Skeletal open-bite malocclusion is frequently discussed in orthodontics. Diagnosis, treatment, and retention can be difficult because this malocclusion has numerous correlated etiologic factors. The earlier this malocclusion is corrected, the better the prognosis will be, especially when the problem is skeletal. This article presents a patient with a skeletal open bite and a thumb-sucking habit who was treated in the mixed dentition with an orthodontic appliance that included an acrylic occlusal splint along with spring-loaded blocks to guide the vertical force against the posterior teeth and the alveolar process. The usefulness of the appliance as a habit-breaking therapy is also highlighted.
In the study of the formation of malocclusion, vertical facial dysplasia is treated with special deference. This attitude is a by-product of many decades of clinical, experimental, and morphologic investigations and reflects the rich variety of opinions concerning the nature of vertical dysplasia. The vertical problem varies from a deep or an excessive overbite to the opposite extreme, an open bite.
Even though the prevalence of open bite is low (3.5% in patients aged 8-17 years ), correcting the problem has proven to be extremely challenging. The cause of an anterior open bite is multifactorial and can be attributed to a combination of skeletal, dental, and soft-tissue effects.
A patient with a skeletal open bite has superimposed craniofacial dysplasia. Development of a skeletal open bite has been attributed to lack of coordination between condylar-glenoid fossa growth (horizontal factor) and vertical growth of the maxilla and the dentoalveolar processes (vertical factor). Increased expression of vertical factors rather than horizontal factors results in clockwise rotation of the mandible, leading to skeletal anterior open bite. This type of disturbance could also be produced by a long-standing finger-sucking habit, converting a dental open bite into a skeletal open bite.
According to Brodie, patterns of facial growth are established early in development. But the use of orthodontic appliances to correct an open bite in the deciduous dentition is not indicated because there is no reason to change a habit or move teeth if the situation will spontaneously correct. However, if the open bite is a result of a skeletal discrepancy of the maxilla in a patient with a long face, spontaneous correction might not occur. The ideal period to begin treatment is during the mixed dentition; if the malocclusion is corrected during the deciduous dentition, it will recur because of continued growth changes. In the mixed dentition, the most important step in correcting an open bite associated with abnormal habits is to eliminate the habits with behavior-modification techniques, accompanied by speech therapy; if necessary, a removable functional appliance with a vertical crib can be used. It is important to present this treatment to the child as an aid and not as a punishment. In about half of the patients, thumb sucking ceases immediately, and the anterior open bite closes relatively quickly. After the habit is eliminated, it is important to maintain the appliance for 3 to 6 months. However, when the open bite is associated with skeletal features such as an increased mandibular plane angle, anterior face height, and extruded posterior teeth, it is necessary to redirect maxillary growth with molar intrusion, to rotate the mandible in an upward and forward direction.
Many approaches have been suggested to modify this early developmental pattern, but only posterior bite-blocks proved to be effective in producing condylar growth and forward rotation of mandible. To actively intrude the posterior teeth, Iscan et al and Akkaya and Haydar suggested the use of a spring-loaded bite-block.
Our objective was to present an alternative treatment for anterior skeletal open bite associated with thumb sucking during the mixed dentition with a removable mandibular acrylic occlusal splint and a spring-loaded block, based on the appliance designed by Woodside and Linder-Aronson. This modified appliance guides the vertical force against the posterior teeth and the alveolar process. The effectiveness of the appliance as a habit-breaking therapy is highlighted.
Case report
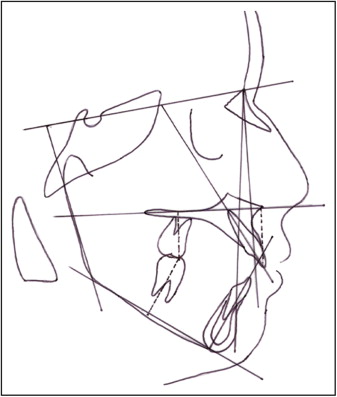
A boy, aged 9 years 4 months, was initially referred by his pediatrician to an orthodontic department ( Figs 1 and 2 ). The clinical examination showed a skeletal open-bite malocclusion associated with a thumb-sucking habit. There was no history of respiratory problems. The patient had all the cephalometric features of skeletal open bite, including steep mandibular plane angle, obtuse gonial angle, increased lower anterior face height, and excessive posterior dental heights ( Table I ). Clinically, the open bite was 7 mm.

