Introduction
The Fränkel function regulator III appliance (FR-3) has been used to correct Class III malocclusions for many years; however, its treatment effectiveness is controversial. In this study, we aimed to assess the effectiveness of the FR-3 in treating patients with Class III malocclusion in the growth and development period.
Methods
Medline (via PubMed), Cochrane Central Register of Controlled Trials, Embase, Chinese Biomedical Literature Database, China National Knowledge Infrastructure, VIP Database for Chinese Technical Periodicals, Scirus, Lilacs, Scopus, and World Health Organization International Clinical Trials Registry Platform were searched electronically. Relevant journals and reference lists of included studies were manually searched. The quality of the included studies was assessed with the Newcastle-Ottawa scale. The meta-analysis was carried out using RevMan (version 5.2; Nordic Cochrane Centre, Cochrane Collaboration, Copenhagen, Denmark).
Results
Seven high-quality cohort studies were included. The meta-analysis showed that SNA changes did not differ in the short (mean difference, 0.43°; 95% CI, −0.52°-1.39°) and long (mean difference, 0.37°; 95% CI, −0.29°-1.03°) terms. However, SNB changes significantly differed in the short (mean difference, −1.62°; 95% CI, −2.62° to −0.62°) and long (mean difference, −1.50°; 95% CI, −2.12° to −0.88°) terms. By contrast, MPA changes did not differ in the short term (mean difference, 0.55°; 95% CI, −0.74°-1.84°).
Conclusions
Clinical evidence suggests that the FR-3 might restrict mandibular growth but not stimulate forward movement of the maxilla. Further high-quality studies are necessary to confirm the effectiveness of the FR-3.
Mandibular prognathism and maxillary retrusion, which were first documented in the artwork left by Egyptians and Greeks, are categorized as Class III malocclusion and were clinically characterized as anterior crossbite after the invention and application of cephalometry. The treatment strategies of Class III malocclusion for patients in the growth and development period usually focus on growth modification with various functional appliances. In 1970, Fränkel invented an appliance called the function regulator type III (FR-3) to treat this type of malocclusion. The appliance is composed of wire and acrylic, with 4 acrylic parts. Two upper labial pads are positioned in the labial vestibule above the maxillary incisors, which are used to eliminate the restrictive pressure of the upper lip on the underdeveloped maxilla. Two vestibular shields extend from the depth of the mandibular vestibule to the height of the maxillary vestibule; they act to remove the restrictive forces created by the buccinators and the associated facial muscles. These pads can also stimulate labial alveolar bone apposition by stretching the adjacent periosteum.
Fränkel expected that the FR-3 could stimulate forward growth of the maxilla and restrict mandibular development by counteracting the forces of the surrounding muscles. However, much controversy exists on the treatment effectiveness of the FR-3. Some studies have demonstrated that with the FR-3, the mandible moved downward and backward, thus correcting a Class III malocclusion. Some researchers agreed that the malocclusion was corrected by a substantial effect on the stimulation of maxilla growth ; nevertheless, objections still exist. Most published studies involve small sample sizes and do not have sufficient power to confirm the effectiveness of the FR-3.
To date, Class III patients treated with the FR-3 still face concerns, such as whether the changes produced are skeletal or dentoalveolar, whether an influence on the maxilla or the mandible exists with respect to the transverse and sagittal dimensions, and whether treatment effects can be distinguished from normal growth. The purpose of this article was to perform a systematic review and a meta-analysis to evaluate the effectiveness of the FR-3 in patients with Class III malocclusion in the growth and development period compared with untreated patients.
Material and methods
A specified protocol was conducted in advance. Two calibrated reviewers (X.Y. and C.L.) independently carried out the study inclusion, data extraction, and risk of bias processes. The kappa score, which measures the level of agreement, was 0.92; this was a good score. Disagreements between the 2 reviewers were discussed with a third reviewer (D.B.) for consensus.
The inclusion criteria were the following. (1) Study type: randomized controlled trials, clinical controlled trials, and cohort studies. (2) Patients: all participants, with ages from 5 to 15 years, who were diagnosed as having an Angle Class III malocclusion in the growth and development period, without limitations for sex and race; the diagnostic criteria for Class III malocclusion were mandibular prognathism, maxillary retrusion, or anterior crossbite, including both skeletal and dental deformities. (3) The intervention group wore FR-3 appliances according to the clinicians’ instructions. (4) The control group received no treatment. (5) Outcome variables: changes in cephalometric measurements, including overbite and overjet in both groups.
The exclusion criteria were the following. (1) Patients had other diseases affecting growth and development. (2) Repetitive publication (only well-described articles were included).
