Transconjunctival Approaches
Transconjunctival approaches expose the floor of the orbit and infraorbital rim. More recently, these approaches have been extended medially to expose the medial wall of the orbit.
The significant advantage of transconjunctival approaches is that the scar is hidden in the conjunctiva. If a canthotomy is performed in conjunction with the approach, the only visible scar is the lateral extension, which heals leaving an inconspicuous scar. Transconjunctival techniques are rapid because neither skin nor muscle dissection is necessary. These simple techniques, however, demand surgical precision in execution because the complication of improper transconjunctival technique (i.e., entropion) is much more difficult to correct than the sequela of an improper skin incision (i.e., ectropion).
Another advantage of the transconjunctival approach is that the medial extent of the incision can be expanded superiorly, behind the lacrimal drainage system, as high as the levator aponeurosis. This approach has been called the transcaruncular because of the incision’s relation to the caruncle. This approach can be useful when access to the medial orbital wall is required.
This chapter will discuss both approaches because they are often combined in practice.
TRANSCONJUNCTIVAL APPROACH TO THE INFRAORBITAL RIM AND FLOOR OF THE ORBIT
The traditional transconjunctival incision, also called the inferior fornix incision, is a popular approach for exposing the orbital floor and infraorbital rim. Both preseptal and retroseptal approaches have been described. These approaches vary in the relation of the orbital septum to the path of dissection (see Fig. 3.1). The retroseptal approach is more direct than the preseptal approach and is easier to perform. An additional advantage is that there is no dissection within the eyelid, which may help avoid scarring within it. The periorbital fat may be encountered during the retroseptal approach, but this is of little concern and causes no ill effects. A lateral canthotomy enhances exposure and is frequently employed. The retroseptal transconjunctival approach with a lateral canthotomy is described in this chapter.
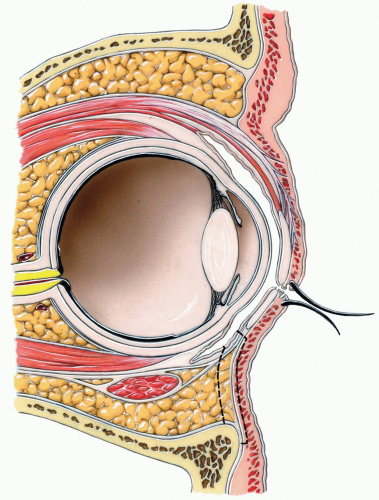
Figure 3.1 Sagittal section through orbit showing preseptal and retroseptal placement of incision.
|
SURGICAL ANATOMY
Lower Eyelid
In addition to the anatomy described in Chapter 2, for the lower eyelid approach, the transconjunctival approach to the infraorbital rim and orbital floor requires the comprehension of other points.
Lower Eyelid Retractors
During full downward gaze, the lower eyelid descends approximately 2 mm in conjunction with the movement of the globe itself. The inferior rectus muscle, which rotates the globe downward, simultaneously uses its fascial extension to retract the lower eyelid. This extension, which arises from the inferior rectus, contains
sympathetic-innervated muscle fibers and is commonly called the capsulopalpebral fascia (see Fig. 3.2). Incision of this fascial sheet is clinically inconsequential when closure of the incision is correctly achieved.
sympathetic-innervated muscle fibers and is commonly called the capsulopalpebral fascia (see Fig. 3.2). Incision of this fascial sheet is clinically inconsequential when closure of the incision is correctly achieved.
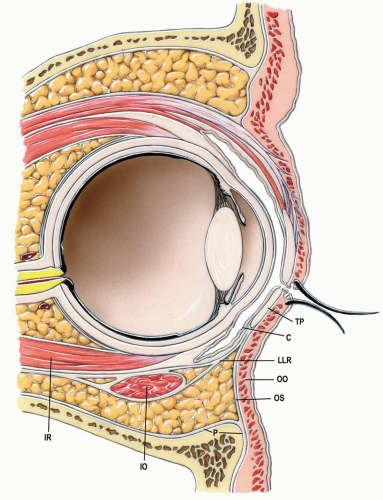
Figure 3.2 Sagittal section through orbit and globe. C, palpebral conjunctiva; IO, inferior oblique muscle; IR, inferior rectus muscle; LLR, lower lid retractors; OO, orbicularis oculi muscle; OS, orbital septum; P, periosteum/periorbita; TP, tarsal plate.
|
TECHNIQUE
▶ Step 1. Vasoconstriction
A vasoconstrictor is injected under the conjunctiva to aid in hemostasis (see Fig. 3.3A). Additional solution is infiltrated during the lateral canthotomy (Fig. 3.3B).
