Although most oral and maxillofacial surgeons spend a great deal of time in the oral cavity and the associated maxillofacial region, the importance of understanding complete head and neck anatomy cannot be ignored. Trauma, superficial pathologic lesions, and infection are just a few of the reasons a maxillofacial surgeon requires a sound understanding of the anatomy of the neck. Malignant tumors in the maxillofacial region can spread through the lymphatic system to adjacent lymph nodes; therefore, a neck dissection is used to remove any suspicious lymph nodes. There are currently four classifications of neck dissection: radical, modified radical, selective, and extended. This chapter focuses on the surgical anatomy of the neck and its relevance for the practicing oral and maxillofacial surgeon. Although many of the key anatomic sites have been identified and established, room remains for growth in both our knowledge of and approaches to this complex area.
Lymphatics ( Figure 7-1 )
Before the importance of lymphatics in the organization of the neck is discussed, a brief overview of the main lymphatic duct, the thoracic duct, is imperative. The thoracic duct conveys lymph from the entire body back to the blood; however, the right side of the head and neck, right upper extremity, right lung, right side of the heart, and a portion of the liver all follow a different path. The path originates at the cisterna chili and enters the posterior mediastinum between the azygous vein and thoracic aorta. From there it courses to the left into the neck, anterior to the vertebral artery and vein, eventually entering the junction of the left subclavian and internal jugular veins.
Over the past three decades, advances have been made in our understanding of cervical fascial planes, lymphatic drainage patterns, preoperative staging, and extracapsular spread. Maximizing control and minimizing morbidity are concerns that have prompted modifications to the classic neck dissection. One modification, in particular, is the preservation of one or more nonlymphatic structures (e.g., spinal accessory nerve, internal jugular vein, and sternocleidomastoid muscle). Further observations have indicated that the pattern of nodal disease depends on the primary site. These findings led to another neck dissection modification, the selective preservation of one or several lymph node groups.
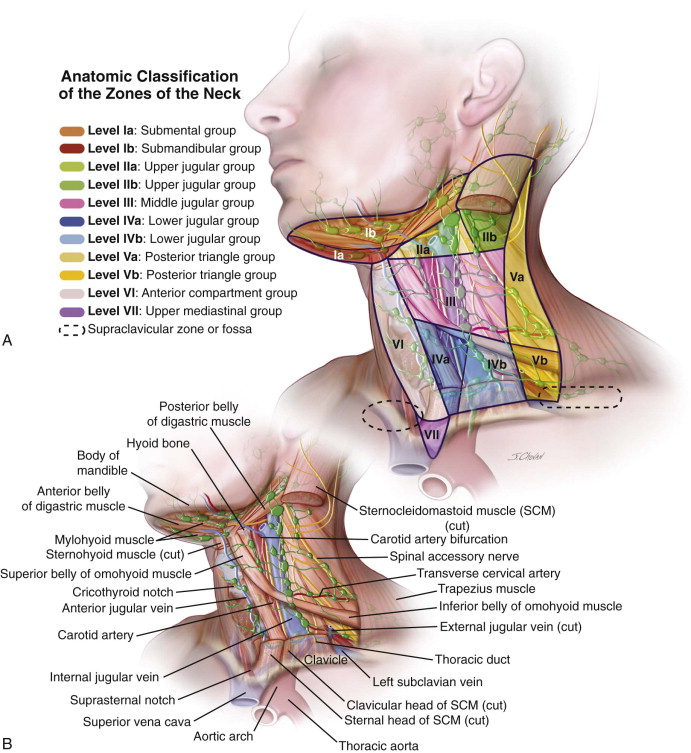
Memorial Sloan-Kettering Cancer Center developed the lymph node regional definitions that are most widely used today. There are approximately 600 lymph nodes in the body, 200 of which are located in the neck. It is important to note that lymphatic flow is well organized and moves in a predictable path in the cervical region. The neck is divided into six areas, or levels, ranging from submental and submandibular triangles toward the chest. These levels are identified by the Roman numerals I through VI. Oral cavity tumors have been found to metastasize to Levels I through III, whereas tumors of the lower neck (e.g., laryngeal cancer) tend to spread to lower levels (e.g., Level III or IV). Level VII, which represented the lymph node groups in the superior mediastinum, is no longer used. Lymph nodes in nonneck regions are referred to by the name of their specific nodal groups.
Level I
Level I includes the submental and submandibular triangles. This level is itself subdivided. Level Ia is the submental triangle, bounded by the anterior bellies of the digastric and the mylohyoid muscles; Level Ib is the triangle formed by the anterior and posterior bellies of the digastric and body of mandible.
Levels II, III, and IV
Levels II, III, and IV include nodes associated with the internal jugular vein (IJV), in addition to fibroadipose tissue located medial to the posterior border of the sternocleidomastoid (SCM) and lateral to the border of the sternohyoid.
