Introduction
The purpose of this study was to analyze the design and surface morphology of 2 brands of mini-implants before and after 12 to 18 months of clinical use.
Methods
We studied 22 mini-implants sold in the Brazilian market by 2 companies (Forestadent, Pforzheim, Germany; and Dental Morelli, Sorocaba, São Paulo, Brazil). The surface morphology of the mini-implants was analyzed by scanning electron microscopy before and after insertion in the oral environment to aid orthodontic movement.
Results
The Forestadent and the Morelli mini-implants showed different shapes (size, screw thread design), and the surface morphology changed after clinical use. The most important surface morphology alterations after clinical use were strain in several parts and fracture of the active thread part of some mini-implants.
Conclusions
The results of the analyses showed that the screw threads of the mini-implants differ in pitch, angle, and length. The mini-implants also showed differences in body design, active tip, and taper. These differences affect the performance of the mini-implants. After clinical use, all mini-implants showed surface degradation, plastic deformation, and some fractures.
Highlights
- •
The morphology of mini-implants was analyzed before and after clinical use.
- •
The 2 types of mini-implants had different shapes and morphology.
- •
After use, the mini-implants showed plastic deformation and surface degradation.
- •
The performance of orthodontic mini-implants can be affected by the manufacturing design.
Orthodontic anchorage can be defined as the resistance to an unwanted tooth movement. Every orthodontic case requires careful and individualized planning with special attention in the selection of the anchorage device. Orthodontic treatments use different techniques to increase tooth anchorage, such as extraoral appliances, transpalatal bars, lingual arches, Nance buttons, and intermaxillary elastics. Although these techniques are efficient, in many patients they allow a certain degree of mobility of the anchorage devices and lose anchorage, and their effectiveness depends on patient compliance.
Mini-implants are useful devices in orthodontic treatment because they offer stable anchorage. Their advantages are that they promote a vector of forces that is favorable to certain types of tooth movement, prevent unwanted effects, and improve the control of resultant forces during orthodontic treatment. These devices are small and can be inserted in several alveolar bone areas; their placement is simple, and they have a low cost, can be immediately loaded after insertion, and are easily removed after clinical use. However, because excellent stability is necessary for these devices, it is important to know their shape, size, and mechanical properties to plan a successful orthodontic treatment.
The shape of the mini-implant must offer mechanical anchorage through bone-implant contact and allow load distribution in a way that will not damage bone physiology. The shape should also cause little insertion trauma and allow primary stability. The primary stability of the mini-implant can be affected by the shape of the screw, and the length, diameter, and profile of the screw threads (shape, depth, pitch).
Normally, mini-implants for orthodontic applications are manufactured with a titanium-aluminum-vanadium alloy or stainless steel F138. These biomaterials have good corrosion resistance, are biocompatible, and have mechanical resistance to endure not only placement and removal torques, but also the orthodontic forces during treatment.
As to the clinical effectiveness of mini-implants, even though high success rates were found in several studies, there are cases of failure related to poor use of the technique and problems such as peri-implantitis and fracture.
Even though mini-implants are routinely used as temporary anchorage devices, few studies have analyzed their surfaces after clinical use in patients who have had orthodontic correction. The purpose of this study was to compare the surface morphology of 2 brands of mini-implants before and after clinical use.
Material and methods
Twenty-two mini-implants made with titanium-aluminum-vanadium alloy were used in this study. The implants were bought in the Brazilian market, and there was no involvement of manufacturers. They were divided into 2 groups: group F: Forestadent, Pforzheim, Germany; and group M: Dental Morelli, Sorocaba, São Paulo, Brazil. The Forestadent mini-implants had a nominal diameter of 1.7 mm, a 1.0-mm cylindrical transmucosal profile, and an 8.0-mm length. The Morelli group had a diameter of 1.5 mm, a 2.0-mm conical transmucosal profile, and an 8.0-mm length.
