The goal of this report was to illustrate new treatment mechanics for using microimplants for the treatment of a Class II Division 2 deepbite malocclusion. A 29-year-old woman with a deepbite was treated with the aid of microimplant anchorage. Microimplants placed between the maxillary second premolars and first molars were used as anchorage to apply a distal force to the anterior teeth to correct the Class II canine and molar relationships. A distal force was applied to long hooks that were crimped between the lateral incisors and the canines. By applying a backward force to the long hooks, the maxillary anterior teeth experienced palatal root movement with no change in the vertical and anteroposterior positions of the incisal edges. The distal extrusive movement of the maxillary second molars achieved by disengaging the second molars from the archwire during distal force application and an anterior bite-block bonded on the lingual surface of the maxillary central incisors produced the increase in vertical dimension. The distal force to the long extended hooks from the microimplants was possibly good mechanics for obtaining the palatal root movement and correcting the Class II canine and molar relationships. The anterior bite-block and disengagement of the maxillary second molars during distal force application were effective for increasing the vertical dimension.
A deepbite is considered a difficult malocclusion to treat. The treatment of deepbite has included orthognathic surgery and orthodontic treatment by intrusion of the anterior teeth or extrusion of the posterior teeth in either or both of the maxillary and mandibular arches. A decision for molar extrusion or intrusion of incisors should be based on the causes and the vertical positions of the incisal edges of the maxillary incisors relative to the upper lip.
Distalization of the maxillary posterior teeth is often needed in the treatment of Class II malocclusion when a nonextraction treatment is planned. Many extraoral and intraoral appliances have been developed to distalize the molars. Extraoral appliances can provide reliable anchorage but only in compliant patients. On the other hand, all intraoral molar distalizing appliances produce adverse side effects such as labial tipping of the maxillary anterior teeth.
With the development of extradental skeletal anchorage such as microimplants, clinicians can now move teeth without anchorage loss to the specific planned goal. The tooth movement can also be precisely controlled with the help of microimplants. Many clinical reports and studies have focused on treating the various types of malocclusions, including bialveolar protrusion requiring maximum retraction of the anterior teeth, whole arch distal retraction, intrusion of a tooth or teeth, and protraction of the molars. However, there has been no report to illustrate the treatment mechanics involved with microimplants in skeletal Class II deepbite treatment. In the treatment of a deepbite, the maxillary or mandibular incisors can be intruded by conventional or microimplant-aided mechanics. However, in a patient with proper vertically positioned maxillary incisors, their intrusion is not desirable. Lingually tipped maxillary incisors should be uprighted by distal root movement, which requires strong anchorage. The microimplant can be used to provide anchorage for root movement of the maxillary incisors and distal retraction of the whole maxillary dentition to correct Class II relationships.
In this report, we illustrate effective microimplant mechanics for the treatment of Class II deepbite malocclusion by palatal root movement of the maxillary anterior teeth, distal movement of the whole maxillary dentition, and an increase of the vertical dimension.
Case report
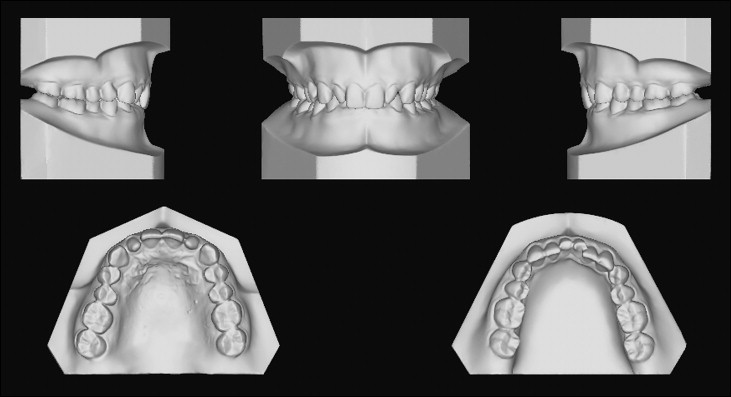
A 29-year-old woman’s chief concern was a deepbite ( Fig 1 ). She had a decreased vertical dimension, a deep mentolabial fold, and a negative E-line value. The cephalometric analyses showed that she had a Class III skeletal pattern. However, because of peg-shaped lateral incisors and lingually tipped maxillary incisors, the canines and molars showed Class II relationships. The maxilla was slightly retropositioned; the SNA angle was 2° under normal, and the ANB angle was 0.8° ( Table ). The patient had a severe brachyfacial pattern; the FMA angle was 14.1° and the gonial angle was 107.3°. There was no apparent facial asymmetry or transverse discrepancy.

