There have been several exciting technological advances in extraction techniques and outpatient oral surgery within the last decade. A variety of new instruments and techniques are revolutionizing the fields of oral and maxillofacial surgery and dentistry. This article reviews the newer innovations in dentistry including the powered periotome, piezosurgery, the Physics Forceps, laser therapy, orthodontic techniques, and use of polyurethane foam.
There have been several exciting technological advances in extraction techniques and outpatient oral surgery within the last decade. A variety of new instruments and techniques are revolutionizing the fields of oral and maxillofacial surgery and dentistry. A powered periotome has been developed to atraumatically extract teeth. This instrument is particularly useful for immediate or delayed implant placement. In addition, a technique using implant drills has been developed to extract teeth in preparation for immediate implant placement. Piezosurgery is also being increasingly used for outpatient oral surgery techniques. The precise and effortless nature of piezosurgery has been used in the removal of certain third molars and in bone grafting. Moreover, the Physics Forceps has been created, which uses class 1 lever mechanics to extract teeth without having to use excessive force or squeezing motion. Lasers are also being used for a wide variety of outpatient procedures such as removal of impacted teeth and excision of oral lesions. Orthodontic techniques are also being used by some practitioners to help facilitate extraction of impacted teeth near the inferior alveolar nerve. The use of polyurethane foam to help close oral antral communications may offer a simple technique of handling this fairly common occurrence following dental extractions.
Powered periotome
The traditional means of extracting teeth often involving creation of a mucoperiosteal flap, elevation, and luxation with forceps often results in fracture or deformation of the dentoalveolar complex. This trauma could lead to ridge defects, making the placement of implants very difficult or even impossible in some cases. Also, elevation of the mucoperiosteum may compromise the periosteal blood supply to the alveolus, leading to loss of marginal alveolar bone even in relatively atraumatic extractions. In addition, if the adjacent teeth to the tooth to be extracted have extensive restorations or crown coverage, the powered periotome eliminates the need to elevate against and possibly damage these restorations.
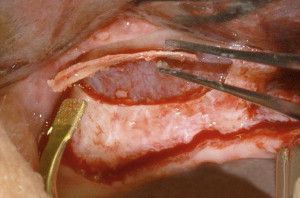
A powered periotome (Powertome 100S, WestPort Medical, Salem, OR) as shown in Fig. 1 has been developed that allows for the precise extraction of a tooth while producing minimal or no alveolar bone loss. This atraumatic means of dental extraction preserves bone and gingival architecture and gives the clinician the option of placing future or even immediate implants. The powered periotome functions by using the mechanisms of “wedging” and “severing” to aid in tooth extraction. As shown in Fig. 2 , these instruments are made of very thin metal blades that are gently wedged down the periodontal ligament space in a circumferential manner. This device severs Sharpey’s fibers, which function to secure the tooth within the alveolar socket. After most of the Sharpey fibers have been severed from the root surface, gentle rotational movement with minimal lateral pressure will facilitate tooth removal.

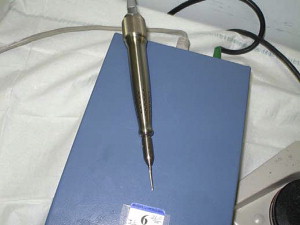
A powered periotome is an electric unit that contains a handpiece with a periotome that is activated by a foot control. This device allows precise control over the quantity of force that the periotome tip exerts and the distance it travels into the periodontal ligament space. The instrument has a microprocessor-run actuator that eliminates uncertainty while extracting a tooth. As shown in Fig. 1 , this device comes with a controller box that can be adjusted to 10 different power settings. In addition, the use of the Powertome 100S system frequently allows flapless removal of teeth, decreasing postoperative pain and discomfort while maintaining the periosteal blood supply to the alveolus. The automated powered periotome system also reduces concern for fracture of lingual bone or buccal plate during difficult extractions. The use of a standard periotome is a much more tedious process and can actually cause unneeded discomfort for the patient, especially if a mallet is also needed to separate the tooth from bone.
When using the powered periotome, the authors have found that starting interproximally seems to work most efficiently because of the thickness of the interproximal bone. It is important to keep the blade parallel along the long axis of the tooth being removed. The blade should follow the tooth anatomy circumferentially in an apical direction in 2- to 3-mm increments. When extracting a multirooted tooth, the authors have found it most efficient to section the tooth and treat each sectioned root as a single-rooted tooth. This instrument has a very small learning curve, and has been used by both general practice and oral surgery residents for tooth extractions. Photographs from a clinical case taken in the authors’ clinic are shown in Figs. 3 to 6 .