One mini-implant from each manufacturer was analyzed with a scanning electron microscope before clinical use, and 10 were inserted into patients. The patients were randomly chosen; they needed this device as temporary anchorage during corrective orthodontic treatment for several kinds of tooth movement, such as retraction of anterior teeth, molar distalization, intrusion, and mesialization. The mini-implants were clinically used between 12 and 18 months; average use was 15.5 months.
The clinical procedure was similar for the insertion and use of all mini-implants.
- 1.
Insertion and removal. The mini-implants were inserted and removed by the same operator (G.M.), who followed the placement protocol recommended for a self-drilling mini-implant. The mini-implants were removed at the end of the orthodontic treatment of each patient. The mini-implants were inserted in the maxilla and the mandible.
- 2.
Cleaning. After removal, all mini-implants were ultrasonically cleaned (Cristófoli, Campo Mourão, Paraná, Brazil). The cleaning process used distilled water and enzymatic detergent (EndoZime; Planitrade, Porto Alegre, Rio Grande do Sul, Brazil).
- 3.
Storage. After the devices had been cleaned, they were stored in plastic containers, with an identification label for each sample and records containing the name of the patient, the name of the manufacturer of the mini-implant, its nominal dimensions, clinical use time, and site of placement.
- 4.
Data collection. The mini-implants were analyzed by scanning electron microscope (Quanta FEG 250; FEI, Hillsboro, Ore) using different magnifications (50-1000 times). Several areas of the head surface, the transmucosal profile, and the active thread were analyzed. The morphology of the samples before and after use was compared to assess the mini-implants’ alterations after clinical use and contact with the oral environment. Microscopic images taken with a camera (D10; Pentax, Tokyo, Japan) with a 100-mm macro lens and a stabilizing system for consistent imaging.
For comparison purposes, the threads of the 2 types of mini-implants were counted, and the shape and dimensions of several parts of the mini-implants were measured. The pitch (distance between the consecutive threads), flank width (distance between the root and the crest), and taper were measured. There is a relationship among pitch size, number of threads, and length; the greater the number of threads to the same mini-implant length, the smaller the pitch.
The purpose of the analysis of the active tip was to verify its shape and dimensions. This part of the screw has the highest risk of fracture during clinical insertion and removal.
Resistance to fracture can be increased by varying the thread and body profile of the mini-implant, which can be conical with self-drilling threads or cylindrical with cutting threads. To assess the taper of the screws, the diameter of the internal thread was measured with the scanning electron microscope. Taper is calculated as the difference between the largest and smallest diameters of the thread divided by the length of the active part.
Statistical analysis
The chi-square nonparametric test at 5% probability ( P <0.05) was used to compare the independent groups before and after clinical use.
Results
Differences in the shape and morphology were observed between the mini-implant groups. The mini-implants in group F had fewer threads (8 threads) than those in group M (11 threads). The transmucosal profile in group F was cylindrical, and group M was tapered ( Fig 1 ).
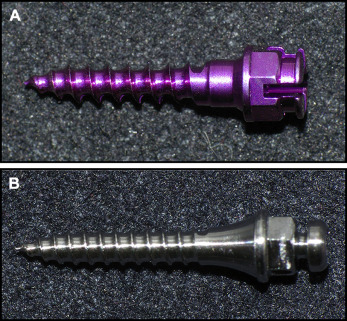
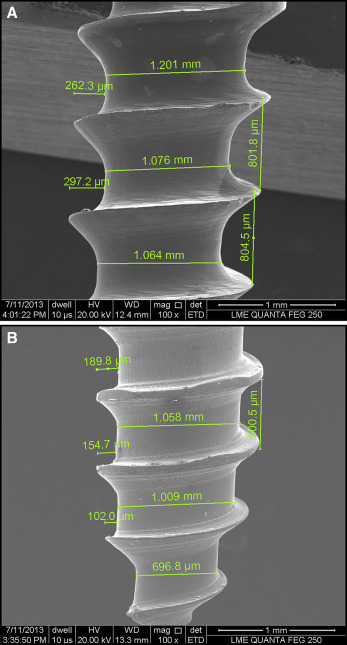
Figure 2 shows that the devices in group M have a smaller pitch size (600 μm) than those in group F (800 μm).
