This case report describes the treatment of a 30-year-old woman with a Class II Division 1 malocclusion, characterized by a large overjet, a deep overbite, and a V-shaped maxillary dental arch. She had a convex profile with a retrognathic mandible and marked lip protrusion. Treatment involved extraction of 4 first premolars and miniscrew implant anchorage for space closure. The total treatment time was about 20 months. Ideal overjet and overbite relationships were established, and the facial profile was improved substantially. The 2-year follow-up records show a morphologically and functionally stable result.
Class II malocclusion is the most frequent treatment problem seen in an orthodontic practice. Facial esthetics is a major concern of many orthodontic patients. A convex facial profile with marked lip protrusion often affects the psychological health of patients. In such circumstances, the major orthodontic treatment goals are to reduce the proclination of the maxillary incisors and improve the facial profile. Therefore, the treatment plan often includes extraction of 2 or 4 premolars, followed by retraction of the anterior teeth by using maximum anchorage.
Anchorage control in severe skeletal Class II patients is a difficult problem in orthodontic treatment. To reinforce anchorage, various auxiliaries can be used, including headgear, lingual arch, transpalatal arch, holding arch, and intermaxillary elastics. However, these appliances require the patient’s cooperation to be effective. To obtain absolute anchorage without patient cooperation, dental implants, screws, and miniplates have been used for skeletal anchorage.
Screws have many advantages—eg, ease of implantation and removal, low cost, possible immediate loading, and possible placement in most areas of the alveolar bone. Incisor retraction with miniscrew anchorage is a new strategy for treating skeletal Class II patients. Our objective in this case report is to demonstrate the advantages of treatment with miniscrew anchorage for incisor retraction in a patient with an Angle Class II Division 1 malocclusion.
Diagnosis and etiology
The patient was a 30-year-old woman, whose chief complaint was her convex facial profile with marked lip protrusion. She had a Class II malocclusion with a 10-mm anterior overjet. Her father had a similar malocclusion. Her periodontal health was good, and her temporomandibular joints were asymptomatic.
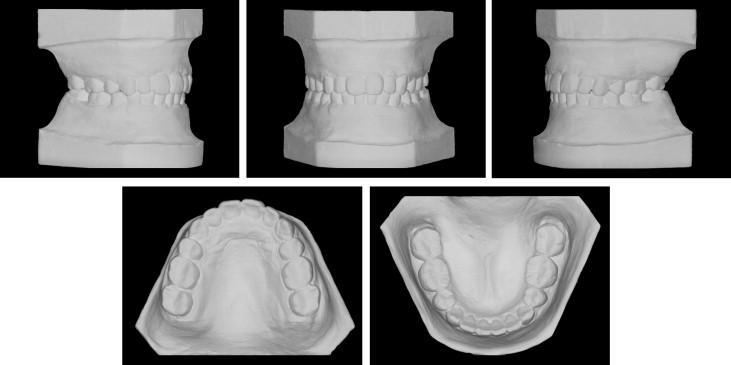
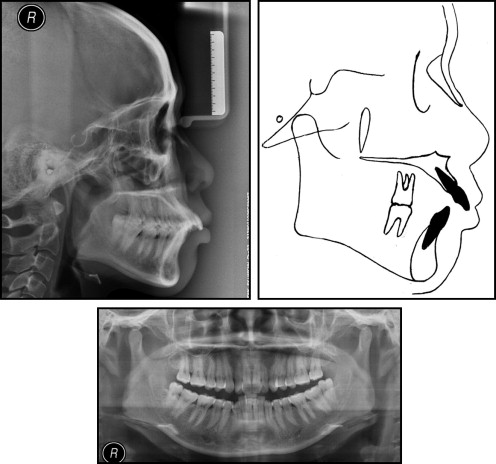
The facial photographs showed a convex facial appearance, a protruded upper lip, overexposure of the maxillary incisors, and a gummy smile ( Fig 1 ). The dental casts showed severe maxillary protrusion with a large overjet, deep overbite, and transverse deficiency with narrow dental arches ( Fig 2 ). The molar relationship was Angle Class II on both sides. The amounts of crowding were 0.5 mm in the maxillary arch and 5.5 mm in the mandibular arch. The panoramic radiograph ( Fig 3 ) showed that she had mandibular third molars. Cephalometric analysis indicated a skeletal Class II jaw deformity ( Fig 3 ). The ANB angle was 5.8°, and the Wits appraisal was 5.7 mm. The SNA angle of 80.9° reflected a normally positioned maxilla, and the SNB angle of 75.1° indicated mandibular deficiency. The U1-NA angle of 34.7° indicated that she had significant proclination of her maxillary incisors.

