Introduction
Self-ligating brackets have been gaining popularity over the past several decades. Various advantages for these systems have been claimed. The purposes of this systematic review were to identify and review the orthodontic literature with regard to the efficiency, effectiveness, and stability of treatment with self-ligating brackets compared with conventional brackets.
Methods
An electronic search in 4 data bases was performed from 1966 to 2009, with supplemental hand searching of the references of retrieved articles. Quality assessment of the included articles was performed. Data were extracted by using custom forms, and weighted mean differences were calculated.
Results
Sixteen studies met the inclusion criteria, including 2 randomized controlled trials with low risk of bias, 10 cohort studies with moderate risk of bias, and 4 cross-sectional studies with moderate to high risk of bias. Self-ligation appears to have a significant advantage with regard to chair time, based on several cross-sectional studies. Analyses also showed a small, but statistically significant, difference in mandibular incisor proclination (1.5° less in self-ligating systems). No other differences in treatment time and occlusal characteristics after treatment were found between the 2 systems. No studies on long-term stability of treatment were identified.
Conclusions
Despite claims about the advantages of self-ligating brackets, evidence is generally lacking. Shortened chair time and slightly less incisor proclination appear to be the only significant advantages of self-ligating systems over conventional systems that are supported by the current evidence.
Self-ligating brackets have been gaining popularity in recent years. However, self-ligation is not a new concept. The first self-ligating bracket, the Russell attachment, was introduced by Stolzenberg in the early 1930s. Perhaps because of skepticism in the orthodontic society at that time, or the lack of promotion, it did not gain much popularity. During the past several decades, interest in self-ligating brackets has been rekindled, with the introduction of various types of new self-ligating systems. These self-ligating brackets have been touted to possess many advantages over conventional edgewise brackets.
Self-ligating brackets can be divided into 2 main categories, active and passive, according to their mechanisms of closure. Active self-ligating brackets have a spring clip that stores energy to press against the archwire for rotation and torque control. In-Ovation (GAC International, Central Islip, NY), SPEED (Strite Industries, Cambridge, Ontario, Canada), and Time (Adenta, Gilching/Munich, Germany) are examples of active self-ligating brackets. On the other hand, passive self-ligating brackets usually have a slide that can be closed which does not encroach on the slot lumen, thus exerting no active force on the archwire. Damon (Ormco, Glendora, Calif) and SmartClip (3M Unitek, Monvoria, Calif) are 2 popular brands of passive design, although the SmartClip’s appearance resembles conventional brackets and does not have a slide.
The claim of reduced friction with self-ligating brackets is often cited as a primary advantage over conventional brackets. This occurs because the usual steel or elastomeric ligatures are not necessary, and it is claimed that passive designs generate even less friction than active ones. With reduced friction and hence less force needed to produce tooth movement, self-ligating brackets are proposed to have the potential advantages of producing more physiologically harmonious tooth movement by not overpowering the musculature and interrupting the periodontal vascular supply. Therefore, more alveolar bone generation, greater amounts of expansion, less proclination of anterior teeth, and less need for extractions are claimed to be possible. Other claimed advantages include full and secure wire ligation, better sliding mechanics and possible anchorage conservation, decreased treatment time, longer treatment intervals with fewer appointments, chair time savings, less chair-side assistance and improved ergonomics, better infection control, less patient discomfort, and improved oral hygiene.
However, self-ligating brackets have some disadvantages, including higher cost, possible breakage of the clip or the slide, higher profile because of the complicated mechanical design, potentially more occlusal interferences and lip discomfort, and difficulty in finishing due to incomplete expression of the archwires.
Many in-vitro studies have investigated parameters such as frictional resistance and torque expression in self-ligating systems. Many have shown that less friction is generated with self-ligating brackets compared with conventional brackets in the laboratory, and, therefore, less force is required to produce tooth movement. However, the suitability of applying the results from in-vitro studies to clinical situations and the importance of friction in alignment, sliding mechanics, and total treatment time have not been fully addressed. Many case series, several cohort studies, and a few randomized controlled trials have addressed various parameters of self-ligating brackets. To date, no systematic review has synthesized evidence from these in-vivo clinical studies.
