Digital Alternatives in the Implant Restoration of the Edentulous Patient
Mathew T. Kattadiyil
Loma Linda University School of Dentistry, Loma Linda, California, USA
Introduction
There are multiple digital applications that are available for the implant restoration of an edentulous patient. However, they are relatively new, as most applications continue to improve with time and innovative ideas. Some of these applications include digital impressions, computer‐aided designing and computer‐aided manufacturing (CAD/CAM) of metallic or zirconia‐based bar/substructures, and even fabrication of implant‐assisted dentures. There is consensus amongst clinicians that a successful implant restoration is planned keeping the final prosthesis in mind. This allows ideal planning and placement of implants. This could not be truer when planning and fabricating an implant‐assisted prosthesis for the completely edentulous arch. An appropriately fabricated complete denture serves as an ideal template for this planning.
The history of complete denture fabrication started in the US approximately 250 years ago with dentures being carved from ivory.1 The wooden dentures worn by President George Washington and his concerns with them have become part of US history. Since those early days, concepts, techniques, and materials involved in the fabrication of complete dentures have evolved and improved over time. An aging population2 promotes a demand for complete dentures that sustains continued interest in innovations in complete denture fabrications. This has been evidenced by the re‐emergence of interest in innovative techniques using digital and computer‐aided engineering of complete dentures. There are multiple options available to the clinician in the rehabilitation of the completely edentulous patient (Figure 20.1). These include prostheses made utilizing digital technology at some stage of fabrication. Figure 20.2 shows the steps involved in the fabrication of a fixed complete denture and steps identifying areas where conventional or digital technology can be applied in the process of fabrication.
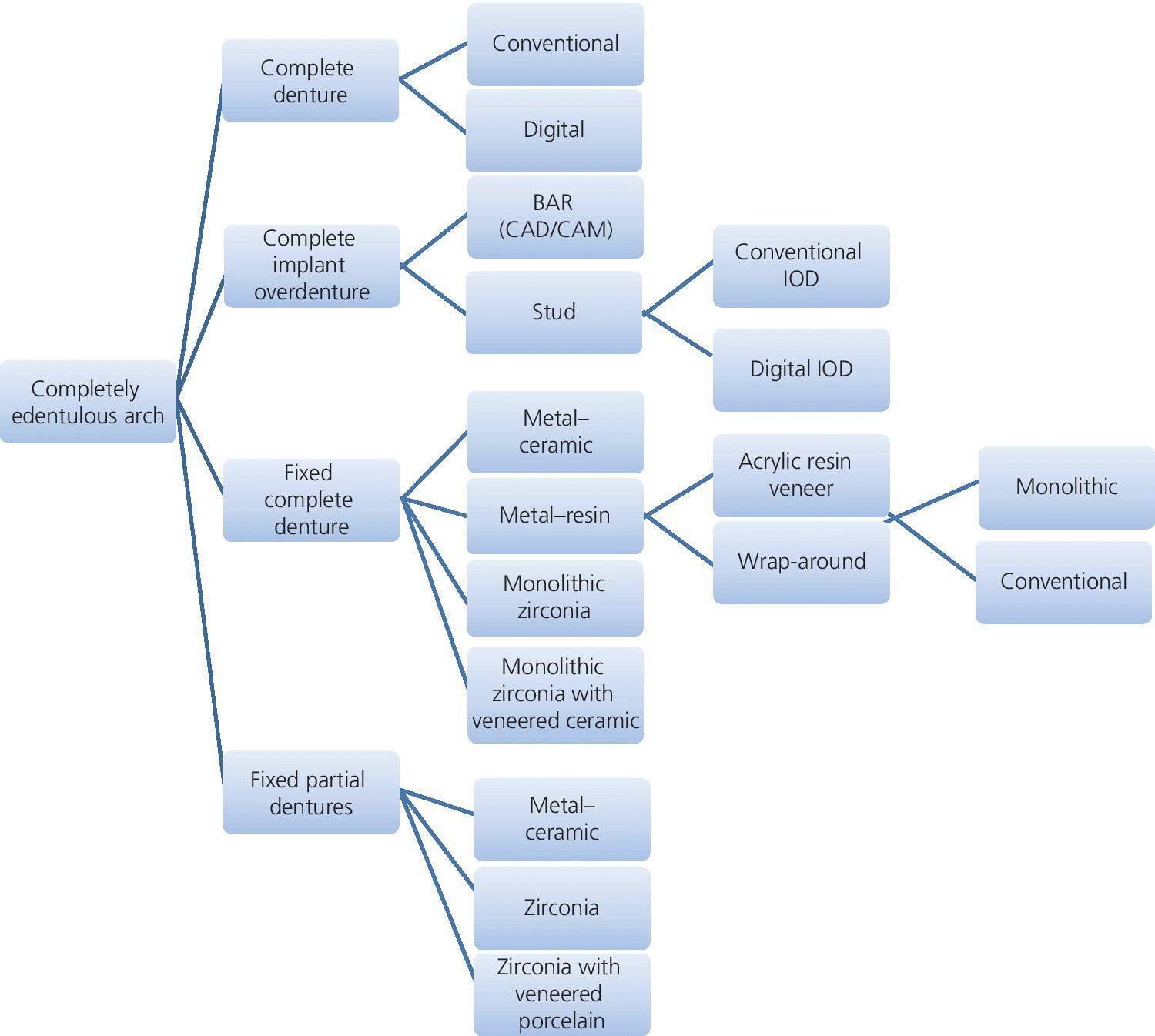
Figure 20.1 Schematic diagram showing the options available in the restoration of the completely edentulous arches.
Source: reproduced with permission from Erin Burke, CA.
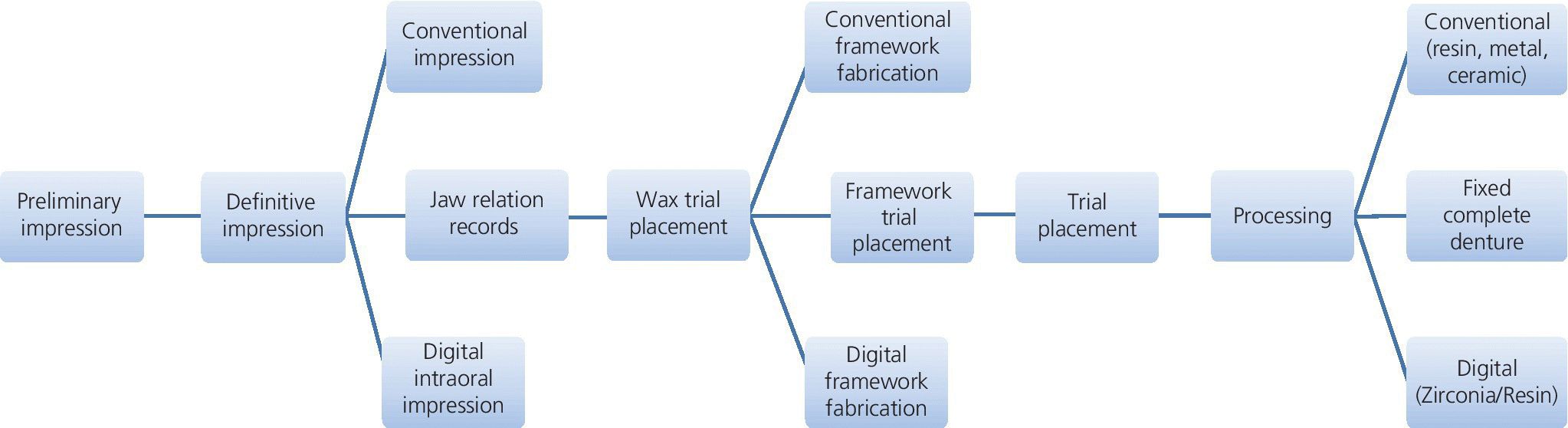
Figure 20.2 Schematic diagram showing the steps involved in the fabrication of a fixed complete denture with areas where digital applications can be an option.
Source: reproduced with permission from Erin Burke, CA.
While digital applications are fairly well entrenched in fixed prosthodontics, it was only recently that published reports on computer‐aided engineering emerged, leading, in a sense, to the awakening of digital applications in removable prosthodontics.