The following electronic databases were searched for any published or ongoing study without language limitations: Medline (via PubMed), Cochrane Central Register of Controlled Trials (issue 9, 2013), Embase ( www.embase.com ), Scirus, Lilacs, Scopus, World Health Organization International Clinical Trials Registry Platform, Chinese BioMedical Literature Database, China National Knowledge Infrastructure, and VIP Database for Chinese Technical Periodicals. A total of 19 Chinese dental journals were manually searched in the library by scanning the titles and abstracts, and the MeSH words were extracted by the librarians. The reference lists of all included studies were also searched, and the “related articles” tool was used in the PubMed search. The updated search was performed in September 2013. The search strategy combined MeSH heading words with free-text words. The main search terms used were “malocclusion, Angle Class III” and “Fränkel appliance.” For example, the search strategy in PubMed used “function regulator type III OR FR-3 OR Fränkel-III OR Fränkel appliance and malocclusion, Angle Class III (MeSH terms) OR Class III malocclusion.” The titles and abstracts were first scanned to find any potentially eligible studies, and their full texts were obtained for final consideration. Any obscure or missing data were obtained by contacting authors.
The Newcastle-Ottawa Scale was applied to assess the quality of the studies. Using this “star system,” we judged each included study on the basis of 3 broad perspectives: the selection of the study groups (including 4 items and 1 star for each item), the comparability of the groups (with only 1 item but 2 stars at most), and the ascertainment of the outcome of interest (with 3 items and 1 star for 1 item) ( Table I ).
| Items | When to give stars | |
|---|---|---|
| Selection | Representativeness of the exposed cohort | Truly representative of the average in the community Somewhat representative of the average in the community |
| Selection of the nonexposed cohort | Drawn from the same community as the exposed cohort | |
| Ascertainment of exposure | Secure record Structured interview |
|
| Demonstration that outcome of interest was not present at start of study | Yes | |
| Comparability | Comparability of cohorts on the basis of the design or analysis | Study controls for the most important factor Study controls for any additional factor |
| Outcome | Assessment of outcome | Independent blind assessment Record linkage |
| Was follow-up long enough for outcomes to occur? | Yes (select an adequate follow-up period for outcome of interest) | |
| Adequacy of follow-up of cohorts | Complete follow-up Subjects lost to follow-up unlikely to introduce bias; small number lost follow-up, or description provided of those lost |
A customized data extraction form was developed. The following items were included: study identification, including the first author’s name and year of publication; study type; number of participants and their demographic data; setting; frequency of appliance wear and duration in the intervention and control groups; and cephalometric measurement results.
Statistical analysis
RevMan (version 5.2; Nordic Cochrane Centre, Cochrane Collaboration, Copenhagen, Denmark) was used in the data analysis. Statistical heterogeneity was explored using a test for heterogeneity (I 2 static) at α = 0.10. If I 2 >50% and P ≤0.10, the causes of the heterogeneity were analyzed, and subgroup analysis was done. If heterogeneity was high (I 2 >50%), the random-effects model was chosen for the meta-analysis; otherwise, the fixed-effects model was adopted. The combined results for the dichotomous data were expressed as relative risk and 95% confidence intervals. For continuous data, the mean difference with 95% confidence intervals, as well as the standard error, was calculated. The statistical significance of the hypothesis test was set at P <0.05 (2-tailed z tests). Sensitivity analyses were conducted, evaluating the pooled effect estimates after omitting each study individually, to determine the effect of individual studies on the overall mean difference. If the data could not be pooled, then they were described. Funnel plots and the Begg’s rank correlation test were chosen to detect publication bias if the number of included studies exceeded 10.
The clinical recommendation of meta-analysis was assessed using GRADEprofiler, which is used to evaluate the methodologic quality of studies, the directness of evidence, the heterogeneity, the precision of effect estimates, and the risk of publication bias. The GRADE quality was recorded as high, moderate, low, and very low. Clinical recommendation was classified as strong or weak.
Results
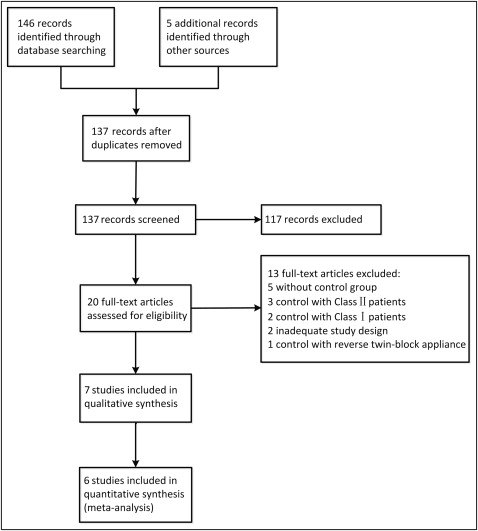
A total of 151 citations were identified through electronic and manual searching. Twenty studies were considered eligible, and full texts were retrieved after screening the titles and abstracts. Subsequently, 13 studies were excluded for specialized reasons. Finally, 7 studies were included in the qualitative synthesis, 6 were included in the meta-analysis, and 1 study was described ( Fig 1 ).
