Fixed Prostheses
FP-1
Definition.
An FP-1 is a fixed restoration and appears to the patient to replace only the anatomic crowns of the missing natural teeth (clinical crown). To fabricate this restoration type there must be minimal loss of hard and soft tissues. The volume and position of the residual bone must permit ideal placement of the implant in a location similar to the root of a natural tooth. The final restoration appears very similar in size and contour to the clinical crown or most traditional FPs used to restore or replace natural crowns on teeth (Figs. 3.2 and 3.3).


Implant Criteria.
The FP-1 prosthesis is most often desired in the maxillary anterior region, especially in the esthetic zone during smiling. The final FP-1 restoration appears to the patient to be similar to a crown on a natural tooth. However, the implant abutment can rarely be treated exactly as a natural tooth prepared for a full crown. The cervical diameter of a natural tooth is approximately 6.5 to 10.5 mm with an oval-triangular cross-section. However, the implant abutment is usually 4 to 5 mm in diameter and round in cross section. In addition, the placement of the implant rarely corresponds exactly to the crown–root position of the original tooth. For example, the thin labial bone lying over the facial aspect of a maxillary anterior root remodels after tooth loss, and the crest width shifts to the palate, decreasing 40% within the first 2 years.
Complication.
The most common complication with a patient requesting a FP-1 prosthesis is not recognizing preoperatively the limitations of the hard and soft tissue anatomy. If the final implant position is nonideal, it will be almost impossible to obtain a FP-1 prostheses without hard and soft tissue grafting.
Prevention.
The bone loss and lack of interdental soft tissue complicate the final esthetic result, especially in the cervical region of the crowns. FP-1 prostheses are especially difficult to achieve when more than two adjacent teeth are missing because of the need for hard tissue augmentation, soft tissue augmentation, and optimal implant positioning.
Hard tissue augmentation.
The width or height of the crestal bone is frequently insufficient after the loss of multiple adjacent natural teeth, and bone augmentation is often required before implant placement to achieve natural-looking crowns in the cervical region.
Soft tissue augmentation.
Because there are no interdental papillae in edentulous ridges, soft tissue augmentation is often required to improve the interproximal gingival contour. Ignoring this crucial step will result in open “black” triangular spaces (where papillae should usually be present) when the patient smiles.
Ideal implant positioning.
To obtain an FP-1 prostheses, the implant must be positioned ideally in the mesial-distal, buccal-lingual, and apicocoronal planes. The center of the osteotomy should be midway between the mesial-distal distance, provided the available space is ideal for the tooth being replaced. In a buccal-lingual position, the implant should be in a plane slightly lingual to the incisal edge of the tooth being replaced. In the apicocoronal plane, the implant should be approximately 3 mm apical to the free gingival margin of the adjacent teeth, provided that the adjacent teeth have ideal hard and soft tissue anatomy.
FP-2
Definition.
An FP-2 fixed prosthesis restores the anatomic crown and a portion of the root of the natural tooth and, therefore, is hypercontoured. The incisal edge of the restoration is in the correct position, but the gingival third of the crown is overextended, usually apical and lingual to the position of the original tooth. These restorations are similar to natural teeth exhibiting periodontal bone loss and gingival recession. In most situations an FP-2 is an acceptable prosthesis for patients. However, in the esthetic zone or in a patient with a high smile line, this may pose complication issues because the prosthesis may be deemed unesthetic by the patient (Fig. 3.4).

Implant Criteria.
The volume and topography of the available bone are more apical compared with the ideal bone position of a natural root (1–2 mm below the cement-enamel junction) and dictate a more apical implant placement compared with the FP-1 prosthesis. This most commonly occurs because of implant placement in Division B ridges, and because of the lack of bone width, the final implant position will be too far apical in comparison to the adjacent teeth.
Complication.
The most common complications that occur with a FP-2 prosthesis are a result of not informing the patient of the hypercontouring of the final prosthesis or the need for the use of pink porcelain. Especially in the maxillary anterior region, this may pose an esthetic issue with the patient. The use of pink porcelain also increases laboratory expenses.
Prevention
Patient communication.
The patient should be well informed prior to the initiation of treatment that the final FP-2 prosthesis will appear longer than healthy natural teeth (without bone loss). The patient should be shown photo images or diagrams of an FP-2 prosthesis compared to an FP-1 prosthesis prior to treatment. Additionally, the surgical informed consent should be modified to explain and fully inform the patient of the overcontoured prostheses (FP-1 vs. FP-2) (Fig. 3.5).

