New technological advances have helped the orthodontic profession progress in traditional and surgical methods of treatment. The profession has seen transitions from traditional braces to self-ligating brackets, lingual braces, removable aligners, and more advanced technology, which have helped to address concerns that include but are not limited to better diagnostics, anchorage control, length of treatment, and esthetics. An increase in the number of adult patients seeking orthodontic treatment and the need for a timely efficient care will continue to drive technology and the use of cone beam computed tomography, miniscrews, piezocision, distraction osteogenesis, and bioengineering.
Technology boldly tells step aside, lead, or follow. Orthodontics has taken a lead driven by the increasing numbers of adult population seeking care that is esthetic, efficient, and at a reasonable cost.
Most of the recently introduced technologies to current orthodontic therapy for both children and adults are geared toward reduced orthodontic time, minimal postoperative pain, and enhanced periodontium.
Self-ligating brackets
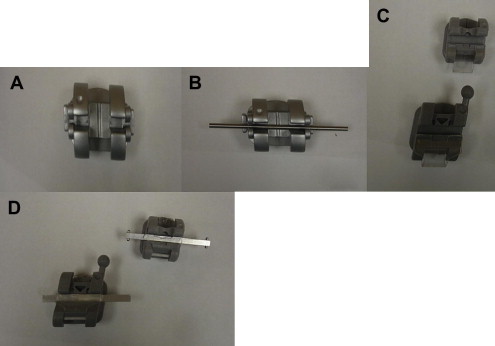
These are 4-walled rectangular brackets that contain a large lumen and are passively ligated with extremely low-force archwires with specific expanded arch forms used in a sequential series during treatment. The aim of self-ligation is to stay within the lowest force necessary at every phase of treatment. This helps to elicit optimum tooth movement through enhanced physiologic response of the periodontal ligament and surrounding supportive hard and soft histologic structures. Examples of self-ligation systems are Damon (Ormco Corporation, Glendora, CA, USA), Speed (Stride Industries, ON, Canada), SmartClip by 3M Unitek (Monrovia, CA, USA) ( Fig. 1 ). When self-ligating brackets have a wire that pulls through them, they produce less friction than conventional brackets. Questions that should be answered by this system are
-
Does this low friction lead to a reduced treatment time and faster tooth movement?
-
Do self-ligating appliances save chair time compared with elastomeric ligation, and are they more hygienic?
According to Hamilton and colleagues, the overall treatment time is no different between self-ligating brackets and conventional preadjusted appliances. However, further prospective studies are needed to prove the effectiveness of the self-ligation system in treatment time. Turpin points out that in vivo studies would be a better measure of self-ligation appliance than current in vitro studies. However, the results of in vitro studies have provided information that could remain useful as long as they are considered with care. Turnbull and Birnie showed that self-ligation is twice as fast to change archwires than conventional twin brackets and Alastik (3M Unitek, Monrovia, CA, USA), saving as much as 3 seconds per bracket and, therefore, reduces chair time. In addition, there is less need for chairside assistance, which can also save valuable time and reduce cost. A more recent report by Ong and colleagues has shown that self-ligating brackets are no more efficient than conventional ligated brackets in anterior alignment or passive extraction space closure during the first 20 weeks of treatment in extraction cases.
A study by Pellegrini and colleagues demonstrated that self-ligating appliances (brackets) promote less retention of bacteria, including streptococci, when compared with conventional appliances that use elastomeric ligatures. Concerning the periodontal status of mandibular anterior teeth in patients with conventional versus self-ligating brackets, a study by Pandis and colleagues showed that the self-ligating brackets had no advantage over the conventional brackets with respect to the status of the periodontal tissues of the mandibular anterior teeth.
Lingual orthodontics
This concept was initiated after Fujita and Kurz developed lingual brackets in the 1970s and 1980s. Not all patients are candidates for lingual orthodontic techniques, and this is especially true for patients with expected low discomfort tolerance. However, the development of indirect bonding techniques, the accuracy of bracket placement, the new metal alloys for archwires, and the wire bending methods simplified with the concept of the straight wire technique have contributed significantly to the reduction of patient discomfort and improved cooperation. In treatment with lingual orthodontics, patients should be carefully selected and diagnosed because some are more amenable than others. In patient selection, Echarri categorizes favorable cases based on the following: Class I skeletal pattern, mesocephalic or mild brachycephalic, patient ability to open the mouth adequately and extend the neck, mild incisor crowding with anterior deep bite, long uniform lingual tooth surface with no restoration on it, good gingival and periodontal health, as well as the patient’s keen compliance. Diagnostic considerations for lingual orthodontics should take into account esthetic factors; good periodontal and gingival health; dental considerations emphasizing on crowns, bridges, and restorations that are unfavorable; dentoalveolar discrepancy; vertical considerations; anteroposterior discrepancy; and preprosthetic cases.
