ENAMEL
• Composition
• Structure
• Thickness
• Color
• Strength
• Structure Present in Enamel
• Functions of Enamel
• Clinical Significance of Enamel
DENTIN
• Composition
• Color
• Thickness
• Hardness
• Structure of Dentin
• Difference between Enamel and Dentin
• Difference between Primary, Secondary and Reparative/ Tertiary Dentin
• Clinical Considerations of Dentin
DENTAL PULP
• Histology of Dental Pulp
• Structural or Cellular Elements
• Extracellular Components
• Anatomy of Dental Pulp
• Functions of Pulp
• Age Changes in Pulp
PERIRADICULAR TISSUE
• Cementurn
• Periodontal Ligament
• Alveolar Bone
Good knowledge of dental anatomy, histology, physiology and occlusion is the foundation stone of operative dentistry. In other words, thorough knowledge of morphology, dental anatomy, histology, is essential to get optimal results of operative dentistry. Though the dental tissues are passive, the occurrence of caries can only be understood when the structure of the teeth is understood.
The teeth consist of enamel, dentin, pulp and cementum (Fig. 3.1).
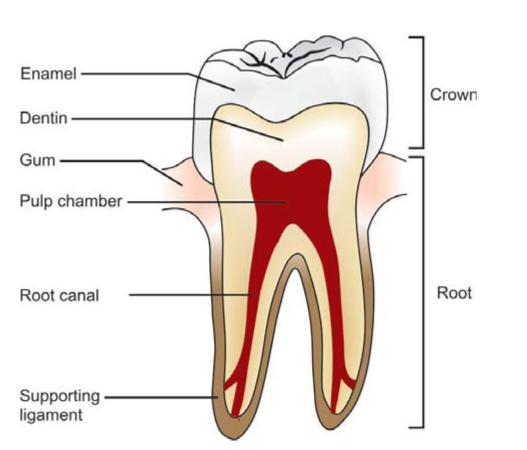
Fig. 3.1: Diagrammatic representation of enamel, dentin, pulp and supporting structures
ENAMEL
Tooth enamel is the hardest and most highly mineralized substance of the body which covers the crown of the tooth. It is the normally visible dental tissue of a tooth which is mainly responsible for color, esthetics, texture and translucency of the tooth. One of the main goal in operative dentistry is preservation of enamel. So today’s dentistry mainly revolves around simulating natural enamel in its color, esthetics, contours and translucency by replacing with synthetic restorative materials.
Although enamel can serve lifelong, but it is more susceptible to caries, attrition (physical forces) and fracture due to its structural make up, i.e. mineralized crystalline structure and rigidity. One of the interesting features of enamel is that it cannot repair itself. So, loss in enamel surface can be compensated only by restorative treatment.
Composition
It is highly mineralized structure which mainly contains inorganic contents in the form of crystalline structure. Main inorganic content in the enamel is hydroxyapatite. In addition to inorganic content, it also contains a small portion of organic matrix along with small amount of water which is present in intercrystalline spaces.
Composition
1. Inorganic content (by vol.)
a. Hydroxyapatite-90-92%
b. Other minerals and trace elements-3-5%
Organic content (by vol.)
1. Proteins and lipids-1-2%
2. Water-4%
Structure
Enamel is mainly composed of millions of enamel rods or prisms as well as sheaths and a cementing inter rod substance. Each rod has a head and tail. The head is directed occlusally and the tail is directed cervically. The rod is formed of number of hydroxyapatite crystals which vary in size, shape and number. Each rod formed of about 300 unit crystal length and 40 units wide and 20 unit thick in threedimensional hexagon. In transverse sections, enamel rods appear as hexagonal and occasionally round or oval. Rods may also resemble fish scales.
The diameter of rods increases from dentinoenamel junction towards the outer surface of enamel in a ratio of 1:2.
The rods or the prisms run in an alternating coarse of clockwise and anticlockwise direction (twisting course). Initially there is wavy coarse in one-third of enamel thickness adjacent to DEJ, then the coarse becomes more straight in the remaining thickness.
Enamel rods are arranged in such planes so as to resist the maximum masticatory forces. Rods are oriented at perpendicular to the dentinoenamel junction. Towards the incisal edge these become increasingly oblique and are almost vertical at the cusp tips. In the cervical region, there is difference in the direction of the enamel rods of deciduous and permanent teeth (Fig. 3.2). The cervical enamel rods of deciduous teeth are inclined incisally or occlusally, while in permanent teeth they are inclined apically. This change in direction of enamel rods should be kept in mind during tooth preparation so as to avoid unsupported enamel rods.