Preoperative smile zone evaluation.
The esthetic zone of a patient is established during smiling in the maxillary arch. The number of teeth displayed when a patient smiles is highly variable. Less than 10% of the population limits their smile to the anterior six teeth. Almost 50% of people show up to the first premolar and approximately 4% of our patients display almost all the maxillary teeth during a smile.3 The low lip position is ideally evaluated during sibilant sounds of speech (e.g., Mississippi, sixty-six). It is not unusual for patients to show fewer lower anterior teeth during smiling, especially in younger patients. Older patients are most likely to show the anterior teeth and gingiva during speech, with men showing more than women. Likewise, if the high lip line during smiling or the low lip line during speech does not display the cervical regions, the longer teeth are usually of no esthetic consequence, provided that the patient has been informed before treatment (Fig. 3.6).

Ideal implant position.
A multiple-unit FP-2 restoration does not require as specific an implant position in the mesial or distal position as does an FP-1 prosthesis. This is because the cervical contour is not displayed during function. The implant position may be chosen in relation to bone width, angulation, or hygienic considerations rather than purely esthetic demands (compared with the FP-1 prosthesis). On occasion, because of available bone, the implant may even be placed in an embrasure between the two teeth. This often occurs when replacing mandibular anterior teeth with a full-arch fixed restoration. If this occurs, the incisal two thirds of the two crowns should be ideal in width, as though the implants were not present. Only the cervical region is compromised (i.e., this is most likely out of the esthetic zone). Although the implant is not positioned in an ideal mesiodistal position, it should be placed in the correct facial-lingual position to ensure that contour, hygiene, and direction of forces are not compromised.
FP-3
Definition.
The FP-3 fixed restoration appears to replace the natural teeth crowns and has pink-colored restorative material (acrylic or pink porcelain) to replace a portion of the soft tissue, especially the interdental papillae. This is most commonly indicated when severe bone resorption has occurred.
Implant Criteria.
As with the FP-2 prosthesis, the original available bone height has decreased by natural resorption or osteoplasty at the time of implant placement. To place the incisal edge of the teeth in ideal position for esthetics, function, lip support, and speech, the excessive vertical dimension to be restored requires teeth that are unnatural in length. The soft and hard tissue loss requires replacement with pink porcelain or acrylic (Fig. 3.7).

Complication.
The main complication associated with an FP-3 prosthesis is patient acceptance because of the hypercontoured crowns (i.e., pink porcelain or acrylic). Additionally, the clinician must be aware of the added laboratory costs associated with an FP-3 prosthesis. Most laboratories will charge a significantly higher fee for the application of pink porcelain. However, the clinician should be aware there exist various shades of pink porcelain. It is recommended that the color of the tissue be evaluated similar to tooth shade. Many pink shade guides are available for use in implant dentistry today (Fig. 3.8).

Prevention
Patient communication.
The patient should be well informed prior to any treatment that the final FP-3 prosthetic teeth will appear longer and also have pink restorative material associated with the prosthesis to replace the loss of hard and soft tissue. Photos or examples of the pink prosthesis should be shown to the patient.
Understanding of smile zone variations.
The ideal high smile line (i.e., not showing excessive soft tissue) occurs in almost 70% of the population. The maxillary lip displays the interdental papilla of the maxillary anterior teeth, but not the soft tissue above the mid cervical regions. A high smile or “gummy” smile will usually display the interdental papillae and at least some of the gingival tissues above the free gingival margin of the teeth. Patients in both of these categories of high lip line should have the soft tissue replaced by either the prostheses or augmentation. Additionally, the appearance of the mandibular teeth may be evaluated during sibilant sounds (Fig. 3.9).

Color of the pink tissue.
Because the color characteristics of patient’s gingiva vary greatly, the implant clinician should use a laboratory that has the capability to use a pink porcelain shade guide to match the tissue. However, patients should be informed of the tissue color changes that occur over time.
Understand the two types of FP-3 prostheses.
There are basically two approaches for an FP-3 prosthesis. (1) A hybrid restoration of denture teeth and acrylic with a metal substructure. The complications associated with this type of prosthesis are excessive wearing of the denture tooth or debonding from the prosthesis. (2) A porcelain–metal/zirconia restoration. An FP-3 porcelain-to-metal/zirconia restoration is more difficult to fabricate for the laboratory technician than an FP-2 prosthesis. The pink porcelain is more difficult to appear as soft tissue and usually requires more porcelain firing cycles. This increases the risk of potential porosity or porcelain fracture (Fig. 3.10).