| Pretreatment | Posttreatment | |
|---|---|---|
| SNA (°) | 80.5 | 78.9 |
| SNB (°) | 79.7 | 78.1 |
| ANB (°) | 0.7 | 0.8 |
| A to N-per (mm) | 1.8 | 1.2 |
| Pog to N-per (mm) | 1.1 | 1.0 |
| Co-A (mm) | 93 | 90 |
| Co-Gn (mm) | 121 | 121 |
| ANS-Me (mm) | 62.6 | 66.3 |
| FMA (°) | 14.1 | 16.7 |
| PFH/AFH | 53/61.5 (0.86) | 53.5/65 (0.82) |
| FH to OP | 6 | 6.4 |
| FH to UI | 96.2 | 106.1 |
| IMPA (°) | 95 | 98 |
| Z-angle (°) | 85.4 | 85.8 |
| Nasolabial angle (°) | 93 | 104 |
| Upper lip to E-line (mm) | −3.7 | −5.5 |
| Lower lip to E-line (mm) | −5 | −6 |
Intraorally, the patient had a Class II Division 2 deepbite malocclusion ( Figs 1 and 2 ). The maxillary lateral incisors were peg-shaped, and the mandibular central incisors exhibited severe attrition and discoloration from trauma 12 years previously. Overjet and overbite were 2 and 6.5 mm, respectively, and arch-length discrepancies in the maxilla and the mandible were +2 and –5.8 mm, respectively. If the lateral incisors were built up to normal size with composite resin, the arch-length discrepancy in the maxillary arch would become –3 mm. The vertical position of the maxillary incisors was 1 mm relative to the reposed upper lip. There were no signs and symptoms of temporomandibular joint disorders or root resorption.
Treatment objectives
Six treatment objectives were identified: (1) obtain Class I canine and molar relationships, (2) correct the overbite by extrusion of the posterior teeth (3) obtain proper inclination and position of the maxillary anterior teeth, (4) make space for cosmetic restoration of the maxillary lateral incisors, (5) increase the vertical dimension, and (6) obtain good retention.
Treatment objectives
Six treatment objectives were identified: (1) obtain Class I canine and molar relationships, (2) correct the overbite by extrusion of the posterior teeth (3) obtain proper inclination and position of the maxillary anterior teeth, (4) make space for cosmetic restoration of the maxillary lateral incisors, (5) increase the vertical dimension, and (6) obtain good retention.
Treatment plan
Distalization of the maxillary molars was planned to correct the Class II relationships. The inclination of the lingually tipped maxillary incisors also needed to be corrected. The distal movement of the posterior tooth segment and palatal root movement of the maxillary incisors required strong anchorage. For these reasons, the use of microimplants was proposed in the treatment plan. The initial facial photos showed a favorable profile, and the anteroposterior position of the maxillary incisors was planned not to change. The vertical position of the maxillary incisors relative to the upper lip was 1 mm, and their intrusion was not indicated. Instead, molar extrusion was proposed to open the anterior bite and obtain enhanced vertical facial proportions. This was achieved by bonding an anterior bite-block on the palatal surface of the central incisors and inducing the extrusion of the maxillary second molars by disengaging them from the archwire during distal force application.
Treatment progress
The traumatized mandibular central incisors were treated. All teeth in the maxillary arch except the second molars were fitted with fixed preadjusted edgewise appliances, and a 0.014-in nickel-titanium (NiTi) aligning archwire was ligated. Simultaneously, the microimplants (diameter, 1.2 mm; length, 6 mm; Absoanchor, Dentos, Daegu, Korea) were placed into the buccal alveolar bone between the maxillary second premolar and the first molar on both sides ( Fig 3 ). After 2 months of treatment, an anterior bite-block was bonded on the palatal surfaces of the maxillary central incisors to increase the vertical dimension ( Fig 4 ). The braces were subsequently bonded to all teeth in the mandibular arch. In the maxillary arch, a 0.016 × 0.022-in stainless steel archwire, with crimped 10-mm long hooks between the lateral incisors and the canines, was placed. Distal force was also applied from the microimplants to the hooks with NiTi coil springs. To increase the counterclockwise moment to the maxillary anterior teeth, the long hooks on the archwire were extended gingivally. After 5 months of treatment, there was distal movement of the maxillary posterior teeth. Vertical steps between the maxillary first and second molars resulted from slight intrusion of the first molars, and distal tipping and extrusion of the second molars was observed. The distal force transmitted to the maxillary posterior teeth had caused distal tipping and extrusion of the second molars. The vertical dimension was increased during treatment by 3-point contacts—the anterior bite-block and 2 second molars. To control the axial inclination of the maxillary anterior teeth, a 0.019 × 0.025 beta-titanium alloy archwire with long hooks with a torquing bend between the lateral incisors and the canines was used. The retraction force was applied continuously by the NiTi coil springs from long hooks to the microimplants ( Fig 5 ). After 12 months of treatment, buccal tubes were bonded onto the maxillary second molars, and the archwire was switched to 0.016-in NiTi. Up-and-down elastics were used to extrude the maxillary first molars to settle the occlusion ( Fig 6 ). After final arch coordination and minimal occlusal equilibration, all appliances were debonded. The microimplants were removed by unscrewing without anesthesia. The treatment time was 20 months. Lingual fixed retainers were bonded from the left first premolar to the right first premolar in the mandibular arch, and resin was built up on the maxillary lateral incisors. A wrap-around retainer with an anterior bite plate was also used to prevent relapse of the anterior overbite.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