The a priori aim of this systematic review was to identify and review the orthodontic literature with regard to the efficiency (chair time, treatment time), effectiveness (occlusal indices, arch dimensions), and stability of treatment with self-ligating brackets compared with conventional brackets. If the data allowed, a meta-analysis would be performed.
Materials and methods
The following criteria were formulated a priori to select articles for inclusion in this review. The inclusion criteria were (1) clinical studies that compared self-ligating with conventional appliances regarding their efficiency, effectiveness, or stability; (2) all ages and sexes; and (3) all languages. The exclusion criteria were (1) in-vitro, ex-vivo, or animal studies; (2) studies with no comparison group; and (3) editorials, opinions, or philosophy articles with no subjects or analytical design.
Electronic data bases—PubMed, Web of Science, EMBASE, and Cochrane Library—from 1966 to the third week of May 2009 were searched with the assistance of a senior research librarian at the University of Washington Health Sciences Library. Search strategies and key words are shown in Appendix 1 . Titles and abstracts of potential articles for inclusion were examined by at least 2 reviewers (S.S.-H.C., J.-E.K., C.L.S.); the articles were included based on consensus agreement on the above criteria. Abstracts of articles with uncertain inclusion characteristics were examined, with the full article retrieved if necessary. Grey literature was considered, but ultimately only published peer-reviewed articles were included.
After compiling the list of studies to be included, 2 investigators (S.S.-H.C., J.-E.K., C.L.S.) read the articles and abstracted the data onto custom data-abstraction forms, which had been piloted on 2 studies of each type (cohort study and randomized controlled trial). The reference lists of the retrieved full articles were also hand searched. Some authors of relevant studies were contacted for additional information. All search and data abstraction were independently performed by at least 2 investigators (C.L.S., J.-E.K., S.S.-H.C., G.M.G.). When 2 reviewers disagreed, a third investigator was called in, and consensus was reached.
Independent quality assessment of the included studies was performed according to a modified Newcastle-Ottawa scale by 2 investigators (G.J.H., S.S.-H.C). In areas of disagreement, a third investigator (G.M.G.) was consulted, and consensus was achieved after discussion.
For randomized controlled trials, 5 criteria were used for assessment: (1) randomization described, (2) allocation concealment reported, (3) intention-to-treat analysis performed, (4) blinded assessment stated, and (5) a priori power calculation performed.
For cohort and cross-sectional studies, these criteria were used: (1) representative sample of adequate size, (2) well-matched samples, (3) adjustment for confounders in analyses, (4) blinded assessment stated, and (5) dropouts reported (for prospective studies only).
One point was given to each criterion if fulfilled. Half a point was granted if part of the criterion was met. Studies with less than 2 points were considered to be at high risk for bias; from 2 to less than 4 points, the risk for bias was considered moderate; and for 4 points and above, the risk of bias was considered low. All quality ratings have limitations, and our intention was to provide a relative scale to judge the quality of the studies, by using the parameters stated above.
Meta-analysis
A meta-analysis was performed to combine comparable results in each category by using Review Manager (version 5.0, Copenhagen: Nordic Cochrane Centre, Cochrane Collaboration, 2008). Heterogeneity was assessed among the included studies. Results with less heterogeneity (I 2 statistics <75%) were presented with a fixed-effects model, whereas results with I 2 >75% utilized a random-effects model. Weighted mean differences were used to construct forest plots of treatment time, occlusal index scores, and other continuous data. Odds ratios were used for dichotomous data. Publication bias was assessed with funnel plots, if possible.