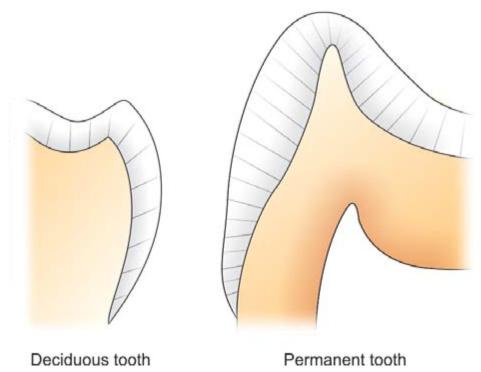
Fig. 3.2: Diagram showing direction of enamel rods in deciduous and permanent teeth
Structure
• Composed of millions of rods or prisms
• Diameter of enamel rod increases from dentinoenamel junction towards outer surface of enamel in 1:2
• Enamel rods lie perpendicular to dentinoenamel junction
• In cervical region, direction of enamel rod is incisally/ occlusally in deciduous while in permanent, it is apically.
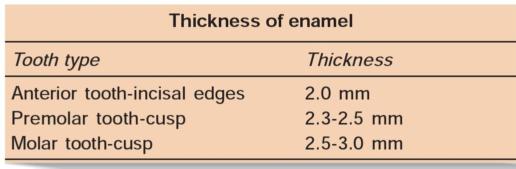
Thickness
The thickness of enamel varies in different areas of the same tooth and from one type of tooth to another type of tooth. The average thickness of enamel at the incisal edges of incisors is 2 mm; at the cusp of premolar and molar from 2.3 to 3.0 mm. Thickness of enamel decreases gradually from cusps or incisal edges to cementoenamel junction.
Color
The color of enamel is usually gray and translucent in nature. Color of tooth mainly depends upon three factors: (a) color of underlying dentin, (b) thickness of enamel, (c) amount of stains in enamel. The translucency of enamel is directly related to degree of mineralization and homogenicity. Anomalies occurring during developmental and mineralization stage, antibiotic usage and excess fluoride intake affect the color of tooth.
Color of enamel is affected by
• Color of underlying dentin
• Thickness of enamel
• Amount of stains in enamel
• Anomalies occurring during developmental and mineralization stage like antibiotic usage and excess fluoride intake affects the color.
Strength
Enamel has a rigid structure. It is brittle, has a high modulus of elasticity and low tensile strength. The specific gravity of enamel is 2.8. Hardness of enamel is different in different areas of the external surface of a tooth. The hardness also decreases from outer surface of the enamel to its inner surface. Also the density of enamel increases from dentinoenamel junction to the outer surface. When compared, dentin has high compressive strength than the enamel, this acts as a cushion for enamel when masticatory forces are applied on it. For this reason during tooth preparation, for maximal strength of underlying remaining tooth structure all enamel rods should be supported by healthy dentin base.
Structure present in enamel
1. Gnarled enamel
2. Bands of Hunter-Schreger
3. Enamel tufts
4. Enamel lamellae
5. Enamel spindles
6. Striae of Retzius
7. Prismless layer
8. Dentinoenamel junction
9. Occlusal pits and fissures.
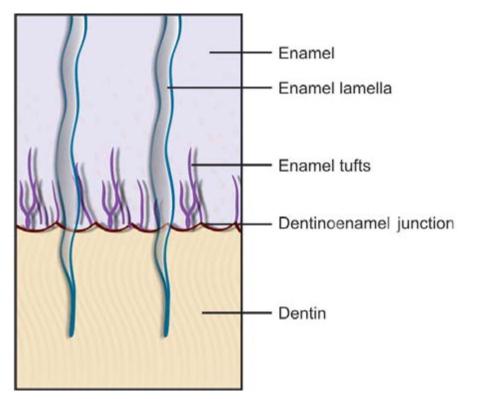
Structure Present in Enamel (Fig. 3.3)
Fig. 3.3: Diagram showing different structures present in enamel
Gnarled Enamel
There are group of irregular enamel that is more resistant to cleavage called Gnarled enamel present mostly in cervical, incisal and occlusal portion. This consists of bundles of enamel rods which interwine in an irregular manner with other group of rods, finally taking a twisted and irregular path towards the tooth surface.
Significance: This part of enamel is resistant to cutting while tooth preparation.
Bands of Hunter-Schreger
Hunter-Schreger bands usually occur because of alteration of light reflection (optical phenomenon) due to changes in rod direction. This results in alternating light and dark zones under the microscope. It is best seen in longitudinal ground sections seen under reflected light. They are mainly found in the inner surface of tooth. H-S bands are composed of different contents of organic material and varied permeability.