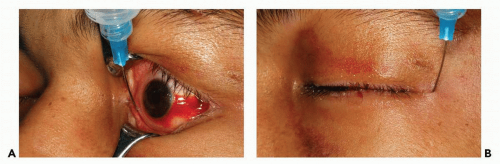
Figure 3.3 Photographs showing delivery of small amounts of local anesthetic with a vasoconstrictor, under the conjunctiva (A) and in the area of the lateral canthotomy (B).
|
▶ Step 2. Protection of the Globe
Because tarsorrhaphy is precluded with this approach, a corneal shield should be placed to protect the globe (see Fig. 3.4).
▶ Step 3. Traction Sutures in the Lower Eyelid
The lower eyelid is everted with fine forceps and two or three traction sutures are placed through the eyelid (Fig. 3.4). These sutures should be placed straight through the eyelid, from palpebral conjunctiva to skin, approximately 4 to 5 mm below the eyelid margin to ensure that the tarsal plate is included in the suture.
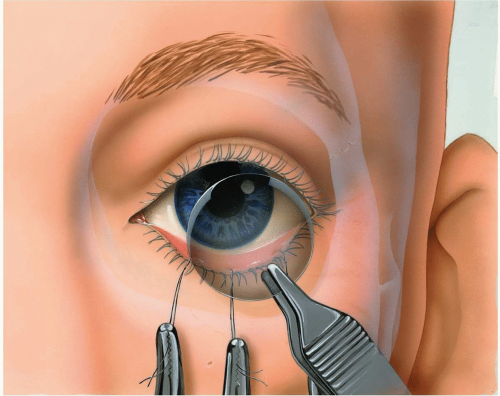
Figure 3.4 Placement of a corneal protector (shield). Two or three traction sutures placed through the lower eyelid assist in the placement of the shield and in subsequent surgery.
|
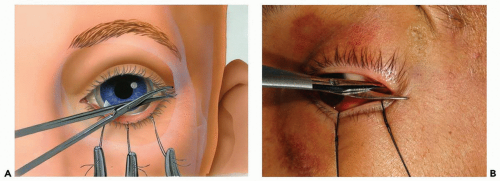
Figure 3.5 Illustration (A) and photograph (B) of initial incision for lateral canthotomy.
|
▶ Step 4. Lateral Canthotomy and Inferior Cantholysis
When a lateral canthotomy is indicated, the canthotomy is the initial incision. One tip of the pointed scissors is inserted within the palpebral fissure, extending laterally to the depth of the underlying lateral orbital rim (approximately 7 to 10 mm). The scissors are used to cut horizontally through the lateral palpebral fissure (see Fig. 3.5). The structures that are cut in the horizontal plane are the skin, orbicularis oculi muscle, orbital septum, lateral canthal tendon, and conjunctiva.
The traction sutures are used to evert the lower eyelid. The lower eyelid is still tethered to the lateral orbital rim by the inferior limb of the lateral canthal tendon (see Fig. 3.6A). This tethering functionally adapts the lower eyelid tightly to the globe (Fig. 3.6B). The tendon, which is easily visualized with eyelid retraction, is released with a sharp vertical cut. To perform the cantholysis, the scissors must be positioned with a vertical orientation (see Fig. 3.7). After cantholysis (see Fig. 3.8A), the lower eyelid is immediately freed from the lateral orbital rim (Fig. 3.8B), making the eversion more effective.