Results
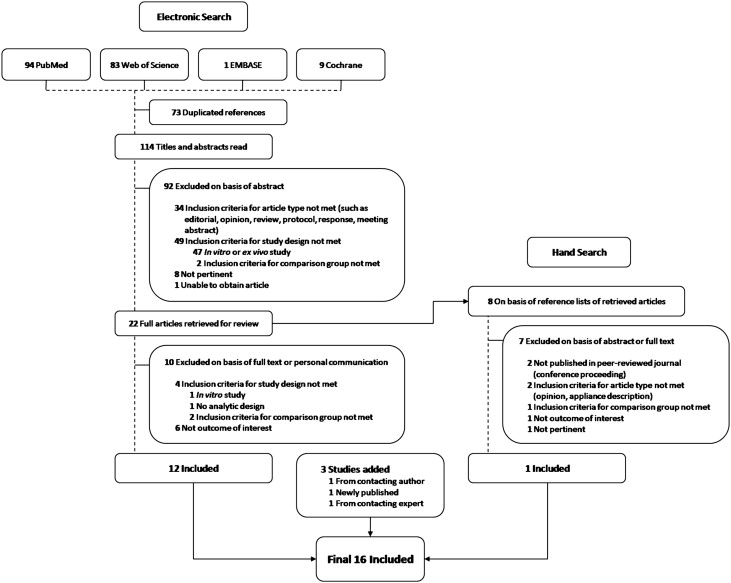
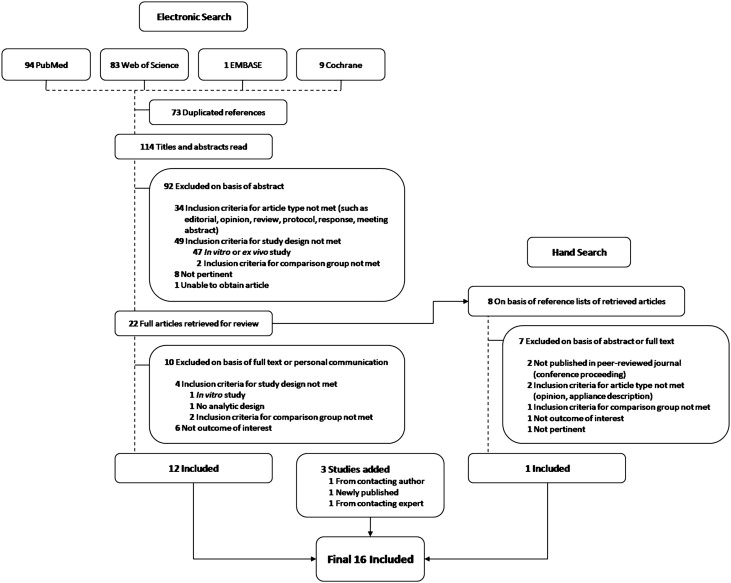
The electronic searches identified 114 titles and abstracts. From these, 22 full articles were retrieved for review. Ultimately, 16 articles met the inclusion criteria, including 1 article added from hand searching, 1 article added from contacting an author, 1 article published during this review, and another identified by contacting an expert in the field ( Fig 1 ). Characteristics of the excluded articles are listed in Appendix 2 .
The 16 studies included 2 randomized controlled trials, 10 cohort studies (7 prospective, 3 retrospective ), and 4 cross-sectional studies. All included articles were published in English, except for 1 in Chinese. Characteristics of the included studies are shown in the Table . Most samples comprised adolescent subjects.
| Author | Year | Design | Self-ligating group (number of patients) | Conventional group (number of patients) | Pretreatment mean age (y) |
Authors’ conclusions | Risk of bias |
|---|---|---|---|---|---|---|---|
| Berger and Byloff | 2001 | Cross-sectional | SPEED (20) (Strite Industries) Damon SL (20) (Ormco/”A” Company) Time (20) (Adenta) Twinlock (20) (Ormco/”A” Company) | Mini-twin (40) (Ormco/”A” Company) | Not reported | Total opening and closing time was significantly less for each of the 4 SL designs compared with conventional brackets; SPEED took the least average time and Damon SL the most. | High |
| Eberting et al | 2001 | Retrospective cohort | Damon SL (108) (SDS Ormco) | Type not specified (107) | Not reported | Patients treated with Damon SL had significantly lower treatment times, required significantly fewer appointments, and had significantly higher American Board of Orthodontics scores than those treated with conventionally ligated edgewise brackets. | Moderate |
| Fleming et al | 2009 | Randomized controlled trial | SmartClip (32) (3M Unitek) | Victory (33) (3M Unitek) | SmartClip: 15.9 Victory: 16.6 |
In nonextraction patients with mild mandibular incisor crowding, the SL system used was no more effective at relieving irregularity. Enhanced resolution of irregularity was positively correlated with pretreatment irregularity. | Low |
| Hamilton et al | 2008 | Retrospective cohort | In-Ovation (379) (GAC International) | Victory (383) (3M Unitek) | Not reported | Active SL brackets appear to offer no measurable advantages in treatment time, number of visits, and time spent in initial alignment over conventional preadjusted orthodontic brackets. The number of debonded brackets and other emergency visits were significantly higher in patients treated with active SL brackets. | Moderate |
| Harradine | 2001 | Retrospective cohort | Damon SL (30) (SDS Ormco) (study on speed of ligation: n = 50) (study on bracket complications: n = 25) |
Type not specified (30) (study on speed of ligation: n = 50) (study on bracket complications: n = 25) |
Not reported | Treatment times were 4 months shorter and required 4 fewer visits on average in the Damon group. Slide opening and closure were significantly faster than with conventional ligation. Both types of brackets produced good and equivalent reductions in occlusal irregularity. | Moderate |
| Jiang and Fu | 2008 | Prospective cohort | Damon3 (13) (SDS Ormco) (mandibular incisor torque: –1°) |
Conventional metal preadjusted brackets (13) (Shinya, China) (mandibular incisor torque: –1°) |
Damon3: 14.5 Conventional:15.3 |
In patients with crowding treated without extractions, there were overall increases in the proclination of the mandibular incisors and arch widths in both groups. Patients treated with Damon3 had greater intermolar width increases than those treated with conventional appliances. | High |
| Maijer and Smith | 1990 | Cross-sectional | Activa (14) (“A” Company) | Straight-wire brackets (14) (“A” Company) | Not reported | Reduced chair time was a significant advantage of SL brackets. The operator’s training made little difference in speed, at least with anterior brackets. | High |