Lingual orthodontics has developed, and its future depends on 3 important issues: (1) advances in technology related to appliance design and laboratory protocols, (2) increasing the adult population seeking orthodontic treatment and the patient-driven demand for more esthetic acceptable appliances, and (3) a change in public and professional attitudes to lingual orthodontics in a more acceptable way.
Lingual orthodontics
This concept was initiated after Fujita and Kurz developed lingual brackets in the 1970s and 1980s. Not all patients are candidates for lingual orthodontic techniques, and this is especially true for patients with expected low discomfort tolerance. However, the development of indirect bonding techniques, the accuracy of bracket placement, the new metal alloys for archwires, and the wire bending methods simplified with the concept of the straight wire technique have contributed significantly to the reduction of patient discomfort and improved cooperation. In treatment with lingual orthodontics, patients should be carefully selected and diagnosed because some are more amenable than others. In patient selection, Echarri categorizes favorable cases based on the following: Class I skeletal pattern, mesocephalic or mild brachycephalic, patient ability to open the mouth adequately and extend the neck, mild incisor crowding with anterior deep bite, long uniform lingual tooth surface with no restoration on it, good gingival and periodontal health, as well as the patient’s keen compliance. Diagnostic considerations for lingual orthodontics should take into account esthetic factors; good periodontal and gingival health; dental considerations emphasizing on crowns, bridges, and restorations that are unfavorable; dentoalveolar discrepancy; vertical considerations; anteroposterior discrepancy; and preprosthetic cases.
Lingual orthodontics has developed, and its future depends on 3 important issues: (1) advances in technology related to appliance design and laboratory protocols, (2) increasing the adult population seeking orthodontic treatment and the patient-driven demand for more esthetic acceptable appliances, and (3) a change in public and professional attitudes to lingual orthodontics in a more acceptable way.
Invisalign
Invisalign, first introduced by Align Technology, Inc (Santa Clara, CA, USA) in 1997, is a technique that uses a series of customized transparent, removable aligners, which are designed and created using advanced computer technology, to orthodontically straighten teeth. A high-quality set of pretreatment records, including photographs and radiographs, as well as polyvinyl siloxane impressions and a bite registration are taken and sent to Align Technology. These models are then digitized and are made available online in a 3-dimensional (3D) format so that the orthodontist can formulate a virtual prospective treatment plan using Align Technology’s software known as ClinCheck. This software allows the orthodontist to see a 3D representation of their treatment plan. Aligners are made and delivered to the orthodontist; on average, 20 to 30 aligners per arch are needed, with each set being replaced every 2 weeks. On average, case completion requires 12 months.
Align Technology has made great advances in the Invisalign product since its inception. In addition to Invisalign Full, its foundation product, there are several other customizable options available now. Invisalign Express is a shorter-duration product that is ideal for treating minor crowding cases and for preparing the mouth for restorative dentistry. Invisalign Teen addresses the unique considerations of treating adolescent patients, including compliance issues, as well as growth and development concerns. Invisalign Assist, the company’s customer service division, provides practitioners with product support to closely monitor the progress of cases, an ideal option for novice Invisalign users and for treating esthesis-centered cases.
Invisalign also has developed various attachments, which have addressed some of the concerns voiced about the product in the past, including extrusion attachments that allow for more controlled and predictable extrusions of the upper and lower anteriors. Rotation attachments now allow for improved rotation of upper and lower canines, and velocity attachments produce more controlled movements of both the crown and root. Power ridges allow for optimal lingual root torque on upper incisors, without having to bond attachments. Improvements in the ClinCheck software allow for interproximal reduction to be completed in the later stages of treatment, when the teeth are more aligned and thus are easier to access.
There are many considerations to be made when deciding whether to use Invisalign or conventional braces; however, with the continued improvements seen with Invisalign technology, it has become a feasible and common treatment option.
SureSmile
SureSmile, a product of OraMetrix (Richardson, TX, USA), is an orthodontic digital system that uses 3D imaging technology and computer software to facilitate diagnosis, treatment planning, and fabrication of customized orthodontic appliances. Brackets are first bonded to the teeth as with conventional braces and are leveled with a straight wire.