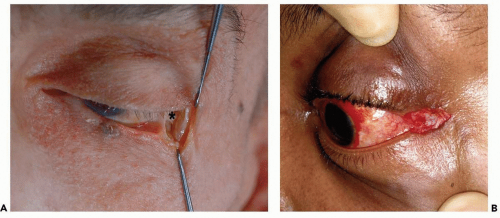
Figure 3.6 A: Anatomic dissection showing result after initial canthotomy illustrated in Figure 3.5. Note that the inferior limb of the lateral canthal tendon (*) is still attached to the lower tarsus, preventing mobilization. The lower eyelid is still tightly adapted to the eyeball (B).
|
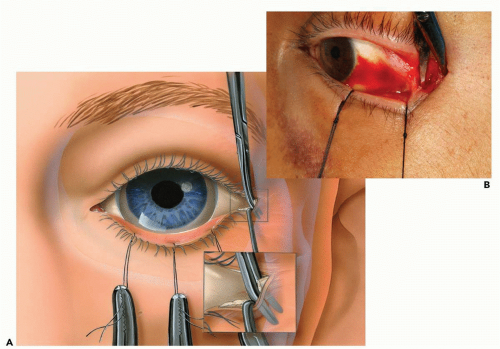
Figure 3.7 Illustration (A) and photograph (B) showing technique of inferior cantholysis.
|
▶ Step 5. Transconjunctival Incision
After the lower eyelid is everted, the position of the lower tarsal plate through the conjunctiva is noted. One of two following techniques can be used to incise the conjunctiva. In the first technique, blunt-tipped pointed scissors are used to dissect through the small incision in the conjunctiva made during the lateral canthotomy, inferiorly toward the infraorbital rim. Traction sutures are used to evert the lower eyelid during the dissection. The scissors are spread to clear a pocket posterior to the orbital septum, ending just posterior to the orbital rim (see Fig. 3.9).
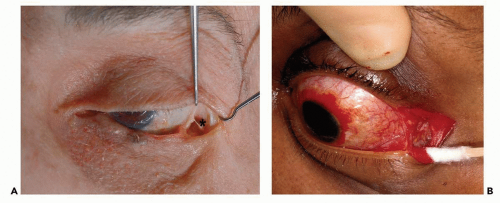
Figure 3.8 A: Anatomic dissection showing result after inferior cantholysis illustrated in Figure 3.7. Note that the inferior limb of the lateral canthal tendon (*) has been severed, allowing the lower eyelid great mobility (B).
|
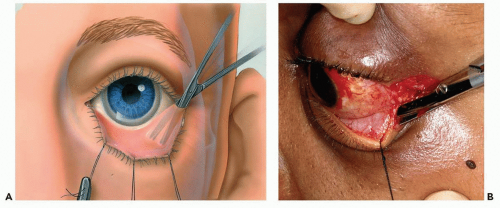
Figure 3.9 Illustration (A) and photograph (B) showing how the scissors are placed into the initial canthopexy incision to dissect in the subconjunctival plane. The dissection should be just below the tarsal plate and should extend no farther medially than the lacrimal punctum. Note how the traction sutures through the lower eyelid assist in this dissection.
|
Scissors are used to incise the conjunctiva and lower eyelid retractors midway between the inferior margin of the tarsal plate and the inferior conjunctival fornix (see Fig. 3.10). The incision can be extended as far medially as necessary for the surgery but must not violate the lacrimal sac.
The incised edge of the vestibular conjunctiva can be dissected free (see Fig. 3.11), providing a location for a traction suture to hold the corneal shield in place (see Fig. 3.12).
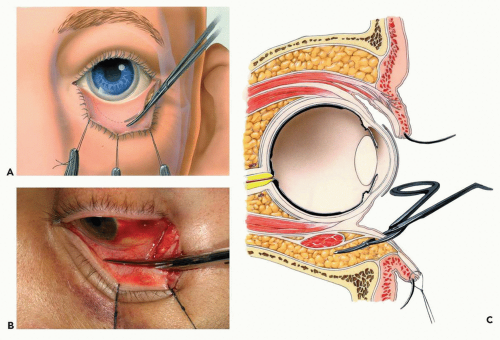
Figure 3.10 Illustration (A) and photograph (B) showing incision of the conjunctiva below the tarsal plate. C: Sagittal plane through the orbit and globe demonstrating the level and plane of incision. The conjunctiva and lower eyelid retractors are incised with scissors.
Stay updated, free dental videos. Join our Telegram channelVIDEdental - Online dental courses
 Get VIDEdental app for watching clinical videos
Get VIDEdental app for watching clinical videos

|