Spacing of multiple implants.
For edentulous arches or larger spaces, implants should be placed a minimum of 3 millimeters apart. If they are less than 3 millimeters apart, difficulty with hygiene will result along with the possibility that bone loss on one will extend to the other, compromising both implants.
Tissue space.
In the maxillary arch, wide open embrasures between the implants may cause food impaction or speech problems. These complications may be solved by using a removable soft tissue replacement mask or make the overcontoured cervical restorations. The maxillary FP-3 prosthesis is often extended or juxtaposed to the maxillary soft tissue so that speech is not impaired. However, this results in hygiene issues, which place the prostheses at risk. The mandibular FP-3 restorations may be left above the tissue, similar to a sanitary pontic. This facilitates oral hygiene in the mandible, especially when the implant is exposed through the soft tissue drape and is not visible during speech. However, if the space below the restoration is too great, the lower lip may lack support in the labio-mental region.
Removable Prostheses
When treatment planning, the patient’s prosthetic requirements should be fully understood and an evaluation of the patient’s anatomy is a priority. The most common removable implant prostheses are overdentures for completely edentulous patients. Complete removable overdentures have been reported with predictability and a high success rate for many decades; however, there is much confusion concerning this type of prosthesis because of the inherent variations.4,5 Most often, patients do not understand the associated movement with overdentures (i.e., dependent on number of implants, attachments, A-P spread, posterior ridge form) because they don’t understand the associated biomechanical factors with an overdenture prosthesis. The complications that may a occur may be significant.
There exist two types of removable prostheses that are based on support, retention, and stability of the restoration. Patients are able to remove the restoration but not the implant-supported superstructure or attachments to the abutments. The difference in the two categories of removable restorations are not in appearance (as it is in the fixed categories). Instead, the two removable categories are primarily determined by the amount of implant and soft tissue support (Fig. 3.11).

RP-4
Definition.
An RP-4 removable prosthesis is completely supported by implants with no soft tissue support. The RP-4 prosthesis is primarily a totally implant-supported prosthesis. The restoration is rigid when inserted, and the overdenture attachments usually connect the RP to single implant attachments or a low-profile tissue bar with attachments (Fig. 3.12).

Implant Criteria.
The implant placement criteria for an RP-4 prosthesis are different than that for an FP prosthesis. Denture teeth and acrylic require more prosthetic space for the removable restoration in comparison to a fixed prosthesis. The implants in an RP-4 prosthesis (and an FP-2 or FP-3 restoration) should be placed in the mesiodistal position for the best biomechanical and hygienic situation. Usually, in the mandible, implants are inserted between the two mental foramens in the A, B, C, D, and E positions.
Complication.
The most common complication occurring with a RP-4 prosthesis is lack of adequate implant support (e.g., insufficient number of implants) and food impaction. In the mandibular RP-4 prosthesis, because there exists no peripheral seal, often food becomes impacted underneath the prosthesis.
Prevention
Patient communication.
The patient should have a thorough understanding of the differences between a RP-4 and a RP-5 prosthesis. There exist distinct differences between RP-4 and RP-5 prosthesis with respect to number of implants, type of support, and prosthesis movement.
Treatment denture.
A preimplant treatment denture may be fabricated to evaluate the occlusal vertical dimension and ensure the patient’s esthetic satisfaction. This technique is especially indicated for patients with demanding needs and desires regarding the final esthetic result or with severely reduced vertical dimensions with their present prosthesis. The implant dentist may also use the treatment denture as a surgical guide for implant placement and for use during the healing stage. After the implants are uncovered, the superstructure or prosthetic design is fabricated within the guidelines of the existing treatment restoration.
Implant position.
The positioning of implants for an RP-4 overdenture is critical to the successful outcome of the prosthesis. For example, a Hader clip requires the mesiodistal implant spacing to be greater than 6 mm from edge to edge of the implant bodies. Because of this space requirement, the number of implants is reduced, especially if placed between the interforaminal space of the mandible. Additionally, in the apicocoronal dimension, adequate interocclusal space is needed to allow for at least 2 mm of acrylic to retain the denture teeth with overdentures; approximately 15 mm is needed from the crest of the bone to the incisal edge.
Implant number.
For a totally implant-supported prosthesis (RP-4), four to five implants are required in the mandible and six to eight implants in the maxilla. Fewer implants being utilized to support a RP-4 prosthesis will result in possible overloading of the prosthesis and/or implants leading to complications.
RP-5
Definition.
RP-5 is a removable prosthesis combining implant and soft tissue support. Predominately, the soft tissue is the primary support (primary stress-bearing areas) and implants are used for secondary support. The advantage of an RP-5 restoration is the reduced cost because fewer implants may be inserted compared with a RP-4 or fixed restoration. Additionally, there is less demand for bone augmentation, which decreases cost.
Implant Criteria.
Implants in the mandible are inserted within the mandibular interforaminal space with two, three, or four implants. These correspond to the Overdenture Treatment Planning options (e.g., OD-1–OD-5). In the maxilla, usually four to six implants are recommended depending upon force factors.
Complication.
The most common complication occurring with an RP-5 prosthesis is the associated movement. A common misconception of patients is they believe that implants, independent of the number, should have no associated movement. Because an RP-5 relies on the soft tissue for support, there will be inherent movement within the prosthesis. Additionally, with an RP-5 prosthesis, because of the primary implant support, soft tissue pressure is present, which may cause sore spots. If a patient’s initial complaint is chronic posterior sore spots, an RP-5 is not the best prosthetic option.
Prevention
Patient communication.
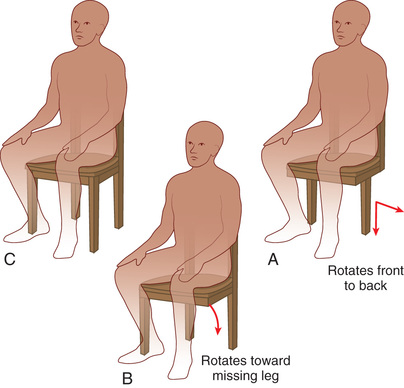
The patient should have a thorough understanding of the differences between an RP-4 and an RP-5 prosthesis. A common problem with an RP-5 prosthesis is the possible associated movement, which some patients may not tolerate or expect. A preoperative explanation must allow the patient a full understanding of the advantages and disadvantages of the two types of prostheses. A common analogy is the use of a chair. A two-implant overdenture is similar to a chair with only two legs. The chair may be stabilized; however, it can easily be moved. A three-implant overdenture is similar to a three-legged chair because it is more stable than two-implant overdenture; however, it will still have some degree of movement. A four- to five-implant overdenture is similar to a four-legged chair, which is associated with minimal movement (Fig. 3.13).
Treatment denture.
A preimplant treatment denture may be fabricated to determine position and prosthesis thickness. However, this is usually less important than in a RP-4 type prosthesis.
Posterior ridge form.
If the patient has a poor posterior ridge form (mandible), especially in the posterior area, an RP-5 prosthesis might not be the ideal treatment option. In these cases, patient education and consent is mandatory so they fully understand the limitations of this type of prosthesis.
Implant position.
The positioning of implants for an RP-5 overdenture is critical to the successful outcome of the prosthesis. When a bar is not going to be utilized, great care should be exercised to make sure that adequate spacing between the implants is present. Lack of space between implants (<3 mm), will result in prosthetic attachment complications. Additionally, the implants should be placed at approximately the same height and as parallel as possible to prevent path of insertion complications.
Implant number.
For a totally implant-supported prosthesis, a minimum of two to four implants is required in the mandible and four to six implants in the maxilla. Fewer implants will result in additional mobility of the prosthesis or occlusal overloading.
Continuous residual ridge bone loss.
The clinician and the patient should realize that the residual bone will continue to resorb in the soft tissue–borne regions of the prosthesis. Relines and occlusal adjustments every few years are common maintenance requirements of an RP-5 restoration. Bone resorption in the posterior regions with RP-5 restorations may occur two to three times faster than the resorption found with full dentures.6 This may be a determining a factor when considering this type of treatment in younger patients despite the decreased cost and lower failure rate (Fig. 3.14).