| Miles | 2005 | Prospective cohort | SmartClip (29) (3M Unitek) | Victory MBT (29) (3M Unitek) | 17.1 | SmartClip was no more effective at reducing irregularity during the initial stage of treatment than a conventional twin bracket. | Moderate |
| Miles et al | 2006 | Prospective cohort (Split-mouth design) | Damon2 (58) (SDS Ormco) | Victory MBT (58) (3M Unitek) | 16.3 | The Damon2 was no better during initial alignment than a conventional bracket. Damon2 had a higher bracket failure rate. | Moderate |
| Miles | 2007 | Prospective cohort (split-mouth design) | SmartClip (14) (3M Unitek) | Conventional MBT twin (14) (3M Unitek) | 13.1 (median) | No significant difference in the rate of en-masse space closure between SmartClip brackets and conventional twin brackets tied with stainless steel ligatures was found. | Moderate |
| Paduano et al | 2008 | Cross-sectional | SmartClip (10) (3M Unitek) In-Ovation (10) (GAC International) Time2 (10) (American Orthodontics) |
GAC Ovation with stainless steel ligatures (10) GAC Ovation with elastic ligatures (10) (GAC International) |
Not reported (age range, 12-30 y) |
SL systems showed quicker and more efficient wire removal and placement for late orthodontic treatment phases. The ligation time in the mandibular arch was affected by the type of SL appliance used. | High |
| Pandis et al | 2006 | Prospective cohort | Damon2 (43) (SDS Ormco) | Microarch (19) (GAC International) | 14 | No significant difference in failure incidence was noted between SL and edgewise brackets bonded with either conventional acid etching or self-etching primer in either arch. | Moderate |
| Pandis et al | 2007 | Prospective cohort | Damon2 (27) (SDS Ormco) (mandibular incisor torque: –6°) |
Microarch (27) (GAC International) (mandibular incisor torque: –1°) |
Damon2: 13.5 Microarch: 13.9 |
No significant difference in the time required to correct mandibular crowding was found between the 2 groups. However, for an irregularity index value <5, self-ligating had 2.7 times faster correction. There were overall increases in mandibular incisor proclination and intercanine width for both groups after alignment, with no significant difference between the groups. The self-ligating group had a statistically greater intermolar width increase. | Low |
| Pandis et al | 2009 | Prospective cohort (completion of part of 2007 study) | Damon2 (27) (SDS Ormco) (mandibular incisor torque: –6°) |
Microarch (27) (GAC International) (mandibular incisor torque: –1°) |
Damon2: 13.6 Microarch: 13.9 |
There were overall increases in mandibular incisor proclination and intercanine width for both groups after treatment, with no significant difference between the groups. The self-ligating group had a statistically greater intermolar width increase after treatment. | Low |
| Scott et al | 2008 | Randomized controlled trial | Damon3 (32) (SDS Ormco) (mandibular incisor torque: –1°) |
Synthesis (28) (SDS Ormco) (mandibular incisor torque: –1°) |
Damon3: 16.2 Synthesis: 16.4 |
Damon3 was no more efficient than conventional ligated preadjusted brackets in initial or overall rate of mandibular incisor alignment. Alignment was associated with increased intercanine width, maintenance of intermolar width, some reduction of arch length, and proclination of mandibular incisors for both appliances, but the differences were not significant. | Low |
| Turnbull and Birnie | 2007 | Cross-sectional | Damon2 (140) (SDS Ormco) | Orthos (122) (SDS Ormco) | Damon2: 13.7 Orthos: 14.4 |
Damon2 had a significantly shorter mean archwire ligation time for both removing and placing wires. | Moderate |
Of the 16 studies, 4 were judged to have a low risk of bias, 8 were categorized as having moderate risk, and 4 were considered to have high risk ( Table ; Appendix 3 ). The 4 studies with low risk of bias were the 2 randomized controlled trials and the 2 prospective cohort studies. Most other cohort studies were judged to have moderate risk of bias, and those with high risk of bias were mainly cross-sectional studies.