Level II
Level II refers to the upper third nodes, including the upper jugular, jugulodigastric, and upper posterior cervical nodes. It is bounded by the digastric muscle superiorly and the hyoid bone (clinical landmark) or the carotid bifurcation (surgical landmark) inferiorly. Level IIa contains nodes in the region anterior to the spinal accessory nerve, whereas Level IIb contains those posterior to the nerve.
Level III
Level III includes the middle third jugular nodes, extending from the carotid bifurcation superiorly to the cricothyroid notch (clinical landmark), the inferior edge of the cricoid cartilage (radiologic landmark), or the omohyoid muscle (surgical landmark).
Level IV
Level IV contains the lower jugular nodes, extending from the omohyoid muscle superiorly to the clavicle inferiorly.
Level V
Level V refers to the posterior triangle group of lymph nodes located along the lower half of the spinal accessory nerve and the transverse cervical artery. The supraclavicular nodes are also included in this group. The posterior boundary is the anterior border of the trapezius muscle; the anterior boundary is the posterior border of the sternocleidomastoid muscle; and the inferior border is the clavicle.
Level VI
Level VI comprises the anterior compartment lymph nodes surrounding the midline visceral structures of the neck, extending from the level of the hyoid bone superiorly to the suprasternal notch inferiorly. On each side the lateral boundary is the medial border of the carotid sheath. Within this compartment are the perithyroidal lymph nodes, paratracheal lymph nodes, lymph nodes along the recurrent laryngeal nerves, and precricoid lymph nodes.
If all the nodes are removed (Levels I through V) and three structures are also removed (internal jugular vein, accessory nerve, and sternocleidomastoid muscle), a radical neck dissection has been performed. (The term radical is misleading; it simply refers to the fact that a complete neck dissection has been performed.) This procedure is indicated only if tumor spread to the neck is rather extensive. If the nodes from Levels I through V are removed and one of the three structures is preserved, the procedure is called a modified radical neck dissection. If the operation does not involve all five levels, it is called a selective neck dissection.
Anatomic Triangles of the Neck ( Figure 7-2 )
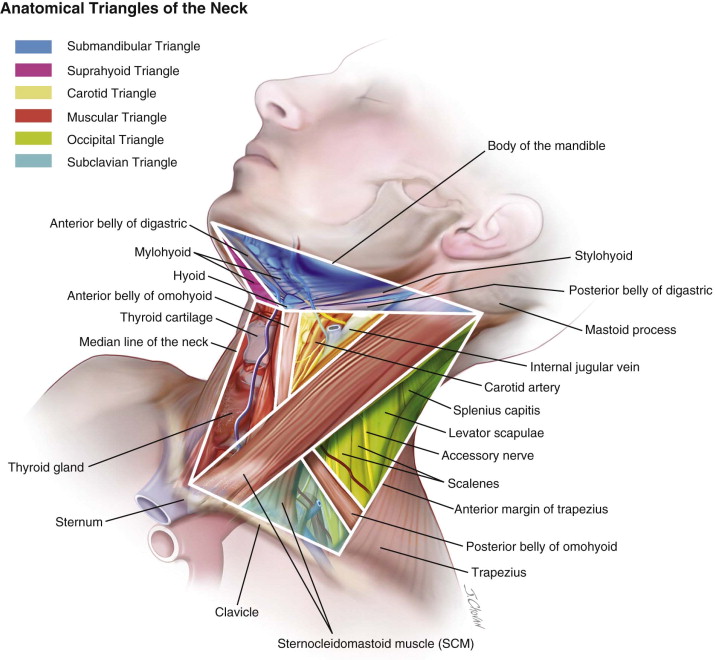
The side of the neck presents a somewhat quadrilateral outline limited by the lower border of the body of the mandible from above, an imaginary line extending from the angle of the mandible to the mastoid process and the anterior margin of the trapezius posteriorly, by the upper border of the clavicle from below, and by the midline of the neck anteriorly. This space is subdivided into two large triangles by the sternocleidomastoid muscle, which passes obliquely across the neck, from the sternum and clavicle below, to the mastoid process and occipital bone above. The triangular space in front of this muscle is called the anterior triangle and that behind it, the posterior triangle.
Anterior Triangle
The anterior triangle is bounded in front by the midline of the neck and behind by the anterior margin of the sternocleidomastoid. Its base, which is directed upward, is formed by the lower border of the body of the mandible and a line extending from the angle of the mandible to the mastoid process; its apex is below, at the sternum. This space is subdivided into four smaller triangles by the digastric above and the superior belly of the omohyoid below. These smaller triangles are named the inferior carotid (muscular) triangle, the superior carotid (carotid) triangle, the submaxillary (digastric) triangle, and the suprahyoid triangle. The anterior triangle is covered by integument, superficial fascia, platysma, and deep fascia.