Divisions of Available Bone
Quantity of Available Bone
After the type of prosthesis is determined, the available bone for implant placement is evaluated to determine the surgical approach necessary (i.e., bone augmentation, implant insertion, or both) to support the intended prosthesis. The available bone concept describes the amount of bone in the edentulous area considered for implantation. Available bone is measured in width, height, length, and angulation and crown height space (CHS) in relation to the remaining bone (Fig. 3.15). If the bone is inadequate to predictably support an implant, a bone graft is considered in the ideal site(s), or alternative sites may be considered when additional implant numbers are necessary.

Not Understanding the Parameters of the Available Bone
To avoid complications in assessing the available bone present, the implant clinician must understand the correct parameters in determining the bone height, width, and length.
Available Bone Height.
The available bone height is first determined by radiographic evaluation (preferably cone beam computed tomography [CBCT]) in the edentulous region by measuring from the crest of the edentulous ridge to the opposing anatomic landmark. The anterior regions of the jaws have the greatest height due to the pneumatization of the maxillary sinus and the inferior alveolar nerve limits this dimension in the mandibular posterior regions. The maxillary canine eminence region, just lateral to the lateral piriform rim of the nose, often offers the greatest height of available bone in the maxillary anterior (Fig. 3.16).7

As a general rule, the anterior mandible has the greatest bone height. There is more bone apical to the mandibular anterior teeth than any other region. Even after the resorption of the residual ridge after tooth loss, there is usually adequate bone to insert dental implants (Fig. 3.17). However, the crown height of the prosthesis may be extensive (e.g., FP-2, FP-3) because of the loss of bone. This region often has the most available bone but also may have the greatest crown height space.

The anterior bone region in the mandible extends between the right and left mental foramens. The mental foramen is most often found in close proximity to the two premolars. The anterior region of bone extends beyond the canines and to the first premolar region most often. The initial mandibular bone height is influenced by skeletal anatomy, with Angle Class II patients having shorter mandibular height and Angle Class III patients exhibiting the greatest height.
The opposing landmarks for both the maxilla and mandible of the initial available bone height are more limiting in the posterior regions distal to the first premolar. In the maxillary posterior jaw region, there is usually greater bone height in the first premolar than in the second premolar, which has greater height than the molar sites because of the concave morphology of the maxillary sinus floor. As a consequence, the existing bone anatomy of the implant patient often requires modification (e.g., sinus augmentation) to enhance long-term implant success (Fig. 3.21).