Clinical use by investigators has shown that this product works efficiently to deliver an intact extraction socket with excellent patient acceptance, while at the same time adding little to no additional time as compared with other surgical extraction techniques. Regardless of whether an implant is placed immediately after extraction or if the socket is grafted in preparation for future implant placement, the preservation of alveolar bone allows for more esthetic and functional implant restorations. Millimeters do count when it comes to implants.
Using implant drills for extractions prior to immediate implant placement
The placement of implants for the restoration of lost dentition is becoming commonplace as a treatment option. Immediate implants are in high demand, due to the rising requests for prompt restoration. As mentioned earlier, the key to placing successful and long-lasting immediate implants is preserving as much bone as possible by extracting the tooth as atraumatically as possible. Yalcin and colleagues presented a novel, minimally invasive technique to aid in the extraction of the tooth. To avoid traumatizing the surrounding bone during elevation, implant drills were placed in the root canals to thin the root walls giving way to extraction with the application of much less force, thereby decreasing the chance of traumatizing the thin buccal bone. The thinning of the walls of the roots prior to elevation made it easier to remove the teeth and minimized the risk of damaging the thin labial wall, especially in root fractures where the fracture line was deep in the socket in immediate implant cases. The investigators were able to successfully complete this procedure with no incisions and without having to reflect any flaps. There was no damage to the labial plate in all of their presented cases. The successful use of this technique may decrease the need for regenerative techniques that could result in graft-related or membrane-related complications.
Using implant drills for extractions prior to immediate implant placement
The placement of implants for the restoration of lost dentition is becoming commonplace as a treatment option. Immediate implants are in high demand, due to the rising requests for prompt restoration. As mentioned earlier, the key to placing successful and long-lasting immediate implants is preserving as much bone as possible by extracting the tooth as atraumatically as possible. Yalcin and colleagues presented a novel, minimally invasive technique to aid in the extraction of the tooth. To avoid traumatizing the surrounding bone during elevation, implant drills were placed in the root canals to thin the root walls giving way to extraction with the application of much less force, thereby decreasing the chance of traumatizing the thin buccal bone. The thinning of the walls of the roots prior to elevation made it easier to remove the teeth and minimized the risk of damaging the thin labial wall, especially in root fractures where the fracture line was deep in the socket in immediate implant cases. The investigators were able to successfully complete this procedure with no incisions and without having to reflect any flaps. There was no damage to the labial plate in all of their presented cases. The successful use of this technique may decrease the need for regenerative techniques that could result in graft-related or membrane-related complications.
Piezosurgery
Piezosurgery was introduced in 1988 and has been improved upon since then. Piezosurgery is an innovative bone surgery technique that produces a modulated ultrasonic frequency of 24 to 29 kHz, and a microvibration amplitude between 60 and 200 mm/s. The amplitude of the vibrations created allows a very clean and precise surgical cut. Piezosurgery is very effective in the creation of osteotomies because it works selectively, without harming soft tissues such as nerves and blood vessels even with accidental contact with the cutting tip. Piezosurgery thus has a tremendous advantage over the use of burrs and surgical saws that have the potential to cause destruction to soft tissue. When compared with oscillating microsaws, the oscillation of the piezosurgery scalpel tip is very small and therefore able to perform more precise and safe ostetomies. Traditional burrs and microsaws do not distinguish hard and soft tissue. Piezosurgery also gives the operator a clearer field of vision by producing a very restricted bloody region. In addition, as shown in Figs. 7 and 8 , the surgical control of the device is effortless compared with rotational burrs or oscillating saws because there is no need for an additional force to oppose rotation or oscillation of the instrument


In a recent study by Sortino and colleagues, rotary and piezoelectric techniques were compared in terms of postoperative outcome. The average time of surgery was 25.83% higher with the piezoelectric technique in comparison with the rotary technique. Despite the longer time of the procedure, the investigators also noted that the piezoelectric osteotomy reduced postoperative facial swelling and trismus.
The ability of piezosurgery to allow precise and selective cuts makes this a useful technique when performing surgery close to the inferior alveolar neurovascular bundle and/or the roots of adjacent teeth. The removal of the body of the mandible lateral cortical bone with piezoelectric instrumentation allows adequate access to the surgical area, excellent visibility, minimal bone loss, and precise cutting ability, and allows the protection of the inferior alveolar nerve (IAN) by sparing the soft tissue when osteotomy is performed blind. Because the bone-cutting ability is so precise with minimal bone loss, investigators using this technique have found it easy to readapt the bone windows to their former location and fixate them. Similarly, piezosurgery can be used to perform sinus lifts in a very precise and controlled manner, as shown in Figs. 9 and 10 .