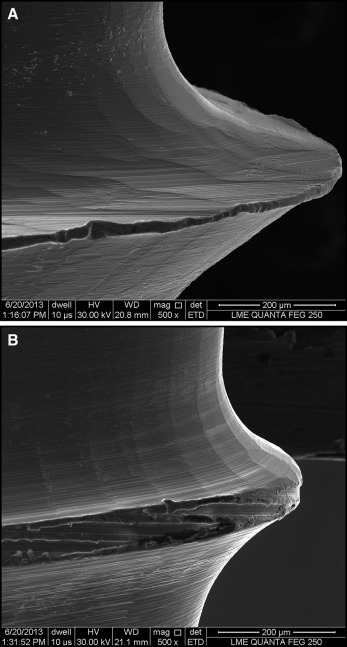
The surface morphology analysis showed that the group F of mini-implants has threads with more tool marks from the manufacturing process, and the crest is sharper and thinner ( Fig 3 ). The group F thread profile is triangular with characteristics of less mechanical resistance. The group M device had a smooth surface, good finish, rounded thread root and crest, and greater external diameter. The Table shows the differences between 2 groups.
| Thread | Morelli | Forestadent |
|---|---|---|
| Number of threads | 11 | 8 |
| Transmucosal | Tapered | Cylindrical |
| Pitch (μm) | 600 | 800 |
| Side flank | Smooth | Grooves |
| Crest | Rounded | Sharper |
| Shape | Rounded | Triangular |
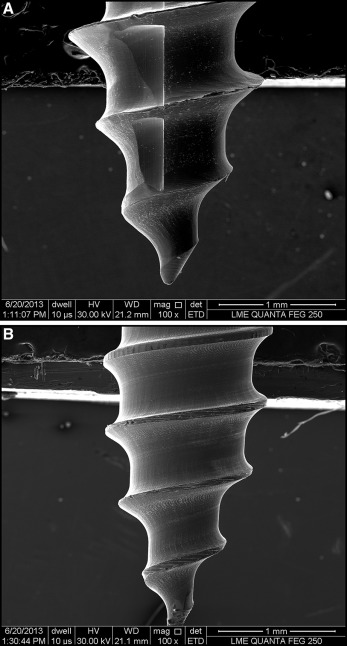
Although there are differences in the body and in the thread profiles, the samples of both groups showed that the tip region had similar characteristics and shapes ( Fig 4 ).
The height or depth of the thread (distance between the crest and root) in group F (241.9 μm) was greater than in group M (194.7 μm). For mini-implants with the same external diameter, as the depth of the thread increases, the insertion thread into bone increases, and the mechanical stability increases.
Taper was calculated by measuring the minor diameter at the beginning of the active thread, and the minor diameter at the end of active tip. Mini-implants in group F had a greater taper than did those in group M. Group F showed an internal thread reduction of 48%, and group M had a 34% reduction.
Microscopic analysis of the mini-implant surface showed degradation after clinical use. The mini-implants showed variations in color, gloss, and surface polish. All mini-implants had a dull surface. These changes were observed in both the head of the screw, which is exposed to the oral environment, and the active thread, which is in contact with bone. This result shows that the oxide layer of the titanium-aluminum-vanadium mini-implant is subject to a change in thickness and, possibly, in the type of oxide. However, this analysis was not the objective of this study.
The mini-implants showed alterations in surface morphology in the thread after they had been subjected to insertion torques and clinical orthodontic movements. In group M, it was observed that 20% of the screws kept the active thread intact, and 80% had some plastic deformation compared with the original state. In this group, the deformation was similar to the compression of the thread crest. Probably, the plastic deformation happened during insertion of the mini-implant ( Fig 5 ). It was observed that 100% of the deformations of the group M mini-implants were located in the middle third, between the sixth and ninth screw threads. Apparently, this is the place with higher compressive stress on the mini-implant during clinical use ( Fig 6 ).
Figure 7 shows that the plastic deformation of the group F mini-implants after clinical use was negligible.