The posterior height of bone in the mandibular region is reduced because of the presence of the mandibular canal, situated approximately 12 mm above the inferior border of the mandible (Fig. 3.18). Generally, less available bone is present in the higher force areas of the posterior mandible and maxilla; however, many treatment plans include shorter and fewer number of implants. Oikarinen et al found that more than 6 mm of bone height is found in less than 50% of posterior mandibles and 40% of posterior maxillae in partially edentulous patients.8

In the literature, the suggested minimum bone height for predictable long-term endosteal implant survival approaches 12 mm. Failure rates reported in the literature for implants shorter than 9 mm tend to be higher, independent of the manufacturer design, surface characteristic, and type of application.9,10
The available bone height in an edentulous site is the most important dimension for implant consideration because it affects both implant length and associated crown height. Crown height space directly affects force factors and esthetics. In addition, bone augmentation is more predictable in width than height, so even when the width is inadequate for implant placement, bone grafting may be used to create a site ideal for restorative and implant insertion requirements.
Available Bone Width.
The width of available bone is measured between the facial and lingual plates at the crest of the potential implant site. The crestal aspect of the residual ridge in the mandible is often cortical in nature and exhibits greater density than the underlying trabecular bone regions. This mechanical advantage permits immediate fixation of the implant, provided this cortical layer has not been removed by osteoplasty.
The crest of the edentulous ridge is most often supported by a wider base in the anterior mandible. In most mandibular situations, because of this triangular cross-section, an osteoplasty provides greater width of bone, although of reduced height (Fig. 3.19).

It should be noted that crest reduction (osteoplasty) affects the location of the opposing landmark, with possible surgical consequences, including implant size selection, implant position, and final prosthesis design. This is particularly important when a FP-1 prosthesis is planned, with the goal of obtaining a normal contour and proper soft tissue drape around a single tooth replacement.
Unlike the anterior mandible, the anterior maxilla often does not follow the triangular anatomy. The palatal plate of bone is more parallel to the facial plate in the maxilla (Fig. 3.20). In addition, many edentulous ridges exhibit a labial concavity in the incisor area, with an hourglass configuration. As a result, osteoplasty does not increase the width of bone as much as in the mandible. As a consequence, bone augmentation for width is more often indicated in the maxilla.

