Introduction
The purpose of this study was to use lateral cephalometry and computed tomography (CT) to examine the volumetric, planar, and linear changes in the pharyngeal airway after mandibular setback surgery.
Methods
The pharyngeal airways of 12 subjects who underwent mandibular setback surgery at Seoul National University Dental Hospital were assessed linearly and volumetrically on lateral cephalometric radiographs and CT before surgery and 6 months after surgery. The pharynx, nasopharynx, and oropharynx were evaluated by volumetric analysis. Pharyngeal depth, airway space, pharyngeal soft-tissue thickness, and hyoid bone position were measured by linear analysis. The axial section area of the airway was measured by area analysis.
Results
From the linear analysis, a significant decrease in pharyngeal depth and a significant posterior movement of the hyoid bone ( P <0.05) were noted. Volumetric analysis by CT showed that the oropharynx decreased after mandibular setback surgery. However, the volume and the axial section area of the airway in the CT images did not change significantly after mandibular setback surgery ( P >0.05).
Conclusions
Although the structures around the mandible inevitably moved backward after mandibular setback surgery on linear analysis, physiologic deformation could occur to preserve the airway capacity after sagittal compression.
The relationship between respiration and craniofacial morphology—airway anatomy, nasal flow, and orthognathic surgery—has been the subject of many studies. Mandibular setback surgery can reduce the volume of the pharyngeal airway because of the positional changes of the tongue. Pharyngeal airway constriction after surgery might lead to sleep apnea syndrome. The results from a 12-year postoperative observation suggested continuous narrowing of the airway.
Therefore, the positional changes in the tongue after mandibular setback surgery might cause postural adaptation of the tongue to preserve the airway, which can influence surgical stability. Another study reported that the hyoid bone finally returned to its original position after an immediate backward, downward movement by surgery, and the position of the hyoid bone might be related to the stability of the surgical results.
On the other hand, Takagi et al reported that the size of the oropharyngeal airway did not change after mandibular setback surgery, even though there was downward movement of the hyoid bone. They suggested that physiologic mechanisms to maintain the pharyngeal airway can occur after the posterior location of the tongue through surgery. A long-term study on the changes in the airway after the mandibular setback surgery showed a gradual physiologic readaptation of the pharyngeal airway morphology to its original dimensions, even though the lower facial morphology and pharyngeal airway morphology had changed after surgery.
Because most evaluations of the pharyngeal airway were carried out with cephalometric radiographs, there were some limitations, such as the lack of soft-tissue detail and the difficulty of 3-dimensional (3D) analysis. Computerized tomography (CT) can provide accurate anatomic information of the soft and hard tissues. Montgomery et al reported that the nasopharynx volume could be calculated by CT rather than with a silicone rubber cast. CT can allow an accurate in-vivo assessment of the 3D relationship of the facial structures.
In this study, we evaluated the volumetric, planar, and linear changes in the pharyngeal airway after mandibular setback surgery on CT and lateral cephalometry, and compared the results from the volumetric and linear data.
Material and methods
Twelve patients (5 men, 7 women; mean age, 25.5 years) who underwent mandibular setback surgery at Seoul National University Dental Hospital in Korea were enrolled in this study. All subjects had a bilateral sagittal split ramus osteotomy for the correction of mandibular prognathism by 1 surgeon (M.J.K.). The facial CT scan and lateral cephalometric radiograph of each subject in the supine position were taken preoperatively within 1 month (T0) and postoperatively about 6 months (T1). The CT scans were made by using a Somatom Plus 4 (Siemens, Erlangen, Germany) with 1.5-mm section intervals, 1.0-mm slice thickness, and 512 × 512 matrix. The head and neck were supported and fixed with a hard pillow while taking the CT. The resulting 2-dimensional image data were stored in Digital Imaging and Communications in Medicine (DICOM) format. Each subject was scanned from the cranial vault to the chin. Lateral cephalometric radiographs were taken (CX90SP, Ashahi, Tokyo, Japan). The data were analyzed with V-Works software (version 4.0, CyberMed, Seoul, Korea) for CT ( Fig 1 ) and V-Ceph software (version 4.5, CyberMed) for cephalometry.

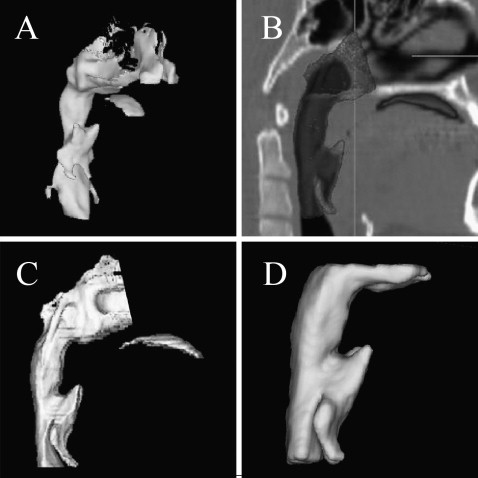
The pharynx is located behind the nasal and oral cavities and the larynx, extending from the cranial base to the level of the sixth cervical vertebra and the lower border of the cricoid cartilage. It can be divided into 3 parts: nasopharynx, oropharynx, and laryngopharynx. The nasopharynx is located behind the nasal cavity and above the soft palate. Anteriorly, it is connected to the nasal cavity. Posteriorly, it continues downward to the oropharynx. The oropharynx is the opening into the oral cavity by an isthmus and extends from the second to the fourth cervical vertebrae. The laryngopharynx joins the oropharynx at the level of the pharyngoepiglottic fold and hyoid, and then continues to the level of the sixth cervical vertebra. For volumetric analysis, the pharynx, nasopharynx, and oropharynx were defined as follows. For the volumetric analysis of the airway on CT, the volume of the pharynx, which consisted of the nasopharynx and the oropharynx, was assessed. The landmarks and planes were defined as the Frankfort horizontal (FH) plane, the most posterior point of the pterygomaxillary fissure (PT point), posterior nasal spine (PNS), and the third cervical vertebra (C3) ( Fig 2 ). The nasopharyx was defined as the airway space between a plane parallel to FH passing through PNS and a plane passing through the right and left PT points, and the PNS. The oropharynx was defined as the airway space between a plane parallel to FH passing through PNS and a plane parallel to FH passing through C3. The pharynx was defined as the sum of the nasopharynx and theoropharynx. V-works software was used to reconstruct the airway space from the CT slice images. The airway volume in the area of interest was calculated from the number of voxels ranging from the minimum value (–1024 HU) to –600 HU to exclude the soft and hard tissues ( Fig 3 , A ). The airway selected by the threshold value was divided into the planes used to the define the airway spaces ( Fig 3 , B and C ). The volume of each part was measured by exporting the divided spaces for volumetric analysis to the surface on demand model ( Fig 3 , D ).
