CHAPTER 10 Medical and Dental Emergencies
EMERGENCY PREVENTION
The combination of pain, stress, infection, and anesthesia use in the dental setting may contribute to medical emergencies. Evaluation includes completion of a comprehensive health history, in-depth history of present illness, assessment of vital signs, physical assessment, and thorough emergency preparation in the dental setting. Instances of when to request a medical consult regarding a patient and/or when to consider a situation an emergency and activate the Emergency Medical Service (EMS) system are discussed in this chapter.
 •
• • See Chapters 6, General and Oral Pathology: pathological disorders risk for emergencies; 8, Microbiology and Immunology: allergic reactions in a dental setting; 9, Pharmacology, drugs in emergency kit in a dental setting; 14, Pain Management: local anesthesia and nitrous oxide administration emergencies in a dental setting.
HEALTH HISTORY
• See Chapters 9, Pharmacology: antibiotic premedication and Physician’s Desk Reference; 11, Clinical Treatment: health history; 18, Ethics and Jurisprudence: related ethical concerns.
A. Identifies changes in drugs and/or conditions that may require antibiotic premedication (e.g., valvular replacement and/or congenital heart disease or transplant).
D. May assist in identification of oral manifestations associated with some drugs or systemic diseases.
Vital Signs
• See Chapter 3, Anatomy, Biochemistry, and Physiology: physiology of blood pressure; Chapter 6, General and Oral Pathology: high blood pressure.
A. Blood pressure: force exerted by circulating blood on the walls of blood vessels.
1. Measured in terms of air pressure required to compress large artery to point of shutting off blood flow, reading recorded in fractions of millimeters of mercury (mm Hg), although mercury is NO longer used in most modern vascular devices because of possible toxicity. Measurements for healthy adult patient are usually <120/80; cannot feel blood pressure level.
3. Hypertension (high blood pressure [HBP]):
c. HBP can have two stages:
(1) Stage 1: Mild HBP (140 to 159/90 to 99 mm Hg):
4. Blood pressure affected by:
5. Technique for taking blood pressure reading: instruments used to measure blood pressure include stethoscope and sphygmomanometer (cuff size is determined by arm size, cuff too small or large will give false HBP reading); SIMILAR for digital devices; need to wait 2 to 3 minutes between readings for all types.
b. Cuff pumped until radial pulse is NO longer felt; note this point (estimated systolic number) and release the pressure.
B. Pulse rate frequency of the heart beat or rate, measured in beats per minute (BPM):
1. Taken from radial artery if patient is conscious (easy access) and from common carotid artery in unconscious patient (more accurate) for adults and brachial artery on infants but ONLY by EMS system personnel; fingers used for palpation, since thumb has own pulse.
2. Taken for 30 seconds if within range (number is multiplied by 2 if the rate is regular); if increased or irregular, taken again for 1 minute.
4. Affected by age, exercise, stress, drugs, stimulants, fasting, long-term illness, emotional state.
6. AVOID palpating carotid pulse unless EMS personnel (lack indicates death), since stimulating its baroreceptors with vigorous palpation can provoke severe bradycardia or even stop the heart in some sensitive persons; BOTH should not be palpated at the same time to AVOID risk of fainting or brain ischemia.
C. Respiration rate: obtained by counting number of breaths for 30 seconds (number is multiplied by 2 if rate is regular), one exhalation and one inhalation together count as one breath; if increased or irregular, taken again for 1 minute.
2. Normal rates can be altered if patient knows that breathing is being observed; overall rates can be affected by anxiety, pain, excitement, infection, presence of fever.
D. Temperature reading: taken with covered thermometer when needed because of signs of clinical infection or inflammation:
ASA Physical Classification
B. ASA II: mild systemic disease or healthy ASA I who demonstrates a MORE extreme anxiety and fear toward dentistry.
1. Able to walk up one flight of stairs or two level city blocks but will have to stop after completion because of distress.
C. ASA III: severe systemic disease that limits activity but is NOT incapacitating.
1. Able to walk up one flight of stairs or two level city blocks, but MUST stop enroute because of distress.
2. History of controlled chronic disease, which includes angina pectoris, myocardial infarction (MI), cerebrovascular accident (CVA), congestive heart failure (CHF) or cardiac surgery more than 4 to 6 weeks in the past, slight chronic obstructive pulmonary disease (COPD), controlled insulin-dependent DM/HBP (with drugs).
D. ASA IV: severe systemic disease that limits activity and is a constant threat to life.
1. NOT able to walk up one flight of stairs or two level city blocks; distress is present even at rest.
2. History of uncontrolled acute or chronic disease, which includes unstable angina pectoris, MI/CVA within the last 4 to 6 weeks, severe CHF, moderate to severe COPD, and uncontrolled HBP, epilepsy, DM, or thyroid condition.
