CHAPTER 20 Initial Placement, Adjustment, and Servicing of the Removable Partial Denture
Initial placement of the completed removable partial denture, the fifth of six essential phases of removable partial denture service mentioned in Chapter 2, should be a routinely scheduled appointment. All too often the prosthesis is quickly placed and the patient dismissed with instructions to return when soreness or discomfort develops. Patients should not be given possession of removable prostheses until denture bases have been initially adjusted as required, occlusal discrepancies have been eliminated, and patient education procedures have been continued.
Adjustments to Bearing Surfaces of Denture Bases
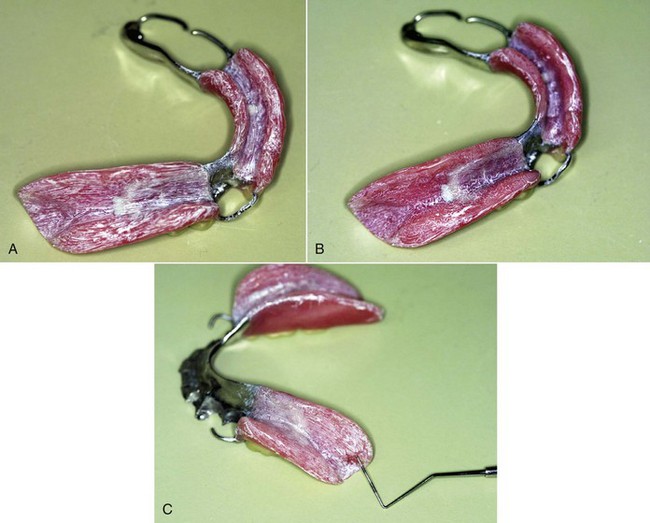
Altering bearing surfaces to perfect the fit of the denture to the supporting tissue should be accomplished with the use of some kind of indicator paste (Figure 20-1). The paste must be one that will be readily displaced by positive tissue contact and that will not adhere to the tissue of the mouth. Several pressure indicator pastes are commercially available. However, equal parts of a vegetable shortening and USP zinc oxide powder can be combined to make an acceptable paste. The components must be thoroughly spatulated to a homogeneous mixture. A quantity sufficient to fill several small ointment jars may be mixed at one time.
Adjustment of Occlusion in Harmony with Natural and Artificial Dentition
Occlusal adjustment of tooth-supported removable partial dentures may be performed accurately by any of several intraoral methods. Occlusal adjustment of distal extension removable partial dentures is accomplished more accurately with the use of an articulator than by any intraoral method. Because distal extension denture bases will exhibit some movement under a closing force, intraoral indications of occlusal discrepancies, whether produced by articulating paper or disclosing waxes, are difficult to interpret. Distal extension dentures positioned on remounting casts can conveniently be related in the articulator with new, nonpressure interocclusal records, and the occlusion can be adjusted accurately at the appointment for initial placement of the dentures (Figure 20-2).
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