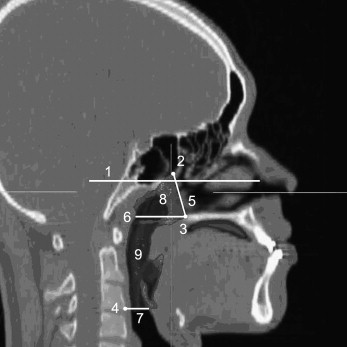
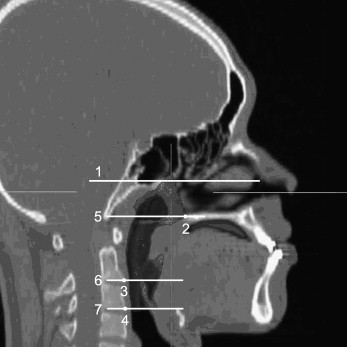
Linear analysis of the pharyngeal airway morphology on the lateral cephalometric radiographs was based on the method of Pae et al and Saitoh. The landmarks and reference planes for linear analysis are shown in Figure 4 , A .
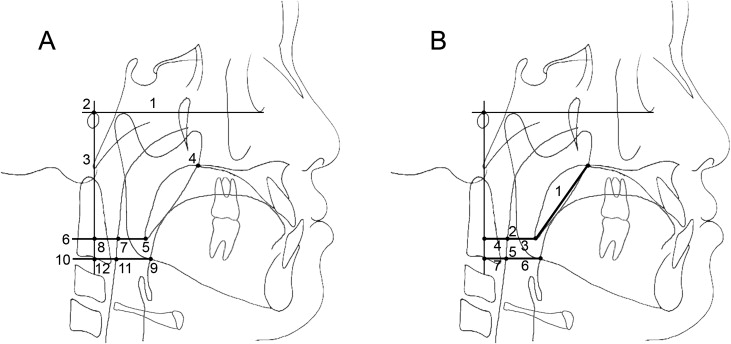
The following 7 measurements were defined for linear analysis on the cephalometric radiograph: soft palate length, middle pharyngeal depth, middle airway space, middle soft-tissue thickness, inferior pharyngeal depth, inferior airway space, and inferior soft-tissue thickness ( Fig 4 , B ).
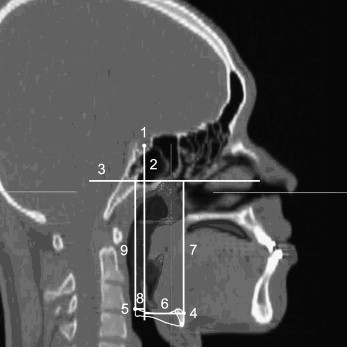
The position of the hyoid bone was analyzed by CT to determine the effects of mandibular setback surgery. The landmarks, planes, and measurements for the linear analysis of the hyoid bone on CT are shown in Figure 5 .
The axial section area of the airway was analyzed by CT to evaluate the changes. For area analysis of the axial section on CT, the landmarks and planes are shown in Figure 6 . The measurements were defined as the area on the PNS (area of the airway on the PNS plane), area on C2 (area of the airway on the C2 plane), and area on C3 (area of the airway on the C3 plane).
Statistical analysis
The airway volume was calculated twice 3 weeks apart to evaluate the reliability of the measuring method. The surgical changes in the pharyngeal airway and hyoid bone position were evaluated by comparing the volumetric and linear measurements and the axial section area of the airway at T0 and T1 by using a paired t test. P <0.05 was considered significant.
Results
The reliability of the method for measuring the airway volume was high, with an error variance from 0.22% to 1.04% of the total mean value ( Table I ). The errors in the estimation ranged from 78.15 to 157.40 mm 3 . The results of the volumetric analysis from the CT data showed no significant difference between the T0 and T1 images of the nasopharynx, oropharynx, and pharynx ( P >0.05; Table II ). The volume of the pharynx, including the nasopharynx and oropharynx, changed from 17.63 × 10 3 mm 3 at T0 to 16.09 × 10 3 mm 3 at T1. There was little change in the nasopharynx volume: 6.70 × 10 3 mm 3 and 6.69 × 10 3 mm 3 at T0 and T1, respectively. The oropharynx volume decreased from 10.92 × 10 3 mm 3 to 9.40 × 10 3 mm 3 . Linear analysis of the cephalometric radiographs showed decreases in all measurements after surgery except for soft-palate length ( Table III ). Some measurements decreased significantly from T0 to T1, such as middle pharyngeal depth ( P <0.01) and inferior pharyngeal depth ( P <0.05). Although the airway space (middle and inferior) and soft-tissue thickness (middle and inferior) were reduced, they showed no significant change ( P >0.05).
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


