Aphthae (recurrent aphthous stomatitis)
 Aphthae are multiple recurrent small, round or ovoid ulcers which have circumscribed margins, erythematous haloes, and yellow or grey floors, appearing first in childhood or adolescence
Aphthae are multiple recurrent small, round or ovoid ulcers which have circumscribed margins, erythematous haloes, and yellow or grey floors, appearing first in childhood or adolescence
 A minor degree of immunological dysregulation underlies aphthae
A minor degree of immunological dysregulation underlies aphthae
 A family history of aphthae is common
A family history of aphthae is common
 Most patients appear otherwise well and predisposing factors are unclear
Most patients appear otherwise well and predisposing factors are unclear
 Ulcers similar to aphthae (aphthous-like ulcers) may be seen in some immune disorders
Ulcers similar to aphthae (aphthous-like ulcers) may be seen in some immune disorders

INTRODUCTION
 With multiple recurrent, round or ovoid ulcers known as aphthae or canker sores, which have circumscribed margins, erythematous haloes, and yellow or grey floors (Fig. 34.1):
With multiple recurrent, round or ovoid ulcers known as aphthae or canker sores, which have circumscribed margins, erythematous haloes, and yellow or grey floors (Fig. 34.1):
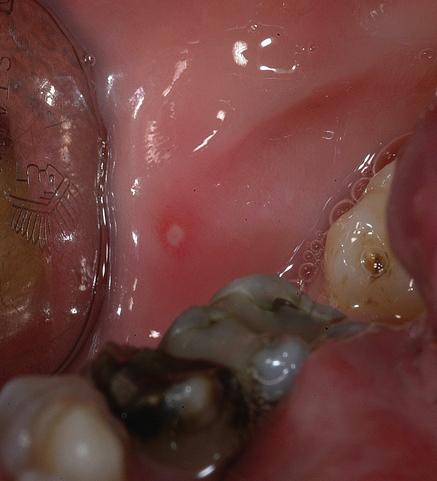



It is important to note that individual aphthae last only a limited period of time, before they heal spontaneously. This is quite a different history from ulcers that persist without healing, such as malignant ulcers and those associated with vesiculobullous disorders such as pemphigoid and pemphigus.
PREDISPOSING FACTORS
 Stress underlies RAS in some cases and ulcers appear to exacerbate during school or university examination times.
Stress underlies RAS in some cases and ulcers appear to exacerbate during school or university examination times.
 Trauma from biting the mucosa or from dental appliances may lead to aphthae in some people.
Trauma from biting the mucosa or from dental appliances may lead to aphthae in some people.
 Cessation of smoking may precipitate or exacerbate RAS in some cases, but the reason is unclear.
Cessation of smoking may precipitate or exacerbate RAS in some cases, but the reason is unclear.


 Allergies to food occasionally underlie RAS, and there is a high incidence of atopy.
Allergies to food occasionally underlie RAS, and there is a high incidence of atopy.








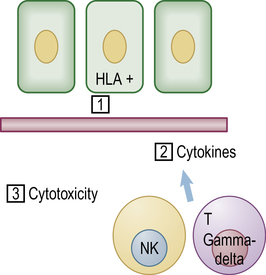
AETIOLOGY AND PATHOGENESIS
Immune mechanisms that appear to play a role in a people with a genetic predisposition to oral ulceration include the following (Fig. 34.2):










CLINICAL FEATURES
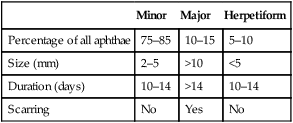
There are three main clinical types of RAS (Table 34.1), though any significance of these distinctions is unclear (they could be three distinct disorders):
Table 34.1
Clinical characteristics of the different clinical types of aphthae
| Minor | Major | Herpetiform | |
| Percentage of all aphthae | 75–85 | 10–15 | 5–10 |
| Size (mm) | 2–5 | >10 | <5 |
| Duration (days) | 10–14 | >14 | 10–14 |
| Scarring | No | Yes | No |



MINOR APHTHOUS ULCERS (MiAU; MIKULICZ ULCER)
 occurs mainly in the 10–40 year age group
occurs mainly in the 10–40 year age group

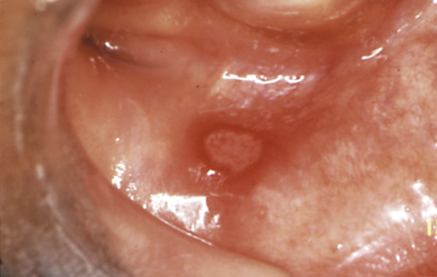
 consists of small round or ovoid ulcers 2–4 mm in diameter (Fig. 34.3), in groups of only a few ulcers (1–6) at a time, with initially yellowish floors surrounded by an erythematous halo and some oedema, but the floors assume a greyish hue as healing and epithelialization proceeds
consists of small round or ovoid ulcers 2–4 mm in diameter (Fig. 34.3), in groups of only a few ulcers (1–6) at a time, with initially yellowish floors surrounded by an erythematous halo and some oedema, but the floors assume a greyish hue as healing and epithelialization proceeds




MAJOR APHTHOUS ULCERS (MjAU)
This type of RAS, also known as Sutton’s ulcers or periadenitis mucosa necrotica recurrens (PMNR):









Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