Maeda et al.3 in 1994 initially reported the concept of developing computer‐aided technology for designing and fabricating complete dentures. In this article, the authors described a rapid prototyping technique to fabricate a complete denture by photopolymerizing a composite resin material. They also predicted the application of a numerical controlled milling process as a potential technique in the digital fabrication of dentures. A few years later, Kawahata et al.4 reported the potential of computer numeric controlled (CNC) milling in the fabrication and duplication of dentures.
Goodacre et al.5 described the development of CAD/CAM technology producing initially a crude “proof‐of‐concept” denture base milled from leucite with a three‐axis milling machine. Denture bases were subsequently milled from prepolymerized poly (methyl methacrylate), a material more commonly used in the fabrication of complete dentures than leucite.5
Kattadiyil et al.6 provided a report on the application of the two currently available digital denture systems; the AvaDent Digital Denture (Global Dental Science, LLC (GDS)) and the Dentca™ CAD/CAM denture (Dentca Inc). They reviewed the fabrication protocol involved with both systems. One of the primary advantages of both digital systems is the reduced clinical appointments to two from the traditional five‐appointment process associated with the conventional method of fabrication. Other anticipated advantages of the use of CAD/CAM technology in the fabrication of digital complete dentures over conventionally fabricated dentures are reduction in actual treatment time, reduction in fees, lack of polymerization shrinkage, potential for convenient fabrication of replacement dentures from the repository of digital data acquired for fabrication of the first set of dentures, and less patient adaptation time for the replacement dentures due to consistency in morphology with the previous dentures.
A systematic review on the fabrication of complete dentures with computer‐aided technology (CAT) by Bidra et al.7 predicted that the application of CAT in the fabrication of complete removable dental prostheses (CRDP) could significantly impact patient care, dental education, public health, and dental research.
Infante et al.8 reported in detail the technique employed to fabricate milled complete dental prostheses with the utilization of digital scanning technology. They described the method of fabrication involved with one of the more commonly used digital CRDP systems (AvaDent, GDS).
The introduction of implants to improve retention and stability for complete dentures has had a significant impact on the quality of life of the edentulous patient.9,10 The McGill consensus report,11 published in 2002, stated that the two‐implant mandibular implant overdenture be considered for every completely edentulous patient stating “there is now overwhelming evidence that a two‐implant overdenture should become minimally the first choice of treatment for the edentulous mandible.” In 2009, the York consensus statement made the same point as the McGill report, saying that “a substantial body of evidence is now available demonstrating that patients’ satisfaction and quality of life with implant supported overdentures is significantly greater than for conventional dentures.”12
This chapter outlines the innovative application of digital technology in the rehabilitation of the edentulous patients with implant‐assisted prostheses.
Applications of digital complete dentures with implants
The increasing interest in digital denture fabrication expanded to the exploration of the application of this technology in the rehabilitation of completely edentulous patients with implant‐assisted prostheses. Although this should only be considered an early stage in this application, there have been some interesting case reports that show promise in expanding the utilization of the new technology.
Bidra et al.13 described the application of this technology where a two‐appointment digital denture process was used to fabricate a complete denture which was subsequently converted to an implant overdenture by picking up the attachments intraorally at the placement appointment. Lozada et al.14 and Kattadiyil et al.15 reported some unique utilization of the digital denture technology to improve efficiency in both the surgical and prosthodontic phases of treatment of the completely edentulous patient. In a two‐part series they described in detail the utilization of CAD/CAM technology in the surgical and prosthodontic phases of treatment.
In part 1, for the surgical phase of treatment, Lozada et al.14 described the fabrication of provisional dentures which were fully milled (including both the denture base and teeth) using a proprietary technique. Subsequently, a milled radiographic template was also fabricated by the digital denture manufacturer that was a duplicate of the mandibular provisional denture to which fiduciary markers were attached. A cone‐beam computed tomography (CBCT) scan was made of only the radiographic template and then the radiographic template was positioned intraorally using an index and a CBCT scan made of the patient following the NobelGuide™/NobelClinician protocol.16 The surgical planning for implant placement was performed using NobelClinician software (Figure 20.3), based on the orientation of the denture bases and teeth to the existing bone and vital anatomical structures, so the most appropriate locations could be identified for each implant. Once the plan for implant positions was finalized, a NobelGuide™ surgical template was fabricated.