After adequate height is available, the next most significant factor affecting the long-term survival of endosteal implants is the width of the available bone. Root form implants with crestal diameters of 4 mm usually require more than 6 mm of bone width to ensure sufficient bone thickness and blood supply around the implant for predictable survival. This dimension provides more than 1 mm of bone on each side of the implant at the crest. Because the bone usually widens apically in the mandible, this minimum dimension rapidly increases. For root form implants, the minimum bone thickness is located in the midfacial and midlingual contours of the crestal region exclusively (Fig. 3.21).
Available Bone Length.
The mesiodistal length of available bone in an edentulous area is often limited by adjacent teeth or implants. As a general rule, the implant should be at least 1.5 to 2.0 mm from an adjacent tooth and 3 mm from an adjacent implant. This dimension not only allows minor surgical error but also compensates for the width of an implant or tooth that acquires a crestal defect, which is usually less than 1.4 mm. As a result, if bone loss occurs at the crest module of an implant or from periodontal disease with a tooth, the vertical bone defect will not spread to a horizontal defect and cause bone loss on the adjacent structure.11 In the case of a single-tooth replacement, the minimum length of available bone necessary for an endosteal implant depends on the width of the implant. For example, a 5-mm–diameter implant should have at least 8 mm of mesiodistal bone, so 1.5 mm is present on each side of the implant. A minimum mesiodistal length of 7 mm is usually sufficient for a 4-mm–diameter implant.
The diameter of the implant is also related to the width of available bone and, in multiple adjacent sites, is primarily limited in this dimension. For example, a width of bone of 4.5 mm without augmentation requires a 3.5-mm or smaller implant, with inherent compromises (e.g., less surface area and greater crestal stress concentration under occlusal loads on abutment screw and marginal bone). In narrow ridges, it is often indicated to place two or more adjacent narrow-diameter implants (when possible) to obtain sufficient implant–bone surface area to compensate for the deficiency in width of the implant. Because the implants should be 3 mm apart and 1.5 to 2.0 mm from each tooth, 13 mm or more in available bone mesiodistal length may be required when the narrower implant dimensions are used to replace a posterior tooth.
The ideal implant mesiodistal width for single-tooth replacement is often related to the natural tooth being replaced in the site. The tooth has its greatest width at the interproximal contacts, is narrower at the cementoenamel junction (CEJ), and becomes even narrower at the initial crestal bone contact, which is 2 mm below the CEJ.12 The ideal implant diameter corresponds to the width of the natural tooth, which may be measured 2 mm below the CEJ of the adjacent tooth. In this way the implant crown emergence (emergence profile) through the soft tissue may be similar to that of a natural tooth. For example, a maxillary first premolar is approximately 8 mm at the interproximal contact, 5 mm at the CEJ, and 4 mm at a point 2 mm below the CEJ. A 4-mm–diameter implant (at the crest module) would be the ideal if it is positioned at least 1.5 mm from the adjacent roots (2 mm below the CEJ).
Available Bone Angulation.
Bone angulation is the fourth determinant for the evaluation of available bone. The alveolar bone angulation represents the natural tooth root trajectory in relation to the occlusal plane. Ideally, this angulation is perpendicular to the plane of occlusion, which is aligned with the forces of occlusion and is parallel to the long axis of the prosthodontic restoration. The incisal and occlusal surfaces of the teeth follow the curve of Wilson and curve of Spee. As such, the roots of the maxillary teeth are angled toward a common point. The mandibular roots flare, so the anatomic crowns are more lingually inclined in the posterior regions and labially inclined in the anterior area compared with the underlying roots. The first premolar cusp tip is usually vertical to its root apex.
The maxillary anterior teeth are the only segment in either arch that does not receive a long-axis load to the tooth roots but instead are usually loaded at an approximate 12-degree angle. As such, their root diameter is greater than the mandibular anterior teeth. In all other regions of the mouth, the teeth are loaded perpendicular to the curves of Wilson and Spee.
Rarely does the bone angulation remain ideal after the loss of teeth, especially in the anterior edentulous arch. In this region, labial undercuts and resorption after tooth loss often mandate greater angulation of the implants or correction of the site before insertion (osseous augmentation). For example, in the anterior mandible, the implant insertion often engages the lingual cortical plate, rather than the inferior border of the mandible, as a consequence of the position of the incisal edge and the angulation of bone. In the posterior mandible, the submandibular fossa mandates implant placement with increasing angulation as it distally progresses. Therefore, in the second premolar region the angulation may be 10 degrees to a horizontal plane; in the first molar areas, 15 degrees; and in the second molar region, 20 to 25 degrees.
The limiting factor of angulation of force between the body and the abutment of an implant is the width of bone. In edentulous areas with a wide ridge, wider root form implants may be utilized. Implants may allow up to 30 degrees of divergence with the adjacent implants, natural teeth, or axial forces of occlusion with minimum compromise. However, angled loads to an implant body increases the crestal stresses to the implant components and bone, but the greater-diameter implant decreases the amount of stress transmitted to these structures. In addition, the greater width of bone offers some latitude in angulation at implant placement. The implant body may often be inserted so as to reduce the divergence of the abutments without compromising the permucosal site.
An acceptable bone angulation in the wider ridge may be as much as 30 degrees. The narrow yet adequate width ridge often requires a narrower design root form implant. Compared with larger diameters, smaller-diameter designs result in greater crestal stress to the system (abutment screws, crestal bone) and may not offer the same range of custom abutments. In addition, the narrower width of bone does not permit as much latitude in placement regarding angulation within the bone. This limits the acceptable angulation of bone in the narrow ridge to 20 degrees from the axis of the adjacent clinical crowns or a line perpendicular to the occlusal plane (Fig. 3.22).

Crown Height Space.
The crown height space (CHS) is defined as the vertical distance from the crest of the ridge to the occlusal plane. It affects the appearance of the final prosthesis and may affect the amount of movement force on the implant and surrounding crestal bone during occlusal loading. Esthetically, the prosthesis is less likely to replace the sole anatomic crowns of natural teeth when a greater CHS is present.
The CHS may be considered a vertical cantilever. Any direction of load that is not in the long axis of the implant will magnify the crestal stresses to the implant-bone interface and to the abutment screws in the restoration. The greater the CHS, the greater the moment force or lever arm with any lateral force or cantilever (Fig. 3.23).

The absence of a periimplant ligament means that the bone-implant stresses cannot be reduced by increasing the implant height. Therefore, as the CHS increases and a cantilever or a lateral load is planned on the restoration, a greater number of implants or wider implants should be inserted to counteract the increase in stress. For an ideal treatment plan, the CHS should be equal to or less than 15 mm under ideal conditions.
Not Understanding the Divisions of Bone: Division A (Abundant Bone)
The Division A edentulous ridge exhibits abundant bone in all dimensions of height, width, and length. Division A root form implants are optimal and most often used as independent support for a fixed or removable prosthesis. Division A bone is the ideal type of bone to provide a natural looking FP-1 prosthesis.
Criteria Division.
Division A bone corresponds to abundant available bone in all dimensions; the height of 12 mm or more, width of >6 mm, angulation <30 mm, and crown height space of <15 mm. Osteoplasty may often be performed to obtain additional bone width in the mandible when a larger diameter implant is desired. In rare instances, an angle abutment will be required; however, the direction of load is not excessive (Box 3.1).
Surgical Treatment.
The implant choice in Division A bone is a Division A root form that is 4 mm or greater in diameter and 12 mm or longer in height (length). A larger-diameter implant is suggested in the molar regions (5 to 6 mm in diameter). Longer implants are suggested in immediate loading treatment options or when an implant is immediately inserted after the extraction of the tooth. As a general rule, Division A bone should not be treated with smaller-diameter implants for the final prosthesis, unless dictated by the specific tooth replacement (e.g., maxillary lateral incisors or mandibular incisors) (Fig. 3.24). There are several advantages to the use of implants equal to or greater than 4 mm in diameter compared with smaller-diameter implants (Box 3.2).

