risk of developing riboflavin deficiency.
• Riboflavin is not known to be toxic, but there is no benefit from high doses.
Niacin (Vitamin B3)
Physiological Roles
Requirements
The body obtains niacin not only directly from food, but also indirectly from conversion of an amino acid, tryptophan, and from synthesis by intestinal microorganisms. RDAs are given in terms of niacin equivalents, which include dietary sources of niacin plus its precursor, tryptophan. Approximately 1 mg of niacin may be formed from 60 mg of dietary tryptophan. Niacin requirements are related to caloric intake. The RDA niacin equivalents for adults are 14 to 16 mg daily (Table 11-5). The UL for adults is 35 mg daily. There is no known adverse effect related to naturally-occurring niacin in foods.
Table 11-5
Institute of Medicine recommendations for niacin
| Life Stage | EAR (mg/day)*† | RDA (mg/day)‡ | AI (mg/day)§ |
UL (mg/day) | ||
| Male | Female | Male | Female | |||
| 0-6 months | 2 | ND¶ | ||||
| 7-12 months | 4 | ND¶ | ||||
| 1-3 years | 5 | 5 | 6 | 6 | 10 | |
| 4-8 years | 6 | 6 | 8 | 8 | 15 | |
| 9-13 years | 9 | 9 | 12 | 12 | 20 | |
| 14-18 years | 12 | 11 | 16 | 14 | 30 | |
| ≥19 years | 12 | 11 | 16 | 14 | 35 | |
| Pregnancy | ||||||
| 14-18 years | 14 | 18 | 30 | |||
| ≥19 years | 14 | 18 | 35 | |||
| Lactation | ||||||
| 14-18 years | 13 | 17 | 30 | |||
| ≥19 years | 13 | 17 | 35 | |||
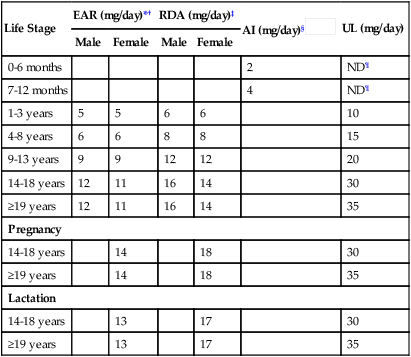
*EAR (estimated average requirement)—the intake that meets the estimated nutrient needs of half of the individuals in a group.
‡RDA (recommended dietary allowance)—the intake that meets the nutrient needs of almost all (97% to 98%) individuals in a group.
§AI (adequate intake)—the observed average or experimentally set intake by a defined population or subgroup that seems to sustain a defined nutritional status, such as growth rate, normal circulating nutrient values, or other functional indicators of health. An AI is used if insufficient scientific evidence is available to derive an EAR. For healthy human milk–fed infants, the AI is the mean intake. The AI is not equivalent to a RDA.

¶ND—not determinable because of lack of data of adverse effects in this age group and concern with regard to lack of ability to handle excess amounts. Source of intake should be from food and formula to prevent high levels of intake.
Data from Institute of Medicine (IOM), Food and Nutrition Board: Dietary reference intakes for thiamin, riboflavin, niacin, vitamin B6, folate, vitamin B12, pantothenic acid, biotin, and choline, Washington, DC, 1998, National Academy Press.
Sources
Niacin is widely distributed in plant and animal foods. Good sources include meats, cereals, legumes, seeds, and nuts (Table 11-6). Approximately 65% of the niacin in the U.S. diet is obtained from meat and milk. Tryptophan is found mainly in milk, eggs, and meats. The RDA for niacin equivalents is easily met by consuming foods high in niacin and foods containing tryptophan.
Table 11-6
Niacin content of selected foods
| Food | Portion | Niacin (mg) |
| Beef liver, braised | 3 oz | 15.77 |
| Wheaties | 1 cup | 13.32 |
| Chicken breast, skinless, cooked | 3 oz | 12.84 |
| Salmon, cooked | 3 oz | 8.24 |
| Halibut, broiled | 3 oz | 6.72 |
| Tuna, white, canned in water | 3 oz | 4.93 |
| Turkey, whole, cooked | 3 oz | 4.80 |
| Peanuts, dry roasted | 1 oz | 3.83 |
| Potato, white, baked | 1 med | 2.64 |
| Mushrooms, raw | 1 cup | 2.53 |
| Rice, enriched white, cooked | 1 cup | 2.33 |
| Milk, skim | 1 cup | 0.23 |

Data from U.S. Department of Agriculture, Agricultural Research Service. USDA national nutrient database for standard reference, release 26, 2013. Nutrient Data Laboratory Home Page. Accessed August 30, 2013: http://www.ars.usda.gov/nutrientdata
Hyper States and Hypo States
Supplemental doses of nicotinic acid (3 to 6 g/day) are effective in reducing low-density lipoprotein (LDL) cholesterol and triglycerides, while increasing high-density lipoprotein (HDL) cholesterol. (Nicotinamide does not function in this role.) Despite positive changes in serum lipid levels, a large study funded by National Institutes of Health using a combination of niacin supplements and statin did not reduce risk of CHD (heart attacks and strokes), causing the study to be terminated early.1,2
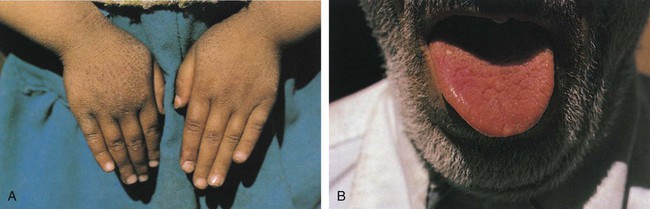
Niacin deficiency is usually associated with a maize (corn) diet because corn products contain all the essential amino acids except tryptophan. This diet increases the body’s requirements for tryptophan and niacin. A deficiency is also seen in alcoholics but is unlikely in individuals who consume adequate protein. Niacin deficiency results in degeneration of the skin, gastrointestinal tract, and nervous system, a condition known as pellagra. Symptoms of pellagra have been referred to as “the 4 Ds”—dermatitis, diarrhea, depression or dementia, and death. The term pellagra is derived from the Latin word for animal hide; the skin may become rough and resemble goose flesh. The most striking and characteristic sign of pellagra is a reddish skin rash, especially on the face, hands, or feet, which is always bilaterally symmetrical (i.e., appears on both sides of the body at the same time) (Fig. 11-7A). It flares up when skin is exposed to strong sunlight. Neurological symptoms include depression, apathy, headache, fatigue, and loss of memory. If untreated, it may lead to death.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