The studies were further divided into 3 categories based on the aspects of self-ligating brackets that were investigated: efficiency, effectiveness, and stability. Eleven studies had results that could be used for meta-analyses.
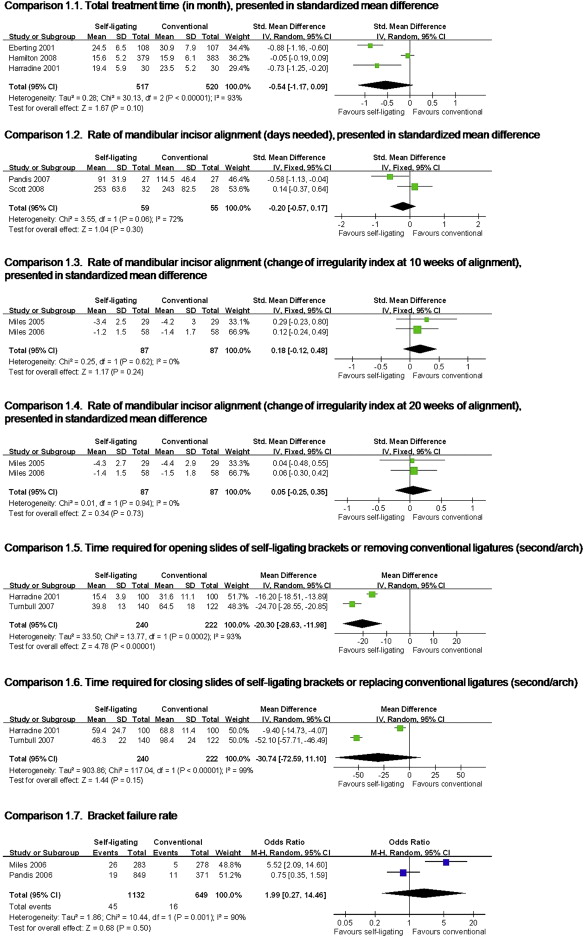
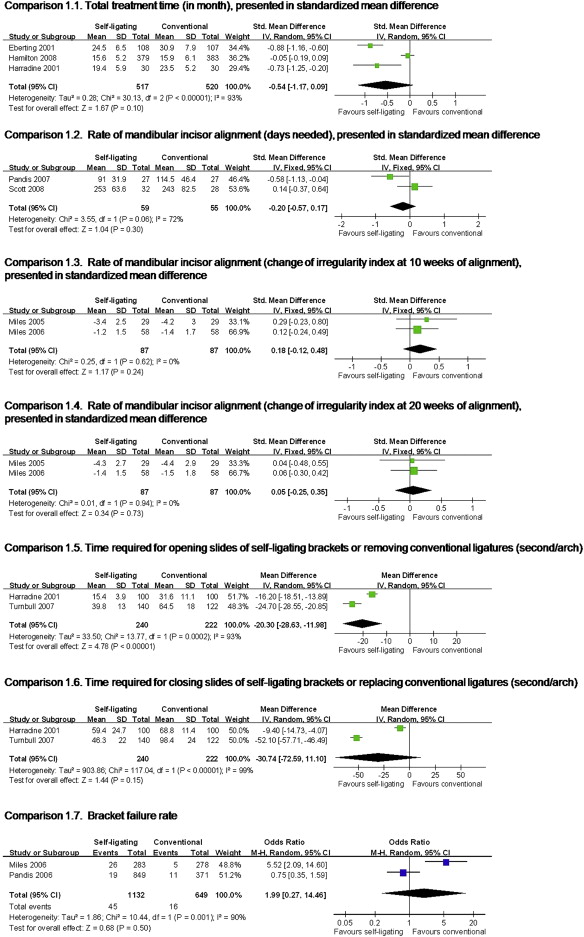
Eleven studies investigating the efficiency of self-ligating brackets compared with conventional brackets were identified, and 7 reported results that could be pooled for analysis. The outcomes studied included total treatment time, rate of mandibular incisor alignment, rate of en-masse space closure, number of visits, chair time, and bracket failure rate. Figure 2 (comparisons 1.1-1.7) shows the results of the meta-analysis from 7 eligible studies. Among all the outcomes, only chair time required for opening the slides of the self-ligating brackets or removing the conventional ligatures showed a significant difference between the 2 groups ( P <0.00001). It took 20 seconds less to open the self-ligating brackets per arch than removing the ligatures in the conventional group.