| Measurement | Pretreatment | Posttreatment | 1 year after retention |
|---|---|---|---|
| Sagittal | |||
| <SNA (°) | 80 | 80.5 | 81 |
| <SNB (°) | 75 | 77.5 | 78 |
| <ANB (°) | 5 | 3 | 3 |
| Vertical | |||
| <SN-GoGn (°) | 36 | 33.5 | 33 |
| <Ar-Go-Me (°) | 132 | 129 | 128 |
| N-Me (mm) | 110 | 107 | 106 |
| S-Go/N-Me × 100% | 58 | 61.5 | 62 |
| Dental | |||
| Maxillary incisor-NA (mm) | 4 | 3 | 3 |
| Mandibular incisor-NB (mm) | 4.5 | 3.5 | 3 |
| Maxillary incisor^ ANS-PNS (mm) | 26 | 27 | 27 |
| Mandibular incisor^ Go-Gn (mm) | 38 | 39 | 39 |
| Maxillary molar^ ANS-PNS (mm) | 26.5 | 25 | 24.5 |
| Mandibular molar^ Go-Gn (mm) | 36 | 35.5 | 35 |
| Overjet (mm) | 4.5 | 2 | 2 |
| Overbite (mm) | −7 | 1 | 1.5 |
The main problem was the anterior open bite, which was of skeletal origin, as confirmed by cephalometric analysis; it impaired his dental esthetics. The severe vertical skeletal dysplasia was most likely hereditary, but the sucking habit probably contributed to the development or exacerbation of the malocclusion.
Therefore, the following objectives were established: (1) eliminate the sucking habit and redefine perioral muscular function, (2) establish a normal overbite, (3) improve facial appearance and labial balance, (4) reduce the vertical skeletal dysplasia, and (5) align and level the teeth with corrective orthodontics, if necessary, in the permanent dentition.
Orthodontic alternatives were limited because of the patient’s age. The treatment objective for the maxilla included altering the vertical position through posterior impaction. The following options were discussed with the patient’s family: early treatment with removable appliances or fixed-appliance treatment after all permanent teeth had erupted.
For removable therapy, 2 options were given to the patient: extraoral appliance (high-pull headgear or vertical pull chincup) and modified posterior bite-blocks. The patient refused the extraoral appliance. Modified posterior bite-blocks had several advantages. They would (1) normalize the open bite, (2) prevent extrusion of the posterior teeth, (3) prevent an increase of the open bite, and (4) prevent downward and backward mandibular rotation. But this alternative also had several disadvantages: the treatment time would not be shorter, and success would depend on patient compliance.
The second alternative was fixed appliances in the permanent dentition. This treatment would normalize the open bite, but we would have to wait for all permanent teeth to erupt. Treatment costs would be greater, and orthognathic surgery might be required.
After we discussed the treatment options with the patient and his parents, it was decided to use the modified bite-blocks. Although posterior bite-blocks had been used previously for control of vertical dimensions, their usefulness in controlling the sucking habit has not been considered. By virtue of its spring action, the appliance stimulates continuous masticatory movements: ie, an oral gymnastic effect. It was thought that this oral gymnastic effect could also act as a habit-breaking therapy by diverting the patient’s attention toward holding the appliance in the mouth. Hence, the option of a spring-loaded bite-block was discussed with the patient and his parents, and informed consent was obtained.
To study the treatment effects, study models, cephalograms, and electromyograph recordings of the masseter and temporalis muscles at rest and at maximal clenching were taken at the start of treatment and after closure of the open bite.
The construction bite was taken by hinging the mandible open about 3 to 4 mm beyond the rest position in centric relation. This resulted in 6 to 8 mm of vertical opening in the second premolar region. Working models were then mounted on the 3-point articulator with the wax construction bite in place.
The appliance had 2 parts: a mandibular removable plate with occlusal coverage and an acrylic bite-block, occlusal to the mandibular plate ( Fig 3 ). The mandibular plate acrylic was extended incisally to the cingulum of the incisors to prevent their supraeruption.



