Introduction
The aim of this crossover study was to assess perceptions and preferences for impression techniques in young orthodontic patients receiving alginate and 2 different digital impressions.
Methods
Thirty-eight subjects aged 10 to 17 years requiring impressions for orthodontic treatment were randomly allocated to 3 groups that differed in the order that an alginate impressions and 2 different intraoral scanning procedures were administered. After each procedure, the patients were asked to score their perceptions on a 5-point Likert scale for gag reflex, queasiness, difficulty to breathe, uncomfortable feeling, perception of the scanning time, state of anxiety, and use of a powder, and to select the preferred impression system. Chairside time and maximal mouth opening were also registered.
Results
More queasiness ( P = 0.00) and discomfort ( P = 0.02) during alginate impression taking of the maxilla were perceived compared with the scans with the CEREC Omnicam (Sirona Dental Systems, Bensheim, Germany). There were no significant differences in perceptions between the alginate impressions and the Lava C.O.S. (3M ESPE, St Paul, Minn) and between the 2 scanners. Chairside times for the alginate impressions (9.7 ± 1.8 minutes) and the CEREC Omnicam (10.7 ± 1.8 minutes) were significantly lower ( P <0.001) than for the Lava C.O.S. (17.8 ± 4.0 minutes). Digital impressions were favored by 51% of the subjects, whereas 29% chose alginate impressions, and 20% had no preference. Regardless of the significant differences in the registered times among the 3 impression-taking methods, the distributions of the Likert scores of time perception and maximal mouth opening were similar in all 3 groups.
Conclusions
Young orthodontic patients preferred the digital impression techniques over the alginate method, although alginate impressions required the shortest chairside time.
Highlights
- •
We assessed perceptions and preferences for impression techniques in orthodontic patients.
- •
We used alginate impressions and 2 intraoral scanners: Lava C.O.S. and CEREC Omnicam.
- •
Patients reported more queasiness and discomfort with alginate impressions.
- •
Patients preferred the CEREC Omnicam for impression taking.
- •
Alginate impressions required the shortest chairside time, and Lava C.O.S. the longest.
Plaster study models have been routinely used in orthodontics for diagnosis, appliance fabrication, and outcome evaluation. Recent advances in 3-dimensional imaging technology have enabled the transition to digital models for the sake of efficiency, simplicity of use, durability, and storage savings. In this context, orthodontic measurements on digital study models were found to be comparable with those made on plaster models, although the evidence was of variable quality. Digital models can be produced either indirectly by laser or cone-beam computed tomography scanning of plaster models or alginate impressions, or directly by scanning the dentition with an intraoral scanner. The latter option, which eliminates the need for physical impressions, has been recently subjected to intense investigation.
So far, most studies have focused on the accuracy of measurements made on digital models obtained from intraoral scanners and not on patient perceptions. Whereas impression taking with conventional alginate materials has been perceived by patients as a most unpleasant treatment experience, conflicting results were reported in adult and mixed-age patients on preferences for conventional or digital impression techniques.
Since the average orthodontic caseload comprises mainly children and adolescents, it would be interesting to investigate the preferred model acquisition method by patients of this age group. Therefore, the aim of this study was to assess youngsters’ perceptions and preferences for a full-arch impression-taking method with 2 intraoral scanners and 1 alginate impression.
Material and methods
A total of 38 consecutive subjects (16 boys, 22 girls; age range, 10-17 years; median, 12 years) seeking treatment at the Department of Orthodontics of the University Medical Center Groningen in The Netherlands in April 2015 and willing to participate in the study were recruited. Informed consent was received from all subjects, who were given information on the research purposes, expected duration of the study, and study protocols. Because the methods used for full-arch impression taking in the study were part of routine clinical procedures, the medical ethics review board ascertained that the study was not clinical research with test subjects as described in the Medical Research Involving Human Subjects Act; therefore, formal ethics approval was not necessary.
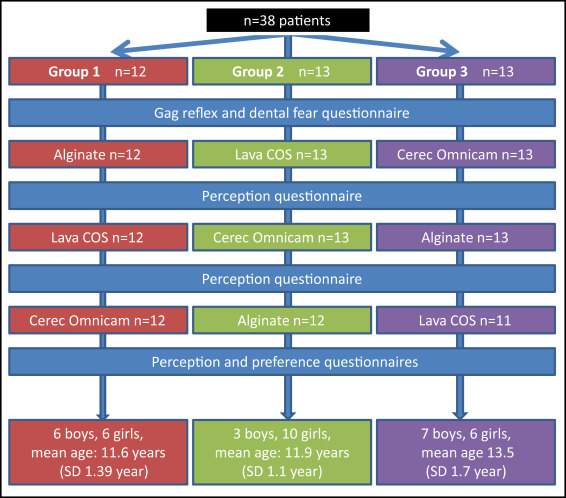
All patients had previously visited the Department of Orthodontics once for their first consultation and had been scheduled for diagnostic records. Further prerequisites for inclusion in the study were no previous experience with either alginate impressions or intraoral scanners, good physical and mental health, and no cleft lip or palate or other craniofacial anomalies. Subjects with a history of dental fear or hyperactive gag reflex—factors known to influence perceptions during the impression-taking process—were excluded. Study procedures and patient enrollment are shown in Figure 1 . Of the 38 patients, 3 were diagnosed with a low treatment need after the second impression appointment and discontinued their participation in the study. Therefore, only data regarding the first 2 impressions were used from these 3 participants.