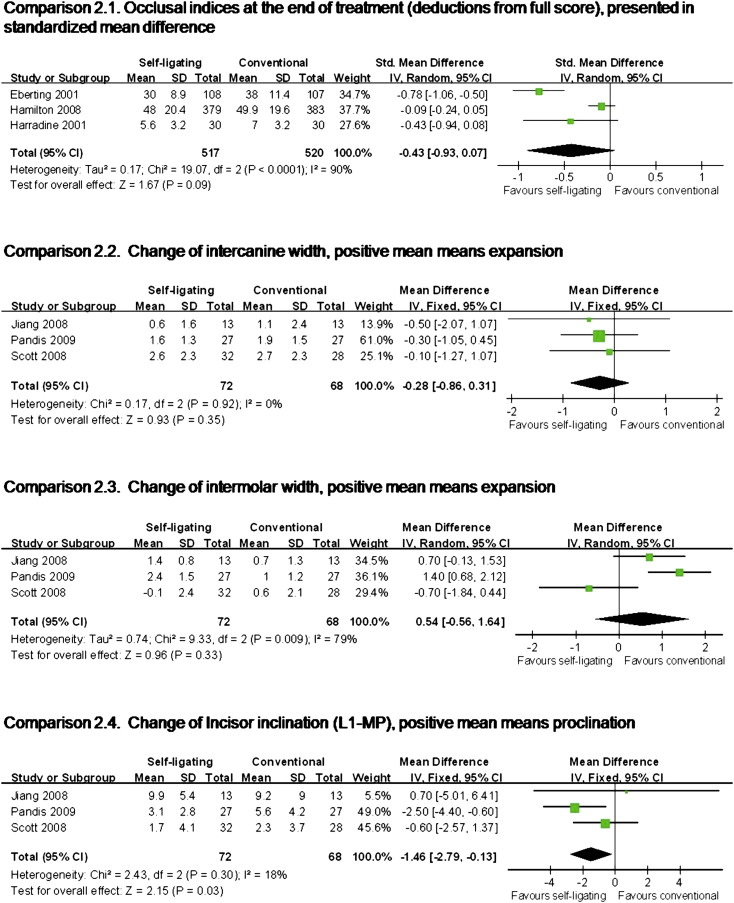
Seven studies investigating the effectiveness of self-ligating brackets compared with conventional brackets were identified. The outcomes that had been studied included occlusal indices, arch dimensions, and mandibular incisor inclinations after incisor alignment or at the end of treatment. Figure 3 (comparisons 2.1-2.4) shows the results of the meta-analysis from these 7 studies. No statistically significant difference was observed between the 2 groups in any outcome category, except for change in mandibular incisor proclination. The self-ligating bracket systems resulted in 1.5° less incisor proclination than the conventional bracket systems.
At this time, no studies comparing the stability of treatment result with self-ligating brackets to conventional brackets were identified.
We intended to assess publication bias, but the small number of studies for each outcome of interest were too few to derive meaning from funnel plots.
