Chapter 11
Atraumatic Piezosurgical Extractions: A Solution for Bone Preservation
HISTORICAL REVIEW
Pioneering work using ultrasonic devices for bone surgery began more than 30 years ago with Horton et al. (1975), shortly followed by Aro et al. (1981). Other practitioners, such as Vercellotti (2005), subsequently widened the field of application for piezosurgical instruments, and they developed considerably to extend their use to all types of buccal bone surgery. Improved control of powers and frequencies came hand in hand with new generations of tips, increasingly better adapted to clinical requirements. Today’s powers and frequencies (between 28 and 36 kHz) are optimal and are electronically controlled to adapt to different types of tissues encountered, allowing the practitioner to cut delicately and precisely. With piezosurgery, the timeworn image of oral surgeons with their hand pieces and bone scissors gives way to that of artists with paintbrushes.
Although preservation of bone tissue is one of the most important issues in modern dentistry, traumatic extractions still account for much of the bone losses that preclude implants and are simply no longer acceptable in aesthetic terms. In all complicated extraction cases, the Piezotome proves its worth as the instrument best adapted to limiting the destruction of bone tissue.
PIEZOSURGERY COMPARED WITH STANDARD TECHNIQUE
The action of piezoelectrical tips has still not been clearly established, but it is probably applied to the three tissue structures concerned—bone, ligament, and tooth—with varying degrees of efficiency. The practitioner can easily direct this action, however, by exercising a light pressure toward the tooth rather than the bone. Piezoelectrical tips operate more effectively on hard tissue than on soft, where their efficiency diminishes considerably (Louise and Macia 2009). Indeed, soft tissues are generally pushed back rather than sectioned. Because of this, literally caught between a rock and a hard place—the bone and the cementum—and unable to escape the vibratory action of the tip, the ligament is mechanically destructured. By applying light pressure toward the tooth, the practitioner allows the tip to glide over the bone and focus its action on the tooth, thus preserving the precious bone tissue.
One of the major advantages of tips is their shape. Combined with the oscillatory movement imparted by the ceramic pellets in the hand piece, this design allows the surgeon to use both the tip and the edges of these ultrasonic scalpels (Figure 11.1.) Long and slim, they can be slipped into spaces where not even a small-diameter drill could be used without collateral damage (Figure 11.2). In order to preserve bone, these inserts must follow the root as closely as possible, whatever its face and whatever the angular formation of the tooth. To facilitate this contact, the cutting faces of tips are now produced with different angulations to meet all situations (Figures 11.3–11.9).
Figure 11.1 Long and slim (working head 9 mm, thickness 0.5 mm), the Satelec extraction tip is easily slipped between root and bone, facilitating access toward fractured roots (the double yellow arrow matches the tip motion).

Figure 11.2 With their longitudinal oscillation, these (Satelec) tips can be used both along their edges and at the tip. Vibration amplitude is between 30 and 60 µm. The working head is 9 mm long and only 0.5 mm thick.
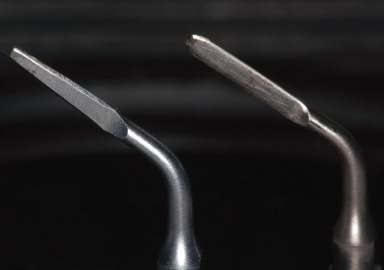
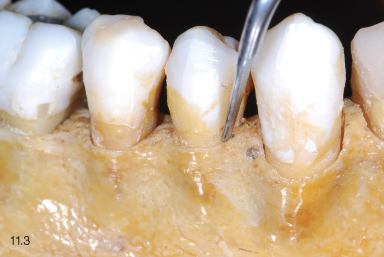
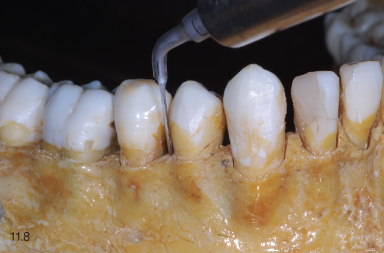
Figure 11.3 to Figure 11.9 Tips may be compared to root-surfacing curettes with “standard” straight instruments that can be used on all easily accessible sides of the teeth (Figures 11.3, 11.4) or simply on the buccal and lingual faces (Figure 11.5). These instruments come with a blade slightly angled to the right for access to two opposite angles (Figures 11.6, 11.7) and to the left for the other two angles (Figures 11.8, 11.9). Three instruments suffice for all teeth.