Treatment alternatives
To accomplish these objectives, we identified 3 treatment alternatives. All 3 called for extraction of the mandibular third molars to facilitate mandibular molar uprighting. The first option consisted of correcting the Class II malocclusion with a combination of surgery and orthodontic treatment. This protocol would provide a better esthetic result, but the risks and treatment expenses would be high. The parents did not want this treatment option.
The second alternative was to extract the maxillary first premolars, correcting the excessive overjet by retracting the maxillary incisors and leaving the posterior occlusion with a Class II molar relationship. This option would correct the incisor proclination, but the treatment would be difficult, because of the excessive overbite and overjet, which often require more effort when retracting the canines and the incisors.
The third alternative was orthodontic treatment with extraction of the 4 first premolars, with miniscrews for implant anchorage. We believed that the miniscrew implant could provide absolute anchorage in the retraction of the maxillary anterior teeth and improve the patient’s facial profile. This option was selected.
Treatment progress
After extraction of the maxillary and mandibular first premolars and the mandibular third molars, fixed appliances were placed in both arches. Maxillary posterior miniscrew implants (diameter, 1.2 mm; length, 8 mm; Absoanchor AX12-108; Dentos, Taegu, South Korea) were inserted into the buccal alveolar bone between the maxillary second premolars and the first molars ( Fig 4 ).

After initial leveling and alignment, rectangular 0.019 × 0.025-in stainless steel archwires were used to close the extraction spaces with sliding mechanics. Class II elastics (3/16 in, 3.5 oz; 3M Unitek, Monrovia, Calif) were added to retract the maxillary incisors and establish a Class I molar relationship ( Fig 5 ).

After final arch coordination and minimal occlusal equilibration, all appliances were debonded. The miniscrew implants were removed without anesthesia. After 20 months of treatment, proper overjet and overbite were achieved. For retention, the patient was instructed to wear removable retainers for 24 hours a day for the first year and then at night only for the next year.
Treatment results
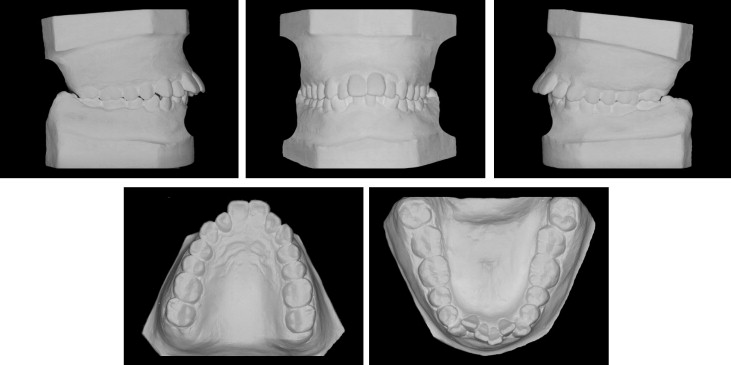
The posttreatment facial photographs ( Fig 6 ) show improvement in the facial profile. The intraoral photographs and dental casts ( Figs 6 and 7 ) show satisfactory dental alignment, bilateral Class I canine and molar relationships, and normal overjet and overbite. The cephalometric analysis ( Fig 8 ) shows that the ANB angle was 4.2°. The Wits appraisal was 0.9 mm, and the U1-NA angle was 20.1° ( Table ). All these demonstrate the changes from a skeletal Class II pattern to a skeletal Class I pattern. The panoramic radiograph ( Fig 8 ) showed that all extraction spaces were closed, and the roots had been paralleled. No obvious root resorption had occurred. The sella-nasion superimposition indicated that the maxillary incisors were retracted, and the facial profile was improved. The patient’s 2-year follow-up records showed good stability with no obvious relapse ( Figs 9-11 ). The occlusion was stable, and the improved facial harmony had been retained.