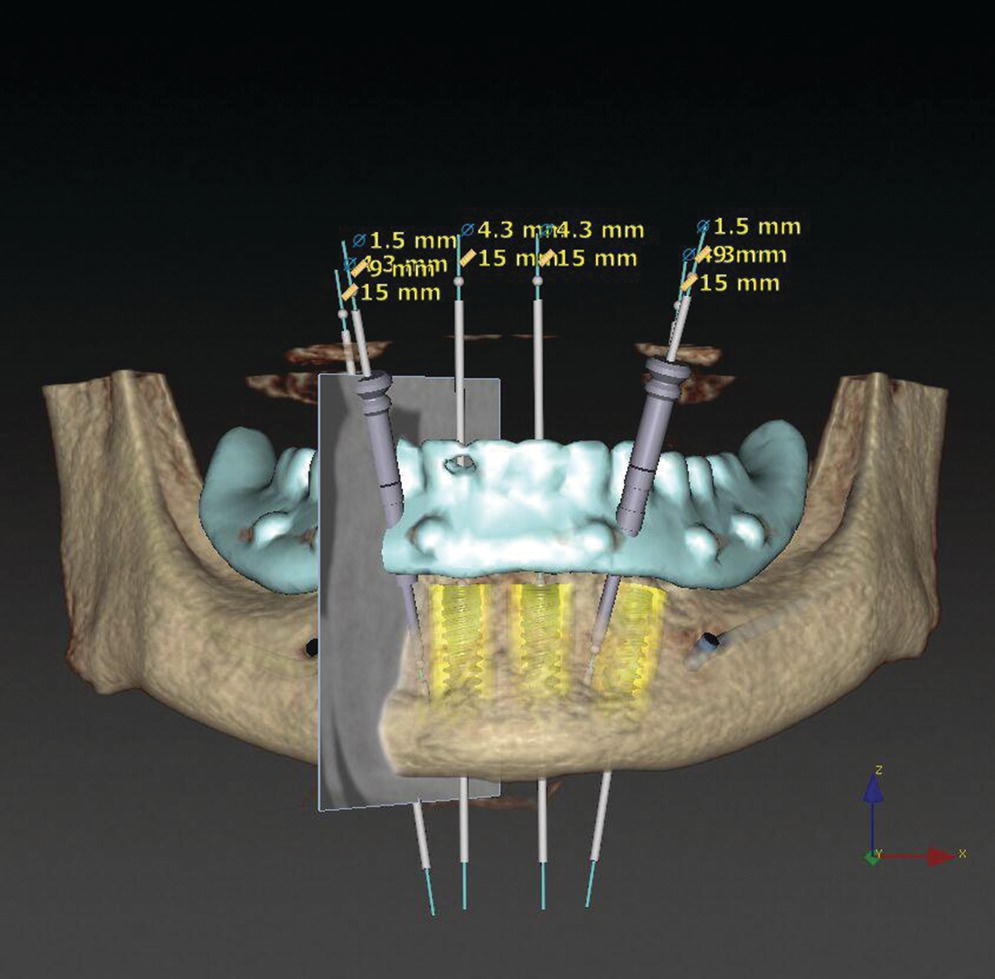
Figure 20.3 Planning for implant surgery accomplished with the Nobel Clinician protocol. The radiographic template is a milled, identical in morphology, replica of the digital provisional denture.
In a classic model where two companies collaborated together using individual strengths of their different software to achieve successful outcome, the virtual implant positions planned using the Nobel Clinician software were used by Global Dental Science to fabricate an AvaDentTM mandibular conversion complete denture (Figure 20.4). This conversion denture had channels milled through the denture base at the appropriate positions where temporary copings would be located after their attachment to the implant abutments. It also had a pre‐milled slot located around the denture base with a small number of struts that connected the peripheral denture base to the central portion of the conversion denture that functioned as the immediate provisional fixed complete denture (CD). The presence of the channels and slot facilitated easy conversion of the denture to a fixed prosthesis, while using the positional stability of the peripheral denture base to accurately orient the prosthesis in the patient’s mouth during attachment of the denture to the temporary copings. The AvaDent™ Conversion Denture was connected to temporary copings using autopolymerizing acrylic resin (Figure 20.5). Once the resin had polymerized, the struts were sectioned to efficiently convert the denture to an immediate fixed CD (Figures 20.5, 20.6 and 20.7). This method reduces the time involved in forming the conversion prosthesis during the surgery.