A trench up to 8 or 9 mm deep is cut around the tooth. This point of access allows the practitioner to slide a thin manual instrument down between the root and the bone. Because the long, narrow nature of the trench gives the instrument the necessary grip, only a slight rotational movement is required to create mobility and allow the avulsion of the tooth. The microvibrations transmitted by the tip gripped in this narrow sheath will oscillate toward the hardest tissue—the tooth itself—and thus help dissociate it from the bone.
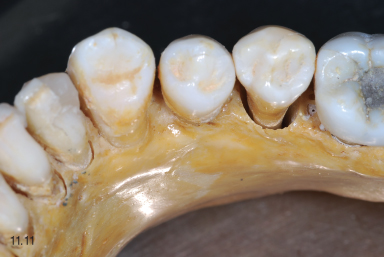
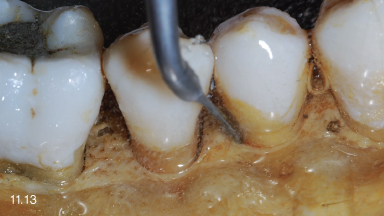
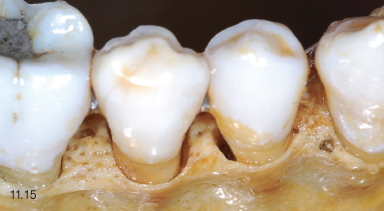
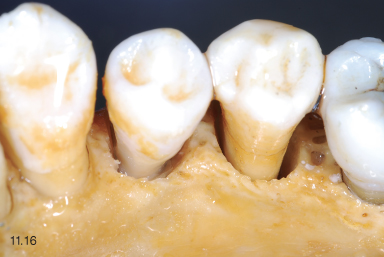
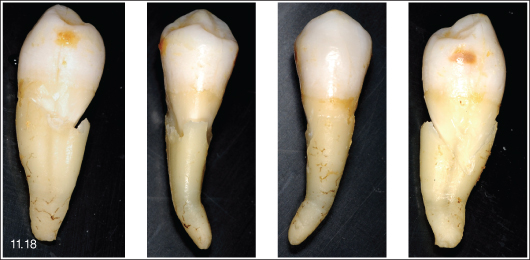
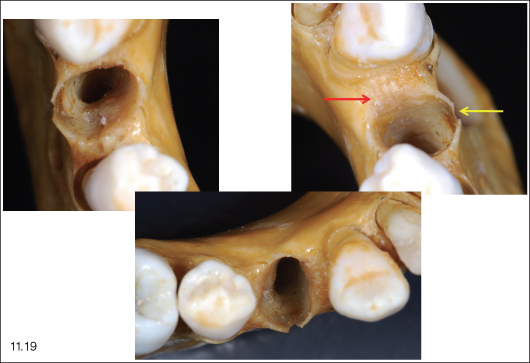
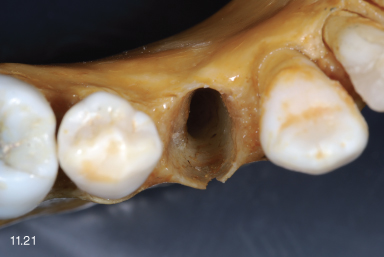
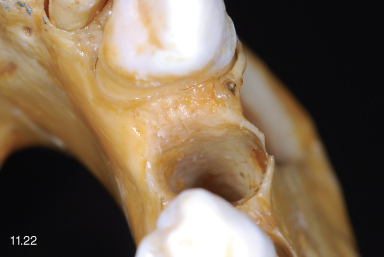
In order to observe the mechanical effect of the piezoelectrical tips on both bone and tooth, we used ultrasonic tips on a dried human jawbone (Figures 11.10–11.22). With neither organic matter nor hydration, both tissues were very hard, noncompressible, and thus highly reactive to ultrasound. A straight tip was used for the lingual side, with an angled tip to the right and another angled insert to the left for all four angles. They were introduced to a depth of 5–6 mm, slightly angled toward the tooth. So as not to destroy the fine cortical bone, the buccal side was barely opened. This compact vestibular bone is often very fine and must be protected from instruments during extractions. Once the encircling trench was completed, the tooth was easily extracted. We noted that except for a little chip on the vestibular rim, the socket was almost wholly preserved, notwithstanding the fragility of such dry, brittle bone. The crest of the socket was slightly enlarged to a height of around 1–2 mm and to a width corresponding to the thickness of the inserts (0.5 mm). This very minimal bone loss is highly favorable in support of the concept of immediate extraction/implant. Examination of the extracted tooth showed that, in order to preserve the bone, the trench had cut into the dental tissue. Sizeable marks, observed on the proximal and lingual sides, bore witness to the highly effective action of the ultrasonic tips. The pressure applied toward the tooth should thus be moderated to avoid weakening the root and running the risk of a fracture during the avulsion.
Figure 11.10 to 11.22 Use of straight and angled tips LC 2 R & L to extract a first premolar firmly bonded to the bone of a dry skull (Figures 11.10–11.14). By tilting the tip slightly (Figure 11.15), the cleavage zone is cut into the tooth itself. A trench is cut right round the tooth, except for the buccal side (Figure 11.16). Once the tooth is loosened, it is withdrawn (Figure 11.17), showing that the ultrasonic action was focused essentially on the root (Figure 11.18), safeguarding the alveolar bone socket. The only remaining traces are a slight buccal nick (yellow arrow) and a small surrounding trench of 1 to 2 mm (red arrow) (Figures 11.19–11.22).





Piezoelectrical tips do have an abrasive effect, however slight, on bone as a hard tissue. This is thus an inconvenience with respect to standard techniques, which do not destroy bone if successfully applied in moderately difficult extraction cases. In situations were action on the bone is necessary to extract the tooth, however, piezoelectrical tips are better suited, for the osteotomy is very delicate, easily controlled, and considerably less aggressive for the bony tissue.
In a study on dogs, Vercellotti et al. (2005) compared bone cicatrisation following osteotomy with diamond burs, carbide burs, and piezoelectrical tips. The rate of postoperative wound healing was compared at 14, 28, and 56 days. In comparison with baseline measurements, they noted that at 14 days the sites operated on with diamond or carbide burs had lost bone, whereas those treated/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