Prosthetic Treatment
Fixed.
FP-1 restorations require a Division A ridge. However, a FP-2 prosthesis most often also requires a Division A bone. A FP-2 restoration is the most common posterior restoration supported by multiple adjacent implants in partially edentulous patients because of either bone loss or osteoplasty prior to implant placement. A FP-3 prosthesis is most often the option selected in the anterior Division A bone when multiple adjacent teeth are missing and the maxillary smiling lip position is high, or a mandibular low lip line during speech exposes regions beyond the natural anatomical crown position.
Removable.
For removable implant overdentures in Division A bone, the final position of the tooth and superstructure bar must be evaluated before surgery. A limited CHS is more common in Division A bone, and an RP-4 or RP-5 restoration may require osteoplasty before implant placement. Division A bone may represent a contraindication for high-profile O-ring attachments or superstructures placed several millimeters above the tissue. This may result in difficulty in prosthesis fabrication, esthetics, hygiene, adequate strength of the prosthesis.
Complications.
Complications with Division A bone are minimal. The most common complication is not assessing the crown height space, which may impinge on the prosthetic rehabilitation. Many clinicians fail to educate the patient about the rapid decrease in bone volume width and the consequences of delaying treatment. When the bone volume is Division A, there is a decrease in treatment costs, with a reduction in the number and complexity of surgeries to the edentulous area (Fig. 3.25).

Not Understanding the Divisions of Bone: Division B (Barely Sufficient Bone)
The decreased width and surface area usually require additional implants to be included in the final prosthesis design. Division B may be changed to Division A by augmentation or osteoplasty. The treatment options may be selected in light of the area to be treated. For example, in the anterior maxilla, augmentation is most often selected because of esthetics. In the anterior mandible, osteoplasty is common because of the available bone height and low esthetic concerns. In the posterior mandible, multiple Division B implants may be used when the bone density is favorable, the available bone height is limited, and esthetics are not a primary factor. When stress factors are a concern, bone augmentation precedes Division B root form implants regardless of the anatomic location (Box 3.3).
As the bone resorbs, the width of available bone first decreases at the expense of the facial cortical plate because the cortical bone is thicker on the lingual aspect of the alveolar bone, especially in the anterior regions of the jaws. This may result in a 25% decrease in bone width the first year and a 40% decrease in bone width within the first 1 to 3 years after tooth extraction.13 The resulting narrower ridge is often inadequate for most 4-mm-diameter root form implants (Box 3.4).
Complications
Division B root forms.
Division B bone offers sufficient available bone height with compromised bone width. The Division B available bone width may be further classified into ridges 4 to 6 mm wide and B minus width (B−w) 2.5 to 4 mm wide, where bone grafting is indicated most likely (Fig. 3.26). Because the ridge width and implant diameter are narrower, and forces increase as the angle of load increases, the angulation of occlusal load is also less and should be ideally within 20 degrees from the axis of the adjacent teeth or occlusal plane. A CHS of 15 mm or less (similar to Division A) is necessary in Division B to decrease the moment of forces with lateral or offset loads, especially because of the smaller width dimension.

Not understanding the need for modification.
Three treatment options are available for the Division B edentulous ridge:
1. Modify the existing Division B ridge to Division A by osteoplasty to permit the placement of root form implants 4 mm or greater in width. When more than 12 mm of bone height remains after osteoplasty, the Division B bone is converted to Division A. When less than 12 mm of bone height remains after osteoplasty, a biomechanical disadvantage results due to the ridge being changed to a Division C−h (Fig. 3.27).

2. The second treatment option is the placement of a narrow diameter implant (3–4 mm diameter and 12 mm or more in length; Fig. 3.28). Smaller-diameter root form implants (3.0–3.5 mm) are designed primarily for Division B available bone. Because Division B bone is compromised in width, there exists less margin of error in the ideal placement. The Division B root form implants present several inherent disadvantages compared with the larger-diameter implants.14 As a result of these concerns for the Division B root form, this option is most often used for single-tooth replacement of a maxillary lateral incisor or mandibular incisors, where the restricted available bone is in mesiodistal width, or with multiple implants in the posterior mandible, where bone density is good and esthetic requirements are limited.

