Chapter 3 Surgery of the Edentulous and Partially Edentulous Maxilla
Surgery of the Anterior Maxilla
Preoperative Planning and Assessment
A prosthetic plan is completed, with the aid of the restorative dentist, after the amount of bone has been determined. Parel’s classification of the edentulous maxilla is useful for conceptualizing the prosthetic plan (Box 3-1).
| Class I | Only maxillary teeth are missing, but patient has retained alveolar bone almost to its original level. |
| Class II | Teeth and some alveolar bone have been lost. |
| Class III | Teeth and most alveolar bone have been lost to the basal level. |
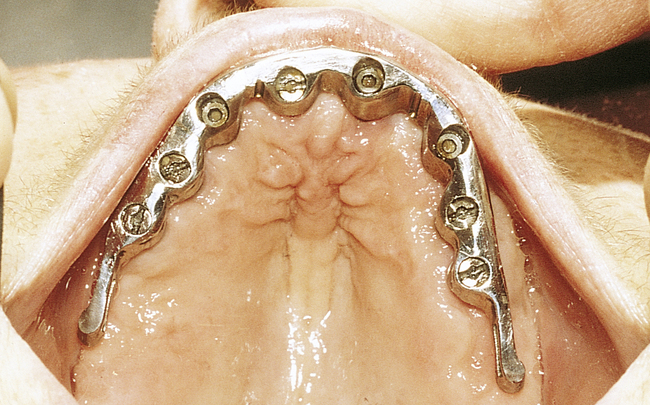
A fixed crown and bridge prosthesis, a fixed-removable (e.g., spark erosion or milled) prosthesis, or a type of removable overdenture prosthesis may be prescribed. The fixed implant-borne and fixed-removable prostheses require at least six (preferably eight) endosseous implants to support a maxillary implant-borne prosthesis adequately. Zygomatic implants are the exception (see later discussion). These traditional fixed or fixed-removable prostheses require posterior maxillary vertical bone height for implants placed in the first molar region. The removable tissue-borne prosthesis requires four implants placed into the anterior maxilla to support a bar, which has retentive vertical stress-breaking attachments. All the edentulous maxillary prostheses usually are fabricated with cross-arch stabilization of the left and right implants.
Placement of Four Implants into the Anterior Maxilla
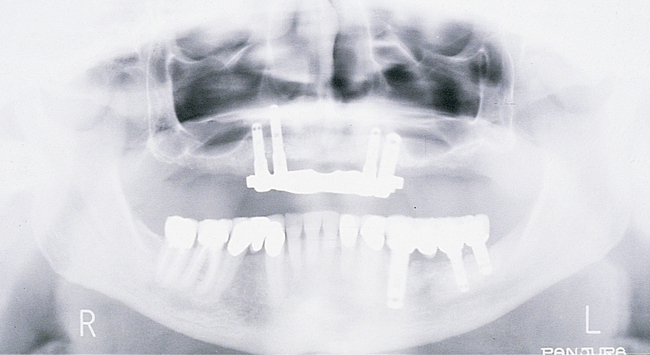
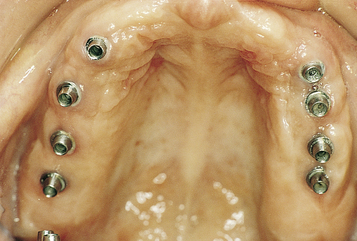
For the patient with adequate anterior vertical bone height and a treatment plan for anterior implants to provide overdenture support, four implants can be placed. Placement of at least four implants is recommended for an implant-supported overdenture in the maxilla, because fewer than four maxillary implants will not predictably resist the forces placed on them (Figure 3-1, A-B, and DVD Figure 3-1, A-F). Two implants are contraindicated to retain a maxillary overdenture.