PREPARATION FOR MEDICAL EMERGENCIES IN DENTAL SETTING
A. Basic emergency kit: MUST include:
1. Noninjectable drugs:
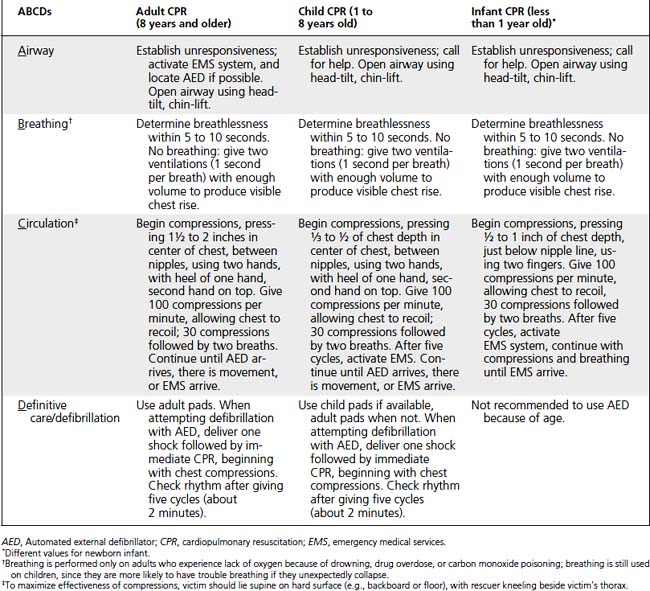
B. AED: portable electronic device that automatically diagnoses potentially life-threatening cardiac arrhythmias of ventricular fibrillation and ventricular tachycardia.
1. Arrhythmia can be treated by application of electrical therapy, which stops arrhythmia, allowing heart to reestablish effective rhythm.
2. When turned on or opened, unit will instruct user to connect the electrodes (pads) to patient:
a. Once pads are properly attached, everyone should AVOID touching victim to prevent false readings by unit.
b. Pads allow unit to examine electrical output from heart and determine if patient is in viable, shockable rhythm (either ventricular fibrillation or ventricular tachycardia); if device determines that a shock is viable, will use battery to charge internal capacitor in preparation to deliver shock.
C. Pulse oximeter: indirectly measures oxygen saturation and changes in blood volume in skin, producing a photoplethysmograph; useful for monitoring patients during surgical procedures.
2. Monitor displays percentage of arterial hemoglobin in the oxyhemoglobin configuration (possibly heart rate); acceptable normal ranges are from 95% to 100%; for a patient breathing room air at not far above sea level, estimate of arterial po2 can be made from blood-oxygen monitor SpO2 reading.
MEDICAL EMERGENCIES IN DENTAL SETTING
Syncope and Orthostatic Hypotension
A. Syncope (fainting): MOST common dental setting emergency; MOST common cause of loss of consciousness.
2. Caused by decreased oxygen flow to the brain, which in turn is caused by:
5. As with ALL emergencies that involve unconscious patient, may lead to airway obstruction and death if improperly recognized and treated.
6. Treatment:
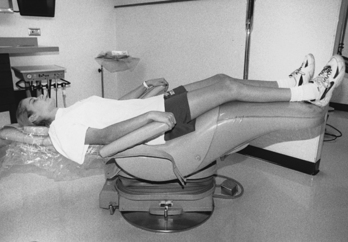
a. Place in Trendelenburg position (subsupine with feet elevated higher than head), EXCEPT for pregnant patient (on side before feet are elevated); usually ensures recovery (Figure 10-1).
b. Maintain open airway to prevent airway obstruction by tongue; imperative for unconscious patient.
c. Use of aromatic ammonia inhalant (amyl nitrate), as needed, to provide stimulus for breathing; caution is necessary during use to prevent burning of tissue.
B. Orthostatic (postural) hypotension:
1. May occur when patient sits up quickly from being in a supine position and may result in loss of consciousness (second MOST common cause of unconsciousness).
C. Hyperventilation: in dental setting usually related to anxiety.
1. Increased rate and depth of respirations, which results in decreased level of carbon dioxide.
2. Treatment:
a. Calm and place in upright position; respiratory emergencies SHOULD be managed with patient upright, if conscious.
D. Airway obstruction or foreign body airway obstruction (FBAO):
1. Occurs MORE easily in dental setting because of supine position; includes cotton rolls, extracted teeth or fragments, restorative materials, vomit.
2. Types of FBAO:
d. Treatment for conscious adult or child with complete or partial FBAO with poor air exchange is the SAME:
(2) Perform Heimlich maneuver: stand behind patient, wrap both arms around the patient and deliver abdominal thrusts (position flat portion of one fist between navel and bottom of rib cage; wrap other hand around fist), push inward and upward until object is expelled or patient becomes unconscious.
(4) Activate EMS system if patient becomes unconscious:
(a) Help patient to the floor or perform abdominal thrusts in the chair, straddling patient’s hips or standing close to hips at one side (if in dental unit).