All 7 included studies were cohort studies, and all participants in the treatment group wore the FR-3 appliance for at least a year during their growth and development periods. Five studies reported short-term effects, and 1 study reported long-term (8 years) effects. One study reported both short-term (2-3 years) and long-term (9 years) effects. However, 2 studies did not report the frequency of wearing the appliance. For the control group without treatment of the Class III malocclusion, 6 studies simultaneously compared participants with the treatment group; however, the authors of the other study chose a controlled sample from a published study ( Table II ).
| Study | Levin (2008) | Falck (2007) | Kalavritinos (2005) | Baik (2004) | Waheed-Ul-Hameed (2002) | Sonmez (1996) | Mustafa (1994) |
|---|---|---|---|---|---|---|---|
| FR-3 group (n) | 32 (15 M, 17 F) | 56 (20 M, 36 F) | 14 (7 M, 7 F) | 30 (13 M, 17 F) | 10 (5 M, 5 F) | 20 (10 M, 10 F) | 20 (10 M, 10 F) |
| Location of selection of Fränkel patients | Heinrich Braun Regional Hospital, Zwickau, Germany | Heinrich Braun Hospital, Zwickau, Germany | Department of Orthodontics, School of Dentistry, Thessaloniki, Greece | Yonsei University Dental Hospital, Seoul, Korea | Orthodontic clinic, Lahore, Pakistan | Department of Orthodontics, University of Istanbul, Turkey | Faculty of Dentistry, University of Istanbul, Turkey |
| Initial mean age (y) | 7 | 7.6 | 9.7 | 8 | 8.7 | 9.5 | 9.5 |
| Inclusion criteria | Anterior crossbite or edge-to-edge incisor relationship, with a Wits appraisal of −2 mm or more | Angle Class III molar relationship and overjet of <0 mm for all incisors | Angle Class III molar relationship, overjet of ≤0 mm for all incisors | Mild or pseudo (functional) Class III malocclusion; good cooperation | Class III with maxillary deficiency, functional anterior crossbite, no anterior open bite | Only anterior crossbite | Could move the mandible backward and bite the anterior teeth in an edge-to-edge position |
| Frequency of appliance wear | Only daytime until the third month, then full-time for 2-3 years | Full-time for 1-2 years, then while sleeping and 4-5 h during the day for another 2-3 years | 14-16 hours per day | At least 14 hours per day | Not specified | Not specified | Full time |
| Mean period of treatment (y) | Short term: 2-3 Long-term: 9 |
8.2 | 2.4 | 1.3 | 1 | 1.9 | 1.9 |
| Numbers in untreated control group | Short term: 32 (15 M,17 F) Long term: 26 (13 M, 13 F) |
15 (7 M, 8 F) | 15 (8 M, 7 F) | 20 (10 M, 10 F) | 10 (5 M, 5 F) | 19 (9 M, 10 F) | 20 (10 M, 10 F) |
| Location of selection of untreated controls | University of Florence, Italy, and University of Michigan, Ann Arbor | Department of Orthodontics, Heinrich Braun Hospital, Zwickau, Germany | Department of Orthodontics, School of Dentistry, Thessaloniki, Greece | Not specified | Orthodontic clinic, Lahore, Pakistan | Department of Orthodontics, University of Istanbul, Turkey | Not specified |
| Initial mean age (y) | 6.1 | 8 | 8.1 | 8.2 | 8.74 | 9.4 | 9.3 |
| Mean observation period (y) | Short term: 2-3 Long term: 9 |
8 | 6 | 1.5 | 1 | 1.8 | 1.8 |
The Newcastle-Ottawa scale, used for assessing the quality of cohort studies, is shown in Table III . The scores ranged from 6 to 8, indicating that these studies were high quality.