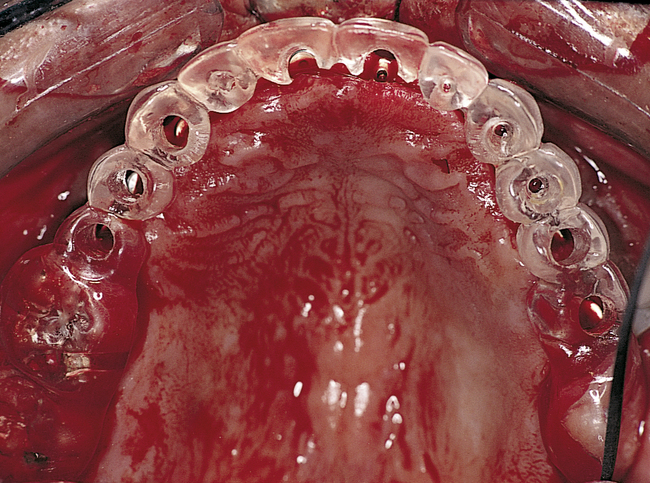
At surgery, the surgeon should understand the prosthetic plan and recognize the ideal locations of the implants. Often these implants can be placed slightly palatal to the crest to engage more of the palatal bone, providing a thicker width of labial bone (Figure 3-2, A-E). A local anesthetic is infiltrated into the labial and palatal regions of the anterior maxilla. Incisions for implants placed into the anterior maxilla usually are placed over or slightly palatal to the crest. Vestibular incisions are avoided in the anterior maxilla, because they can shorten the vestibule and increase the patient’s postoperative discomfort.

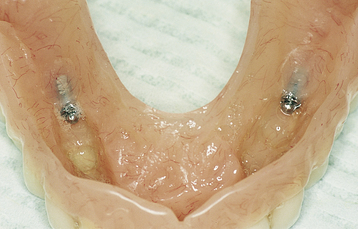
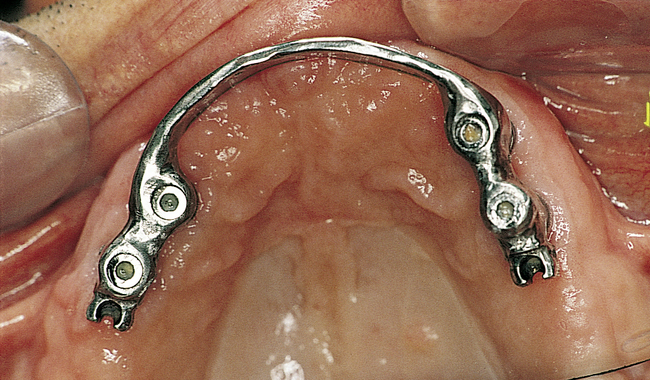
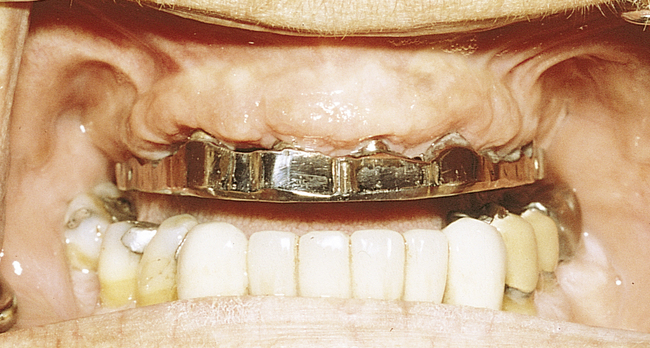
• FIGURE 3-2 D, Distal ASC52 vertical stress-breaking attachments are placed within the denture to provide vertical stability.

• FIGURE 3-2 E, Maxillary prosthesis in place. The palatal portion of the maxillary prosthesis is removed for patient comfort.
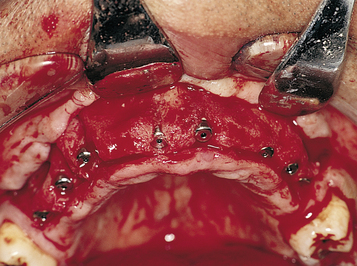
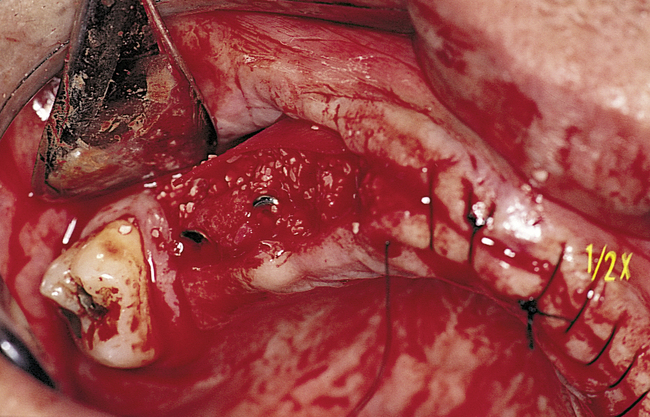
A full-thickness palatal reflection is then accomplished. The contents of the incisive canal are preserved and not incised. The palatal reflection should allow visualization of the slope of the vertical palatal bone to ensure that the surgeon can visualize the insertion of the implants without violating either the labial or the palatal cortical bone, thereby keeping the implant body within bone. The visualization also allows determination of the probable need for osteotomes, either round or flat, to widen the ridge during implant placement.