Results
The electronic searches identified 114 titles and abstracts. From these, 22 full articles were retrieved for review. Ultimately, 16 articles met the inclusion criteria, including 1 article added from hand searching, 1 article added from contacting an author, 1 article published during this review, and another identified by contacting an expert in the field ( Fig 1 ). Characteristics of the excluded articles are listed in Appendix 2 .
The 16 studies included 2 randomized controlled trials, 10 cohort studies (7 prospective, 3 retrospective ), and 4 cross-sectional studies. All included articles were published in English, except for 1 in Chinese. Characteristics of the included studies are shown in the Table . Most samples comprised adolescent subjects.
| Author | Year | Design | Self-ligating group (number of patients) | Conventional group (number of patients) | Pretreatment mean age (y) |
Authors’ conclusions | Risk of bias |
|---|---|---|---|---|---|---|---|
| Berger and Byloff | 2001 | Cross-sectional | SPEED (20) (Strite Industries) Damon SL (20) (Ormco/”A” Company) Time (20) (Adenta) Twinlock (20) (Ormco/”A” Company) | Mini-twin (40) (Ormco/”A” Company) | Not reported | Total opening and closing time was significantly less for each of the 4 SL designs compared with conventional brackets; SPEED took the least average time and Damon SL the most. | High |
| Eberting et al | 2001 | Retrospective cohort | Damon SL (108) (SDS Ormco) | Type not specified (107) | Not reported | Patients treated with Damon SL had significantly lower treatment times, required significantly fewer appointments, and had significantly higher American Board of Orthodontics scores than those treated with conventionally ligated edgewise brackets. | Moderate |
| Fleming et al | 2009 | Randomized controlled trial | SmartClip (32) (3M Unitek) | Victory (33) (3M Unitek) | SmartClip: 15.9 Victory: 16.6 |
In nonextraction patients with mild mandibular incisor crowding, the SL system used was no more effective at relieving irregularity. Enhanced resolution of irregularity was positively correlated with pretreatment irregularity. | Low |
| Hamilton et al | 2008 | Retrospective cohort | In-Ovation (379) (GAC International) | Victory (383) (3M Unitek) | Not reported | Active SL brackets appear to offer no measurable advantages in treatment time, number of visits, and time spent in initial alignment over conventional preadjusted orthodontic brackets. The number of debonded brackets and other emergency visits were significantly higher in patients treated with active SL brackets. | Moderate |
| Harradine | 2001 | Retrospective cohort | Damon SL (30) (SDS Ormco) (study on speed of ligation: n = 50) (study on bracket complications: n = 25) |
Type not specified (30) (study on speed of ligation: n = 50) (study on bracket complications: n = 25) |
Not reported | Treatment times were 4 months shorter and required 4 fewer visits on average in the Damon group. Slide opening and closure were significantly faster than with conventional ligation. Both types of brackets produced good and equivalent reductions in occlusal irregularity. | Moderate |
| Jiang and Fu | 2008 | Prospective cohort | Damon3 (13) (SDS Ormco) (mandibular incisor torque: –1°) |
Conventional metal preadjusted brackets (13) (Shinya, China) (mandibular incisor torque: –1°) |
Damon3: 14.5 Conventional:15.3 |
In patients with crowding treated without extractions, there were overall increases in the proclination of the mandibular incisors and arch widths in both groups. Patients treated with Damon3 had greater intermolar width increases than those treated with conventional appliances. | High |
| Maijer and Smith | 1990 | Cross-sectional | Activa (14) (“A” Company) | Straight-wire brackets (14) (“A” Company) | Not reported | Reduced chair time was a significant advantage of SL brackets. The operator’s training made little difference in speed, at least with anterior brackets. | High |
| Miles | 2005 | Prospective cohort | SmartClip (29) (3M Unitek) | Victory MBT (29) (3M Unitek) | 17.1 | SmartClip was no more effective at reducing irregularity during the initial stage of treatment than a conventional twin bracket. | Moderate |
| Miles et al | 2006 | Prospective cohort (Split-mouth design) | Damon2 (58) (SDS Ormco) | Victory MBT (58) (3M Unitek) | 16.3 | The Damon2 was no better during initial alignment than a conventional bracket. Damon2 had a higher bracket failure rate. | Moderate |