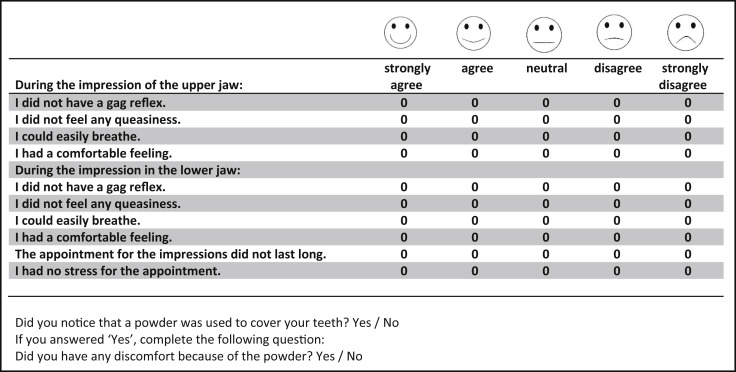
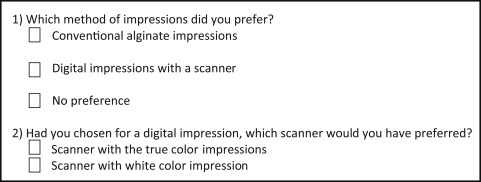
Four questionnaires were used for the purposes of the study. Two validated self-report instruments, the Dutch versions of the Children’s Fear Survey Schedule Dental Subscale and the Gagging Problem Assessment, were used to identify participants’ attitudes toward dental procedures. Both questionnaires were filled in by the patients at home and collected during the second visit. A third questionnaire (perception questionnaire) ( Fig 2 ) was developed after interviewing 5 children who had previously experienced the alginate impression process and 2 dental professionals (L.B. and a dental hygienist) with clinical experience with intraoral scanners. The perception questionnaire used in this study aimed to measure gag reflex, queasiness, difficulty to breathe, discomfort, time perception, anxiety, and the experience of the powder used for digital impressions. Accordingly, 10 questions with 5-point Likert scale responses ranging from “strongly agree” to “strongly disagree” and 2 closed yes-no questions were included. A fourth questionnaire (preference questionnaire) ( Fig 3 ) was introduced to determine the preferred impression method and specifically the intraoral scanner of choice if the participants favored digital impressions.
The participants were assigned to 3 groups according to the chronologic order of their first visit ( Fig 1 ). One alginate impression and 2 intraoral scans were obtained from each participant during 1 of the 3 appointments for diagnostic records, treatment plan discussions, and appliance placements with a 4-week interval between them. A balanced Latin square design was applied in the sequence of impression techniques to counterbalance any possible carryover and learning effects arising from the immediately preceding tested method. The intraoral scanners tested were the CEREC Omnicam (Sirona Dental Systems, Bensheim, Germany) and the Lava C.O.S. (3M ESPE, St Paul, Minn). The scanning protocol was applied according to the manufacturer’s prescription and as described previously. Alginate impressions were obtained with an irreversible hydrocolloid impression material (Cavex Impressional; Cavex Holland, Haarlem, The Netherlands) and standard plastic trays. All impression procedures were carried out by 1 examiner (L.B.) who had received 5 hours of training for each intraoral scanner before the study.
Maximal mouth opening, defined as the distance between the incisal edges of the maxillary and mandibular right central incisors, was registered before the first impression-taking session. The total time the patient needed to be seated for the impression was also registered as chairside time. Immediately after completing an impression at each session, the participants were asked to fill in the perception questionnaire. After the third impression session, the preference questionnaire was handed out and returned to the examiner (L.B.). Means and standard deviations of the Likert scores from the patients were calculated.
Statistical analysis
The 10-item Likert answers from the perception questionnaire and the time required for alginate impressions and the intraoral scanner were analyzed statistically with the nonparametric Friedman test with P <0.05 as the level for statistical significance. If the Friedman test was significant, Wilcoxon signed rank tests were performed with a Bonferroni corrected level for statistical significance of P <0.02. Correlations between chairside time, time perception, and maximal mouth opening were analyzed with the Spearman correlation test. All statistics were performed using PASW statistics (version 18.0; SPSS, Chicago, Ill).