| Quality evaluation | Study | ||||||
|---|---|---|---|---|---|---|---|
| Waheed-Ul-Hameed (2002) | Kalavritinos (2005) | Levin (2008) | Sonmez (1996) | Baik (2004) | Falck (2007) | Mustafa (1994) | |
| Representativeness of the FR-3 group | * | * | * | * | * | * | * |
| Selection of the control group | * | * | * | ||||
| Ascertainment of FR-3 treatment group | * | * | * | * | * | * | * |
| Demonstration that outcome of interest was not present at start of study | * | * | * | * | * | * | * |
| Comparability of participants in FR-3 and control groups | ** | * | ** | ** | * | * | ** |
| Assessment of outcome with independent blinding | |||||||
| Adequacy of follow-up | * | * | * | * | * | * | * |
| Lost to follow-up acceptable (<10% and reported) | * | * | * | * | * | * | * |
| Total quality (score) | High (8) | High (6) | High (7) | High (8) | High (6) | High (6) | High (8) |
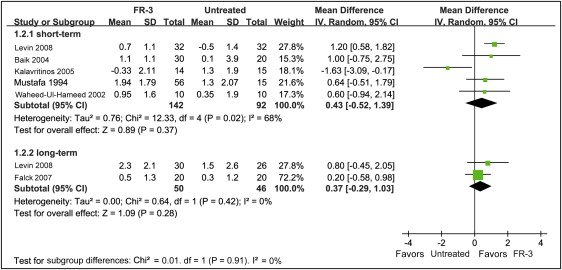
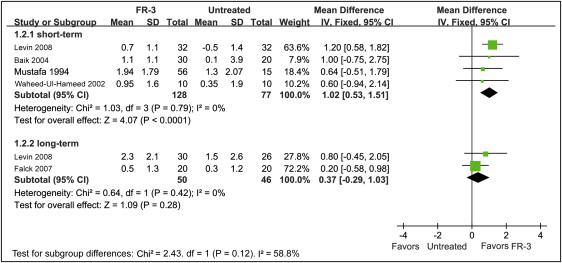
Five studies reported the short-term effects of SNA angle changes in 142 participants in the FR-3 groups and in 92 participants in the control groups. Two studies reported the long-term effects in 50 participants in the FR-3 groups and in 46 participants in the control groups. The meta-analysis showed that SNA changes did not differ between the 2 groups in the short term (mean difference, 0.43°; 95% CI, −0.52°-1.39°) and long term (mean difference, 0.37; 95% CI, −0.29°-1.03°) ( Fig 2 ). Moreover, sensitivity analysis was carried out by excluding 1 study with heterogeneity, showing that there was no difference in either the short term (mean difference, 1.02°; 95% CI, 0.53°-1.51°) or long term (mean difference, 0.37°; 95% CI, −0.29°-1.03) ( Fig 3 ).
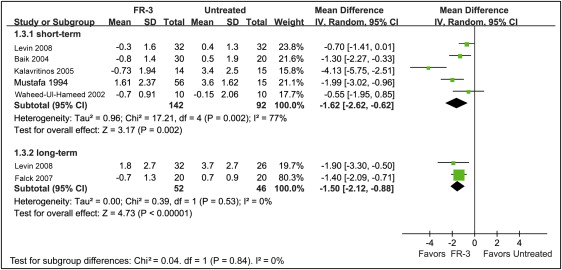
SNB angle changes were reported in 5 studies with 142 participants in the FR-3 groups and 92 in the control groups for the short-term effects, with significant differences observed between the groups (mean difference, −1.62°; 95% CI, −2.62° to −0.62°). In terms of long-term effects, 2 studies with 52 participants in the FR-3 groups and 46 participants in the control groups had significant differences (mean difference, −1.50°; 95% CI, −2.12° to −0.88°) ( Fig 4 ).
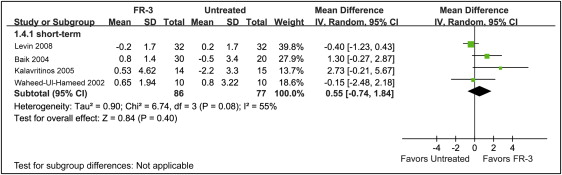
The mandibular plane angle (MPA) changes, measured by the Frankfort MPA in all included studies except one that mentioned only MPA, were reported in 4 studies. The short-term effects among the 86 participants in the FR-3 groups and the 77 participants in the control groups showed no difference (mean difference, 0.55°; 95% CI, −0.74°-1.84°) ( Fig 5 ).
Five studies reported ANB angle changes for the short-term effects among 142 participants in the FR-3 group and among 92 participants in the control groups. Two studies reported long-term effects among 52 participants in the FR-3 groups and among 46 participants in the control groups. The meta-analysis showed statistical differences in both the short term (mean difference, 1.84°; 95% CI, 0.96°-2.71°) and long term (mean difference, 0.07°; 95% CI, −3.17°-3.30°) ( Fig 6 ).