3. The third alternative treatment for Division B bone is to change the Division B ridge into a Division A by grafting the edentulous ridge with autogenous bone or allogenic bone (Fig. 3.29). A disadvantage of this treatment plan includes the need for adequate bone healing. The emergence profile angle of the final crown, which does not compromise hygiene, requires a Division A root form implant (with the exception of maxillary lateral incisors or mandibular incisors). Stress factors may also dictate the augmentation approach to Division B bone in order to utilize larger-diameter implants. In the presence of unfavorable stress factors, the number and width of abutments should be increased without increasing the CHS to provide a greater surface area of resistance to the magnified forces, which most likely will require augmentation. To accomplish this goal, augmentation is most ideal in Division B bone.

Modification from Division B to Division A may lead to a change in prosthesis.
When a Division B ridge is changed to a Division A by osteoplasty procedures, the final prosthesis design has to compensate for the increased CHS. For example, before surgery, the available bone height may be compatible with an FP-1 prosthetic design. If, at the time of surgery, the ridge is found deficient in width for implant placement, it is not unusual to remove crestal bone before reaching a Division A width. This means the final restoration will require an additional height. It may result in an extended tooth (FP-2, FP-3) restoration, which may not be acceptable to the patient.
Insufficient osteoplasty.
The most common approach to modify the narrower Division B ridge into another bone division by osteoplasty is when the final restoration is a mandibular implant overdenture. Because of the resorptive process that occurs in the anterior mandible, an osteoplasty is usually indicated to allow for adequate bone width if the CHS is less than 15 mm; this maybe be advantageous for a fixed prosthesis and problematic for a removable prosthesis. When a RP-4 or RP-5 is planned, care should be noted to make sure adequate CHS is available. If insufficiency osteoplasty is performed, lack of space will be available for the prosthesis, which may lead to prosthesis fracture, tooth fracture, or tooth delamination. Ideally, greater than 2 mm of acrylic is required to secure an attachment or a denture tooth (Fig. 3.30).

Not Understanding the Divisions of Bone: Division B−w (B Minus Width)
The distinction between Division B and Division B−w is especially important when augmentation is the method of choice. Bone augmentation is more predictable when the volume to augment is minimal and is for width and least predictable when additional bone height is desired. For example, a width increase of 1 to 2 mm may be obtained with an alloplast and guided bone regeneration, but more than 2 mm of width is more predictable with autologous bone as part of the graft.
Complications
More bone augmentation required.
The Division B−w ridge will usually require more than 2 mm of width increase, and therefore autologous bone or an autologous/allogenic graft is beneficial to predictably grow the additional bone width. If the Division B−w ridge contour requires alteration altered for improved prosthodontic relationships, an onlay particulate or block graft of autogenous bone is indicated. The autograft may be harvested from an intraoral region (e.g., the mandibular symphysis or ramus) and placed along the lateral aspect of the ridge that corresponds to ideal arch form. The implant placement is usually delayed for 4 to 6 months after the augmentation process to permit ideal implant placement and to ensure complete bone formation before placing the implant.
Bone resorption progression.
The patient delaying treatment with a Division B bone situation should be informed of the future bone volume resorption that presents from disuse atrophy. The augmentation of bone in height is much less predictable and requires more advanced techniques than augmentation of bone width alone (Fig. 3.31). For example, the patient may not be experiencing problems with a maxillary denture, but the Division B bone will resorb in height and decrease the stability and retention of the removable soft tissue–supported prosthesis. When treatment is delayed until patient problems begin, the overall result may be more difficult to achieve and more costly to the patient.

Final prosthesis.
The final prosthesis type for Division B ridges is dependent on the surgical option selected. Whereas grafted ridges will more often be used when a fixed prosthesis is desired, ridges treated with osteoplasty before implant placement are likely to be supporting removable prostheses. The treatment option may be influenced by the region to be restored. For example, in a partially edentulous anterior maxilla, augmentation is most often selected because of esthetics, and the parallel bony anatomy of the residual ridge is not conducive for osteoplasty to gain bone width. In the edentulous anterior mandible, osteoplasty is common. In the premolar region of the posterior mandible, Division B root form implants are often used because the bone density is adequate, available bone height is limited and may be reduced after osteoplasty, and esthetics are often not a major factor.
Not Understanding the Divisions of Bone: Division C (Compromised Bone)
The Division C edentulous ridge exhibits moderate resorption and presents more limiting factors for predictable endosteal implant placement. The decision to restore with endosteal implants or to change to a more favorable bone division via augmentation before implant placement is influenced by the prosthesis, patient force factors, and patient’s desires.
The Division C ridge is deficient in one or more dimensions (width, length, height, or angulation) (Box 3.5) regardless of the position of the implant body into the edentulous site. The resorption pattern of bone occurs first in width and then in height. As a result, the Division C ridge continues to resorb in width, until it becomes inadequate for any design of endosteal implant.
Box 3.5
Division C Bone
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