A 3D image is then created with brackets in place 3 to 6 months later using the OraScanner, a handheld light-based imaging device, which takes pictures of all surfaces of the teeth. Cone beam computed tomography (CBCT) can be used alongside the OraScanner for an even more accurate representation of the orientation of the teeth, roots, and adjacent structures. The resulting images are viewed using the therapeutic model, SureSmile software, that allows the operator to view the dentition from various perspectives and to consider several treatment alternatives by moving the teeth and extracting the teeth, along with other options. Once the treatment plan has been formulated, the SureSmile Digital Lab sends a set-up model to the practitioner for approval before archwire customization begins. The SureSmile archwire is created using robotics that precisely shapes the wire according to the specifications outlined in the set-up model and as confirmed/approved by the orthodontist. Copper Ni-Ti (nickel-titanium) metal is used during the robotic customization process to create a shape memory alloy that permanently retains the wire-bending specifications.
The ability to diagnose, plan treatment, and simulate the results of various treatment options, along with the extreme precision produced in the robotic-driven archwire bending process, improves orthodontic treatment in several critical areas. The 3D models allow for detailed planning so that the teeth move the shortest distance to their target position, and the robotic wire bending greatly reduces errors that can be introduced to the archwire. In fact, a study evaluating the efficiency and effectiveness of SureSmile showed that the process results in a lower mean ABO OGS (American Board of Orthodontics Objective Grading System) score and reduced treatment time as compared with conventional braces. This technology improves the reproducibility, efficiency, and quality of orthodontic treatment.
Cone beam computed tomography
CBCT is an imaging modality originally developed for angiography and later used in radiation therapy planning in mammography and later intraoperatively in otolaryngologic surgery. Although CBCT scanners have been around for more than 25 years, it was not until 2001 that the US Food and Drug Administration approved the first commercial system for oral and maxillofacial imaging. Some of the necessary technological advances that made the application of these scanners in the orthodontic office possible include:
- 1.
The development of compact, cost-efficient, flat-panel digital detectors
- 2.
The development of cost-efficient computers with the processing power to reconstruct the scans (a typical scan can range in size from 99–250 MB of data and include >500 slices )
- 3.
The fabrication of highly efficient radiograph tubes
- 4.
The development of machines that can scan limited field of views (FOVs).
The method of image data acquisition for a CBCT scanner involves a single rotation of an x-ray tube and a rectangular or round 2-dimensional detector. The fan beam CT scanners used in most hospital settings make use of a thin broad fan-shaped x-ray beam to acquire axial slices that are integrated yielding volumetric data ( Fig. 2 ).

The advantages of the CBCT include greater efficiency in radiograph use, lower cost of the equipment, and quicker data acquisition that affects patient comfort. Furthermore, using CBCT, measurements made in any plane are usually precise, given that the voxels (the 3D equivalent of a pixel) are isotropic.
Although CBCT has various uses in dentistry, some of its benefits in orthodontics include:
- •
A 3D rendering of the craniofacial structures without distortion or magnification. Cross-sectional views can be taken without the interference of other structures superimposed on them (for this same reason, certain landmarks on a lateral cephalometric projection may not be visible or difficult to locate based on definition, ie, location of porion)
- •
Detection of affected teeth, their axial inclination, and proximity to total structures/other teeth can be better visualized ( Fig. 3 )
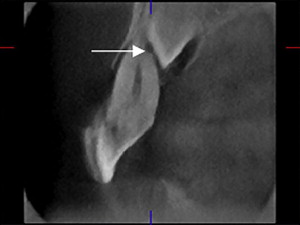
Fig. 3 An affected maxillary canine causing resorption of the root of the adjacent lateral incisor ( arrow ).( Adapted from Alqerban A, Jacobs R, Souza PC, et al. In-vitro comparison of 2 cone-beam computed tomography systems and panoramic imaging for detecting simulated canine impaction-induced external root resorption in maxillary lateral incisors. Am J Orthod Dentofacial Orthop 2009;136:764.e7; with permission.) - •
Measurement of the airway is much more accurate than with 2D lateral cephalography
- •
Treatment planning for orthodontic miniscrews is made simpler. Evaluations of root proximity, bone thickness, and adjacent vital structures can be performed
- •
Assisting in creating physical biomodels in the treatment of patients with craniofacial syndromes
- •
An improved ability to detect occult pathologic condition ( Fig. 4 ).