Subsequent graduating-sized drills initiate and expand the implant site until the final drills are used. If the ridge is excessively narrow, round or flat osteotomes can be used to expand it, or the ridge may require grafting before implant placement. Usually the ridge has sufficient width for placement of the implants. If the ridge width is deficient, the surgeon should consider whether osteotomes can be effective or whether onlay grafting is indicated. If the ridge width is 3 mm, osteotomes can be used to expand it in most cases. However, if the ridge is thin and does not expand as the bone is examined superiorly, the use of osteotomes or ridge splitting in a ridge less than 3 mm is not predictable. For these cases, onlay grafting is indicated and should be discussed with the patient. (See Chapter 4 for examples of onlay grafting of the anterior maxilla with symphyseal bone.)
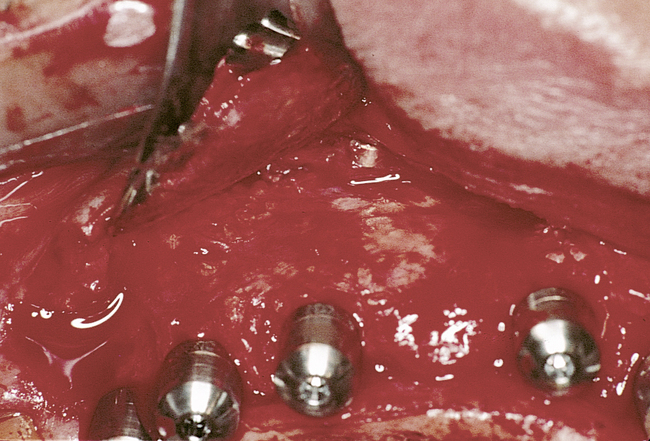
Implants for overdentures typically are placed with their centers slightly palatal to the crest to avoid dehiscence and thin bone over the facial aspect of the implants. The incisive canal should be avoided as a site for implant placement. Implants should be placed to prevent dehiscence of the implant within the incisive canal. Specifically, implants for overdentures are placed in the canine and premolar locations, depending on the availability of bone. An implant can be placed in the lateral incisor position if necessary. However, implants placed in the central incisor locations complicate the prosthetic rehabilitation, because the presence of the abutments and bar near the midline may result in excessive palatal bulk in the denture; this outcome may be bothersome to the patient.
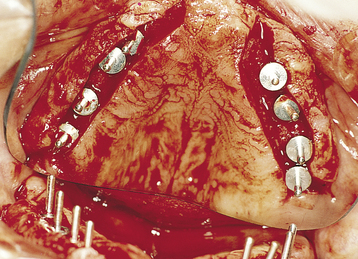
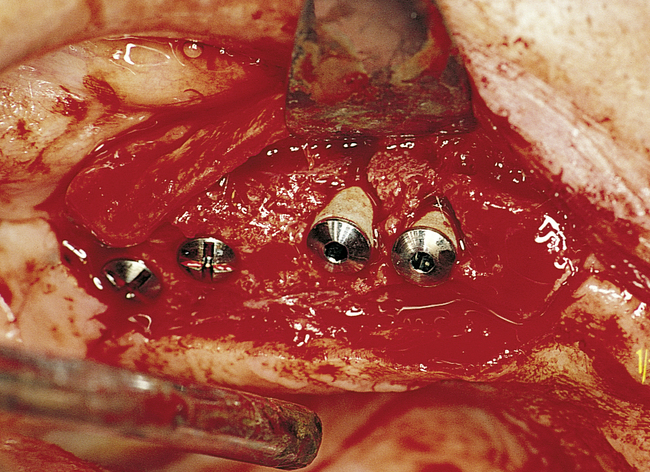
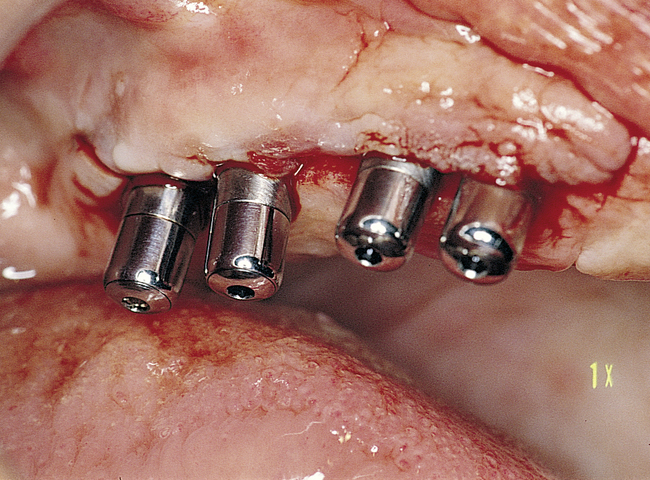
Placement of Eight Implants without a Graft
The edentulous patient with a Class I maxilla requires only the placement of implants to replace the missing teeth (Figure 3-3, A-G). In most patients with a Class I maxilla, who have lost their teeth with minimal bone loss, the labial bone has an irregular contour. These patients may benefit from augmentation of the labial bone to smooth the bone contour and enhance the final restoration, especially for those with high smile lines (Figure 3-4, A-I).