Inferior Carotid (Muscular) Triangle
The inferior carotid, or muscular, triangle is limited in the front by the median line of the neck from the hyoid bone to the sternum and behind by the anterior margin of the sternocleidomastoid. The upper border is the superior belly of the omohyoid. The deep fascia contains branches of the supraclavicular nerves. Beneath these superficial structures are the sternohyoid and sternothyroid muscles, which together with the sternocleidomastoid conceal the lower part of the common carotid artery. This vessel, along with the internal jugular vein and vagus nerve, is enclosed within its sheath. The vein lies laterally to the artery on the right side of the neck but overlaps it below on the left side; the nerve lies between the artery and vein on a plane posterior to both. In front of the sheath are a few descending filaments from the ansa hypoglossi, and behind the sheath are the inferior thyroid artery, the recurrent nerve, and the sympathetic trunk. On its medial side are the esophagus, trachea, thyroid gland, and lower part of the larynx. By cutting into the upper part of this space and slightly displacing the sternocleidomastoid, the surgeon may tie the common carotid artery below the omohyoid.
Superior Carotid (Carotid) Triangle
The superior carotid, or carotid, triangle is bounded from behind by the sternocleidomastoid, below by the superior belly of the omohyoid, and above by the stylohyoid and the posterior belly of the digastric. Within the deep fascia are branches of the facial and cutaneous cervical nerves. The floor of the superior carotid triangle is formed by parts of the thyrohyoid muscle, hyoglossus muscle, and the inferior and medial pharyngeal constrictor muscles. When dissected, this area contains the upper part of the common carotid artery, which bifurcates opposite the upper border of the thyroid cartilage into the external and internal carotid. These vessels are somewhat concealed from view by the anterior margin of the sternocleidomastoid, which overlaps them. The external and internal carotids lie side by side, and the external carotid is the more anterior of the two. The following branches of the external carotid are also met within this space: the superior thyroid, running forward and downward; the lingual, directly forward; the external maxillary, forward and upward; the occipital, backward; and the ascending pharyngeal, directly upward on the medial side of the internal carotid. The associated veins are the internal jugular, which lies on the lateral side of the common and internal carotid arteries, and veins corresponding to the above-mentioned branches of the external carotid (the superior thyroid and the lingual, common facial, ascending pharyngeal, and sometimes the occipital), all of which end in the internal jugular.
The nerves in this space should also be taken into consideration by the surgeon. In front of the sheath of the common carotid is the ramus descendens hypoglossi. The hypoglossal nerve crosses both the internal and external carotids above, curving around the origin of the occipital artery. Within the sheath, between the artery and vein and behind both, is the vagus nerve; behind the sheath is the sympathetic trunk. On the lateral sides of the vessels, the accessory nerve runs for a short distance before it pierces the sternocleidomastoid; on the medial side of the external carotid, just below the hyoid bone, the internal branch of the superior laryngeal nerve is found. More inferior is the external branch of the same nerve. The upper portion of the larynx and lower portion of the pharynx are also found in the front part of this space.
Submaxillary (Digastric) Triangle
The submaxillary, or digastric, triangle corresponds to the region of the neck immediately beneath the body of the mandible. It is bounded above by the lower border of the body of the mandible and a line drawn from its angle to the mastoid process, and below by the posterior belly of the digastric and the stylohyoid. It is bordered in front by the anterior belly of the digastric. Within the deep fascia are branches of the facial nerve and ascending filaments of the cutaneous cervical nerve. The floor consists of the following muscles: mylohyoid, hyoglossus, and superior constrictor pharyngeal muscles; it is divided into an anterior and a posterior part by the stylomandibular ligament. The anterior part contains the submaxillary gland, superficial to which is the anterior facial vein; embedded in the gland is the external maxillary artery and its glandular branches. Beneath the gland, on the surface of the mylohyoid, are the submental artery and the mylohyoid artery and nerve. The posterior part of this triangle contains the external carotid artery, ascending deeply in the substance of the parotid gland; this vessel lies in front of and superficial to the internal carotid; it is crossed by the facial nerve and, during its course, gives off the posterior auricular, superficial temporal, and internal maxillary branches. More deeply are the internal carotid, the internal jugular vein, and the vagus nerve. These structures are separated from the external carotid by the styloglossus and stylopharyngeus muscles and the glossopharyngeal nerve.
Suprahyoid Triangle
The suprahyoid triangle is limited from behind by the anterior belly of the digastric, in front of the midline of the neck between the mandible and the hyoid bone, and below by the body of the hyoid bone. The mylohyoid muscle helps to form the floor. It contains one or two lymph glands and some small veins, which unite to form the anterior jugular vein.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