(b) Place heel of one hand between navel and bottom of rib cage; position other hand above first, interlacing fingers; push inward and upward five times; then move to head and open airway.
CLINICAL STUDY
| Age | 33 YRS | SCENARIO |
| Sex | Male ⌧ Female | The patient dreads dental appointments but currently experiences less anxiety because she has been following 6-month oral prophylaxis schedule and her appointments take less time. Her dental health is good. After her medical history is updated and her vital signs are obtained, bitewing radiographs are taken. While the dental hygienist leaves to process the radiographs, the patient remains seated in an upright position. Upon returning to the patient, the dental hygienist notes that she is breathing rapidly, and she complains of tightness in her chest and tingling in her fingers. |
| B/P | 122/82 | |
| Chief Complaint | “I just hate being here and I hate all that happens here!” | |
| Medical History |
1. Probably experiencing hyperventilation, indicated by increased rate of respiration, dizziness, chest tightness, tingling in fingers. Most often occurs in the dental setting because of anxiety. Anxiety about dental appointments was a problem, although the patient believed it had lessened. Her recent personal loss and stressful career must also be taken into consideration.
2. Treatment includes calming her and keeping her positioned upright. Rapid rate of breathing results in decreased level of carbon dioxide. To restore carbon dioxide, patient should inhale, hold her breath, and then exhale. If this is ineffective, should breathe into paper bag 6 to 10 times/min (known as rebreathing); important to allow her to hold bag in position.
3. Hyperventilation is one emergency in which administration of oxygen is not indicated; although oxygen would not harm her, it would not benefit her.
Allergic Reactions
Allergic reactions, including asthmatic attacks, are common in a dental setting. MOST are due to increased sensitivity to allergen (antigen, foreign) that has entered the body (type I [immediate] hypersensitivity). A.Allergic reactions:
1. Immune system then releases chemicals, such as histamine from mast cells, resulting in varying degrees of reaction.
2. Skin reactions generally are NOT considered true emergencies; however, MUST be monitored for potential advancement; reactions may be localized or generalized, severity and type of reaction are related to type and amount of allergen to which patient is exposed.
3. If reaction occurs immediately after exposure, is MORE severe; when reaction occurs MORE than 60 minutes after exposure, LESS severe.
4. Types of hypersensitivity and allergic reactions:
c. Angioedema: initially may be mistaken for hives.
(1) Localized, unilateral, colorless and painless swellings of face or neck without well-defined borders of hives; allergic reaction to food or drug; affects tissues of the hands, face, genitals; rarely results in pain or itching.
(2) Treated by removing cause; referral to dermatologist or allergist, supervising dentist may administer antihistamine, such as diphenhydramine (Benadryl) or chlorpheniramine (Chlor-Trimeton), to reduce reaction; localized, mild allergic reactions should be treated with oral histamine blocker for minimum of 3 days because of risk of recurrence.
d. Anaphylaxis (anaphylactic reaction): MOST severe allergic reaction.
(1) Level depends on amount of allergen to which patient is exposed, acquired sensitivity, route of entry; occurs almost immediately after exposure; may be fatal despite treatment.
(2) Can be caused by foods, drugs (MOSTLY penicillin and related antibiotics), rubber latex, or other environmental factors.
(3) With allergy to local anesthetic agent (rare), MUST be determined if true allergic reaction or some other adverse reaction occurred.
(a) Allergic reaction occurs MORE often in response to ester injectable local anesthetic agents (e.g., procaine was removed from American market for this reason); allergic reactions to amide agents are rare; NO longer using injected ester agents, so has become rare with injectables.
(b) Allergy to preservative sodium metabisulfite (antioxidant for the vasoconstrictor) must also be considered; using plain local anesthetic, such as 2% lidocaine (Xylocaine), 3% carbocaine (Mepivacaine), or 4% prilocaine (Citanest), without any vasoconstrictor will prevent almost ALL local anesthetic-related allergic reactions.
(4) Symptoms affect different body systems and may occur separately or simultaneously:
(a) Begins rapidly as a skin response (pruritus, urticaria, angioedema); angioedema in mouth may result in airway obstruction.
(5) Treatment for anaphylaxis:
(a) Place in supine position, administer oxygen at 5 liters/min through nasal cannula; provide BLS as needed.
(b) Activate EMS system; epinephrine administration (0.3 mg every 5 minutes for adults, 0.15 mg for children; in some cases of systemic allergic reactions, clinical signs of bronchospasm and hypotension persist after FIRST dose of epinephrine) by supervising dentist when diagnosis is definite.
(c) Because of urgent nature of epinephrine administration in anaphylactic shock, prefilled syringes provide quicker, MORE foolproof method for administering; autoinjectors (EpiPen) are available to inject single adult or pediatric dose when pressed against the thigh (even through clothing) by patient or supervising dentist.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