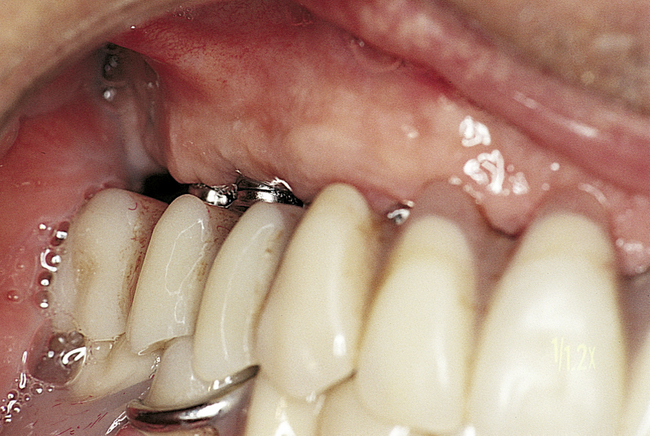
• FIGURE 3-3 E, Final restoration is placed. The space created allows for easy maintenance of oral hygiene.
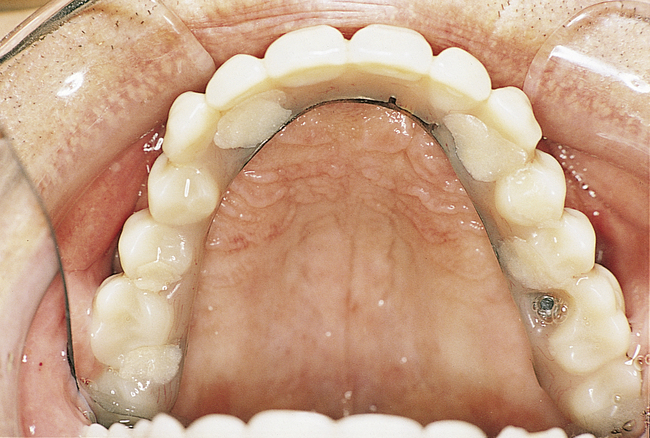
• FIGURE 3-3 F, Occlusal view showing the implants positioned within the confines of the teeth as planned.






• FIGURE 3-4 H-I, Final prosthesis with appropriate gingiva form and papilla.
(Prosthetics by Dr. Steven Locasio.)
Patients with a Class II maxilla, who have lost their teeth but have a moderate amount of bone, must have an esthetic evaluation. These patients may require the labial flange of a removable prosthesis to provide nasolabial support. They may have sufficient bone for the placement of implants, but without additional lip support, the result may be compromised (Figure 3-5, A-F). The patient’s denture can be duplicated in clear acrylic, and the flange can be completely removed. If the modified denture is placed into the mouth and the lip support is adequate, a fixed restoration can be used. However, the locations of the implants and the need for removable prosthetics to aid in the maintenance of effective oral hygiene also are important considerations.





Patients with a Class III maxilla, who have lost their teeth and most of the alveolar bone to the basal level, benefit from a fixed-removable restoration (Figure 3-6, A-E).
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