Results
No patient had a gagging problem or dental fear. Because the differences between the groups were small, the perception questionnaire and the chairside time data of all participants were pooled. The perception questionnaire items including chairside time are described in Table I . There were no statistical differences in chairside time and perceptions between the same impression methods from the 3 groups, except for breathing difficulty in the mandible ( P = 0.03) and the perception of time ( P = 0.03) for the alginate impressions.
| Variable ∗ (Likert score) | LAV (n = 36) | CO (n = 38) | ALG (n = 37) | P value † | |||
|---|---|---|---|---|---|---|---|
| Mean (SD) | Median (IQR) | Mean (SD) | Median (IQR) | Mean (SD) | Median (IQR) | ||
| Gag reflex | |||||||
| Maxilla | 1.64 (1.29) | 1 (1) | 1.58 (1.15) | 1 (1) | 2.11 (1.39) | 1 (2) | 0.06 |
| Mandible | 1.61 (1.18) | 1 (1) | 1.58 (1.20) | 1 (1) | 1.57 (1.02) | 1 (1) | 0.95 |
| Queasiness | |||||||
| Maxilla | 1.56 (1.16) | 1 (0.75) | 1.32 (0.84) | 1 (0) | 1.92 (1.23) | 1 (1.5) | 0.00 ‡ |
| Mandible | 1.53 (0.91) | 1 (1) | 1.32 (0.84) | 1 (0) | 1.62 (1.06) | 1 (1) | 0.06 |
| Breathing difficulty | |||||||
| Maxilla | 1.42 (0.69) | 1 (1) | 1.39 (0.79) | 1 (1) | 1.49 (0.80) | 1 (1) | 0.62 |
| Mandible | 1.44 (0.65) | 1 (1) | 1.34 (0.67) | 1 (1) | 1.41 (0.64) | 1 (1) | 0.45 |
| Uncomfortable feeling | |||||||
| Maxilla | 1.89 (0.98) | 2 (2) | 1.55 (0.92) | 1 (1) | 2.03 (0.01) | 2 (1.5) | 0.02 ‡ |
| Mandible | 1.81 (1.01) | 1 (1.75) | 1.58 (0.98) | 1 (1) | 1.76 (0.90) | 2 (1) | 0.21 |
| Time perception | 2.03 (1.03) | 2 (2) | 1.79 (0.94) | 2 (1) | 1.76 (0.86) | 2 (1) | 0.72 |
| Anxiety experience | 2.03 (1.22) | 2 (2) | 1.74 (1.11) | 1 (1) | 1.92 (1.16) | 1 (2) | 0.26 |
| Chairside time (min) | 17.83 (3.99) | 18 (5.75) | 10.74 (1.81) | 10 (1.25) | 9.72 (1.81) | 9 (2.5) | 0.00 § |
∗ Variables are denoted as means (standard deviations) and medians (interquartile ranges).
† group differences were tested with the Friedman test with P <0.05 as the level of significance.
‡ post hoc test with the Wilcoxon signed rank test with P <0.02 as the level of significance gave difference between the ALG and CO.
§ post hoc test with Wilcoxon signed rank test with P <0.02 as the level of significance gave differences between the ALG and LAV and CO and LAV.
According to the perception questionnaire results ( Table I ), the participants had significantly more uncomfortable feelings ( P = 0.02) and more queasiness ( P = 0.00) in the maxilla with alginate impressions than with the CEREC Omnicam. All other perceptions were not significant from each other. The shortest chairside time was achieved with the alginate impressions (9.7 ± 1.8 m) followed by the CEREC Omnicam (10.7 ± 1.8 m). The Lava C.O.S. had the longest time (17.8 ± 4.0 m). The alginate impression and the CEREC Omnicam times were significantly shorter than the Lava C.O.S. time ( P <0.001). The difference between the alginate impressions and the CEREC Omnicam was marginally significant ( P <0.03).
Of the participants for the Lava C.O.S. and the CEREC Omnicam, 64% and 74%, respectively, confirmed they had noticed the powder during the scan. In these groups, 14% and 18% of the participants for the Lava C.O.S. and the CEREC Omnicam, respectively, indicated that they experienced discomfort related to the powder.
Answers given for the preference questionnaire are summarized in Table II . The intraoral scanner was favored by 51% of the subjects, followed by alginate impressions (29%), and no preference (20%). Of the participants who favored the intraoral scanner, 44% preferred the CEREC Omnicam, and 39% did not differentiate between the 2 intraoral scanners.