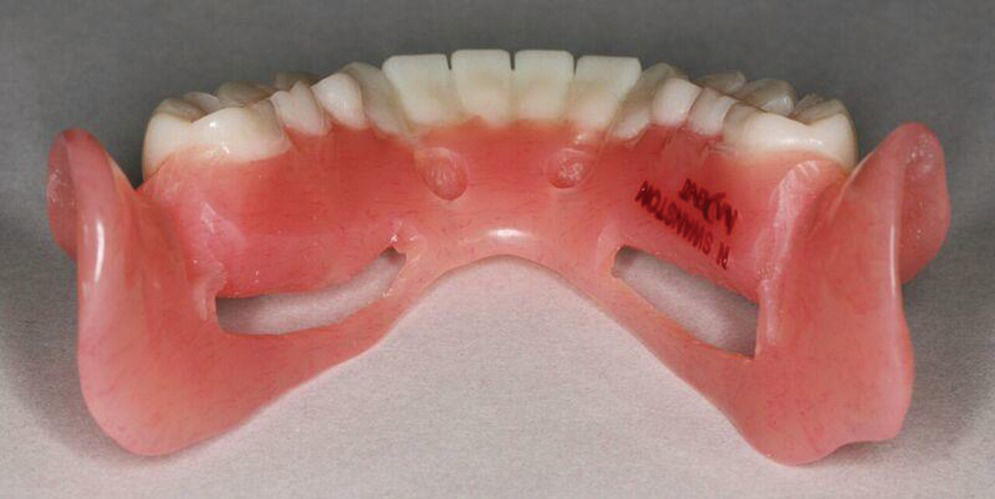
Figure 20.4 Milled conversion denture with slots and recesses to allow easy placement, connection to temporary copings for conversion to a provisional fixed complete denture.
Source: reproduced with permission from Ankur Dahiya, Austin, TX.
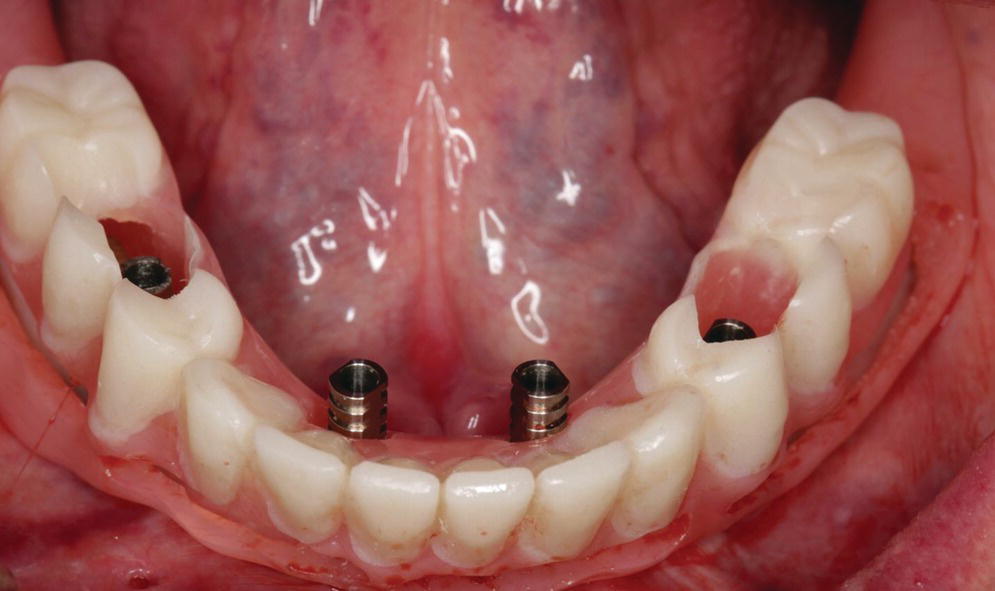
Figure 20.5 Mandibular conversion denture placed easily to seat on to the soft tissues. Access holes had been already fabricated utilizing information from the digital planning for the surgery. Temporary copings had already been placed on the implants and are ready to be attached to the conversion denture. Note the peripheral struts for easy separation.

Figure 20.6 Intaglio surface of mandibular conversion denture.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