Significance: They are considered to resist and disperse the strong forces.
Enamel Tufts
Enamel tufts are ribbon-like structures which run from dentin to enamel. They are named so because they resemble tufts of grass. They contain greater concentration of enamel proteins.
Significance: Hypomineralized structure in the enamel, thus it plays role in spread of dental infection.
Enamel Lamellae
These are leaf like defects present in enamel and may extend to DEJ. They contains organic substances. Lamellae are commonly found at the base of occlusal pits and fissures. Bodecker in 1906 was the first to describe these developmental defects of enamel which he named “lamellae”.
These are caused by “imperfect calcification of enamel tissue”.
Pincus suggested that if developing cusps fail to coalesce when forming a fissure, a gap in the enamel occurs. Such a gap may vary in size from a crack or lamella.
Three types of lamellae are commonly seen:
• Type A composed of “poorly calcified rod segments”
• Type B composed of degenerated cells
• Type C arising after eruption where the crack is filled with mucoproteins from the oral preparation.
Type A lamellae is confined to enamel while types B and C may extend into dentin.
Various studies have shown that lamellae might be the site of entry of caries.
Ten Cate stated that tufts and lamellae are of no significance and do not appear to be sites of increased vulnerability to caries attack.
A lamella at the base of an occlusal fissure provides an appropriate pathway for bacteria and initiate caries.
Enamel Spindles
Odontoblastic processes sometimes crosses DEJ and their end is thickened. Spindles serve as pain receptors, that is why, when we cut in the enamel patient complains of pain.
Striae of Retzius
They appear as brownish bands in the ground sections and illustrate the incremental pattern of enamel. These represent the rest periods of ameloblast during enamel formation, therefore also called as growth circles. When these circles are incomplete at the enamel surface, it results in alternating grooves called imbrications lines of pickerills, the elevations in between called perikymata. Perikymata are shallow furrows where the striae of Retzius end. These are continuous around the tooth and parallel the CEJ.
Striae of Retzius are stripes that appear on enamel when viewed microscopically in cross-section. Formed from changes in diameter of “Tomes” processes, these stripes demonstrate the growth of enamel, similar to the annual rings on a tree.
Prismless Layer
There is structureless layer of enamel near the cervical line and to a lesser extent on the cusp tip which is more mineralized.
Dentinoenamel Junction
Dentinoenamel junction is pitted/scalloped in which crests are toward enamel and shallow depressions are in dentin. This helps in better interlocking between enamel and dentin. This is a hypermineralized zone and is about 30 microns thick.
Significance: Shape and nature of the dentinoenamel junction prevents tearing of enamel during functions.
Occlusal Pits and Fissures
Pits and fissures are formed by faulty coalescence of developmental lobes of premolars and molars (Fig. 3.4). These are commonly seen on occlusal surfaces of premolars and molars. These are formed at the junction of the developmental lobes of the enamel organs. Grooves are developed by smooth coalescence of developmental lobes.

Fig. 3.4: Showing pits and fissures of premolars and molars
Significance:
• Thickness of enamel at the base of pit and fissure is less.
• Pits and fissures are the areas of food and bacteria impaction which make them caries prone (Fig. 3.5).

Fig. 3.5: Deep pits and fissures making areas favorable for food impaction
• V-shaped grooves provide escapement of food when cusps of teeth of opposite arch occlude during mastication.
Functions of Enamel
1. It is hardest structure of tooth which supports masticatory forces.
2. It is mainly responsible for color, esthetics, surface texture and translucency of the tooth.
3. It also supports the underlying dentin and pulp.
Functions of enamel
• Hardest structure of tooth supporting the masticatory forces
• Responsible for color and esthetics
• Responsible for surface texture and translucency of tooth
• Support underlying dentin and pulp
Clinical Significance of Enamel
• Color: Color of the enamel varies because of following factors:
– Age
– Ingestion of tetracycline during the formative stages
– Ingestion of fluoride
– Extrinsic stains
– Developmental defects of tooth.
• Attrition: The change usually seen in enamel with age due to wear of occlusal surfaces and proximal contact points during mastication. Sometimes bruxism or contacts with porcelain also lead to attrition (Fig. 3.6). So, in these patients, try to avoid placing the margins of restoration in occlusal contact area or place a restorative material that wears at a same rate as enamel.

Fig. 3.6: Attrition of teeth
• Acid etching: Acid etching is used in fissure sealants and bonding of restorative material to enamel. Acid etching has been considered as accepted procedure for improving the bonding between resin and enamel. Acid etching causes preferential dissolution of enamel surface and helps in increasing the bonding between resin and enamel.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