| Miles | 2007 | Prospective cohort (split-mouth design) | SmartClip (14) (3M Unitek) | Conventional MBT twin (14) (3M Unitek) | 13.1 (median) | No significant difference in the rate of en-masse space closure between SmartClip brackets and conventional twin brackets tied with stainless steel ligatures was found. | Moderate |
| Paduano et al | 2008 | Cross-sectional | SmartClip (10) (3M Unitek) In-Ovation (10) (GAC International) Time2 (10) (American Orthodontics) |
GAC Ovation with stainless steel ligatures (10) GAC Ovation with elastic ligatures (10) (GAC International) |
Not reported (age range, 12-30 y) |
SL systems showed quicker and more efficient wire removal and placement for late orthodontic treatment phases. The ligation time in the mandibular arch was affected by the type of SL appliance used. | High |
| Pandis et al | 2006 | Prospective cohort | Damon2 (43) (SDS Ormco) | Microarch (19) (GAC International) | 14 | No significant difference in failure incidence was noted between SL and edgewise brackets bonded with either conventional acid etching or self-etching primer in either arch. | Moderate |
| Pandis et al | 2007 | Prospective cohort | Damon2 (27) (SDS Ormco) (mandibular incisor torque: –6°) |
Microarch (27) (GAC International) (mandibular incisor torque: –1°) |
Damon2: 13.5 Microarch: 13.9 |
No significant difference in the time required to correct mandibular crowding was found between the 2 groups. However, for an irregularity index value <5, self-ligating had 2.7 times faster correction. There were overall increases in mandibular incisor proclination and intercanine width for both groups after alignment, with no significant difference between the groups. The self-ligating group had a statistically greater intermolar width increase. | Low |
| Pandis et al | 2009 | Prospective cohort (completion of part of 2007 study) | Damon2 (27) (SDS Ormco) (mandibular incisor torque: –6°) |
Microarch (27) (GAC International) (mandibular incisor torque: –1°) |
Damon2: 13.6 Microarch: 13.9 |
There were overall increases in mandibular incisor proclination and intercanine width for both groups after treatment, with no significant difference between the groups. The self-ligating group had a statistically greater intermolar width increase after treatment. | Low |
| Scott et al | 2008 | Randomized controlled trial | Damon3 (32) (SDS Ormco) (mandibular incisor torque: –1°) |
Synthesis (28) (SDS Ormco) (mandibular incisor torque: –1°) |
Damon3: 16.2 Synthesis: 16.4 |
Damon3 was no more efficient than conventional ligated preadjusted brackets in initial or overall rate of mandibular incisor alignment. Alignment was associated with increased intercanine width, maintenance of intermolar width, some reduction of arch length, and proclination of mandibular incisors for both appliances, but the differences were not significant. | Low |
| Turnbull and Birnie | 2007 | Cross-sectional | Damon2 (140) (SDS Ormco) | Orthos (122) (SDS Ormco) | Damon2: 13.7 Orthos: 14.4 |
Damon2 had a significantly shorter mean archwire ligation time for both removing and placing wires. | Moderate |
Of the 16 studies, 4 were judged to have a low risk of bias, 8 were categorized as having moderate risk, and 4 were considered to have high risk ( Table ; Appendix 3 ). The 4 studies with low risk of bias were the 2 randomized controlled trials and the 2 prospective cohort studies. Most other cohort studies were judged to have moderate risk of bias, and those with high risk of bias were mainly cross-sectional studies.
The studies were further divided into 3 categories based on the aspects of self-ligating brackets that were investigated: efficiency, effectiveness, and stability. Eleven studies had results that could be used for meta-analyses.
Eleven studies investigating the efficiency of self-ligating brackets compared with conventional brackets were identified, and 7 reported results that could be pooled for analysis. The outcomes studied included total treatment time, rate of mandibular incisor alignment, rate of en-masse space closure, number of visits, chair time, and bracket failure rate. Figure 2 (comparisons 1.1-1.7) shows the results of the meta-analysis from 7 eligible studies. Among all the outcomes, only chair time required for opening the slides of the self-ligating brackets or removing the conventional ligatures showed a significant difference between the 2 groups ( P <0.00001). It took 20 seconds less to open the self-ligating brackets per arch than removing the ligatures in the conventional group.