Snoring and Obstructive Sleep Apnea
Definition
Sleep-related breathing disorders constitute a spectrum of clinical entities with variations in sleep structure, respiration, and blood oxygen saturation. The spectrum ranges from mild snoring to severe obstructive sleep apnea (OSA) ( Fig. 9.1 ). Obesity-hypoventilation syndrome (formerly called Pickwickian syndrome) is the term used to describe a syndrome characterized by severe obesity, daytime hypoventilation, and sleep-disordered breathing.

Snoring, upper airway resistance syndrome (UARS), and OSA are the main subjects of this chapter. All of these sleep-related breathing disorders are caused by upper airway obstruction of variable degree, leading to resistance to airflow during respiration. Attempts to breathe continue despite the obstruction. A related disorder, central sleep apnea, is the cessation of breathing that is caused by disruption of central nervous system (CNS) ventilatory drive; this type of apnea usually is associated with an underlying medical problem such as heart failure and is not caused by obstruction, so it is not included in this chapter.
Snoring may occur alone or may be caused by a more significant airway impairment. Snoring is the result of vibration of the soft tissues of the upper airway, primarily during inspiration. Primary snoring is sometimes referred to as simple snoring or benign snoring. It occurs as an independent entity and is not associated with disrupted sleep or complaints of daytime sleepiness and occurs without abnormal ventilation. Findings on an overnight sleep study, or polysomnogram (PSG), are normal. UARS is a clinical entity midway between primary snoring and OSA that is characterized by snoring, variable complaints of daytime sleepiness, and fragmentation of sleep. In UARS, a PSG typically demonstrates only a modest increase in ventilatory efforts, but the impairment is not severe enough to be classified as OSA. OSA, in contrast, is characterized by loud snoring and excessive daytime sleepiness with episodes of complete cessation of breathing (apnea) or significantly decreased ventilation (hypopnea) caused by airway obstruction during sleep along with significant fragmentation of sleep architecture. A PSG demonstrates significant abnormalities in sleep architecture, ventilation, and blood oxygen saturation.
COMPLICATIONS: Fragmented sleep leads to sleepiness, decreased alertness, irritability, poor concentration, lack of libido and memory loss. These can lead to poor job performance, marital discord, and driving impairment. The cardiovascular effects can result in hypertension, increased risk of stroke, congestive heart failure, pulmonary hypertension, cardiac arrhythmias, and death.
To appreciate the consequences of sleep-related breathing disorders, it is necessary to understand the aspects of normal sleep. Normal sleep patterns vary with age but are nevertheless similar across patient groups; thus, for illustrative purposes, the sleep of young adults is discussed here. Normal sleep occurs in two phases: non–rapid eye movement (NREM) sleep and rapid eye movement (REM) sleep ( Table 9.1 ).
| Stage Plus EEG Characteristics | Percent of Sleep (%) |
|---|---|
| Relaxed wakefulness | <5 |
| Non–rapid eye movement sleep (NREM) | |
| Stage 1: transitional; easy arousal | 2–5 |
| Stage 2: sleep onset; K-complexes (sleep spindles) | 45–55 |
| Stage 3: high-voltage, high-amplitude slow waves | 3–8 |
| Stage 4: increased numbers of high-voltage slow waves | 10–15 |
| Rapid eye movement sleep (REM) | 20–25 |
| Associated with desynchronized brain waves on EEG, muscle atonia, bursts of rapid eye movement |
The phases of sleep are characterized by distinctive patterns on the electroencephalogram (EEG), as well as by the presence or absence of eye movements. NREM sleep occurs in three (or four) stages and generally is characterized by synchronous and increasingly high-amplitude, lower frequency brain waves, mental inactivity, and physiologic stability ( Fig. 9.2 ). The NREM sleep state sometimes is referred to as “a quiet brain in a quiet body.” Stage 1 NREM is a brief, transitional stage that lasts only a few minutes between wakefulness and sleep and from which the person can be easily aroused. Stage 2 NREM is the initial stage of true sleep, from which arousal is more difficult. The appearance of EEG waves called sleep spindles, or K-complexes, identifies this stage, which typically lasts 10 to 25 minutes. Stage 3 is characterized by the appearance on the EEG of high-voltage, high-amplitude slow waves that last for a few minutes and then undergo transition into stage 4, with more frequent and higher amplitude slow waves. This stage lasts for 20 to 40 minutes. Stages 3 and 4 often are combined, and this combination is referred to as slow-wave sleep (SWS).

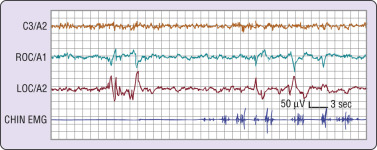
After a period of NREM sleep, a “lightening” or change occurs, marked by entry into REM sleep. REM sleep is very different from NREM sleep and is characterized by asynchronous, low-amplitude, high-frequency brain waves, an active brain, physiologic instability, and muscular inactivity. REM sleep state often is described as “an active brain in a paralyzed body.” A key feature is the presence of periodic rapid movement of the eyes with low-voltage EEG waves resembling those typical of wakefulness ( Fig. 9.3 ). Variations in blood pressure, heart rate, and respiration occur, along with general muscle atonia and poikilothermia . Dreaming also occurs during REM sleep. Sleep normally is entered through NREM sleep and progresses to REM. Over the course of a night, sleep cycles between NREM and REM sleep, with each complete cycle (NREM + REM) averaging about 90 minutes. Depending on the length of the sleep period, the sleeper typically passes through four to six cycles per night . The length of time in each stage varies, with NREM predominating in the earlier part of the night and REM predominating in the later part of the night ( Fig. 9.4 ). It is difficult to define a “normal” length of sleep because of multiple variables, including age, environment, circadian rhythm, and medication effects; however, most young adults report that they sleep an average of 7.5 hours per weeknight and 8.5 hours on weekend nights.

To gain the restorative benefits of sleep, it is necessary to progress through the normal stages of sleep. Whereas NREM sleep provides physical restoration, REM sleep provides psychic restoration. If such restoration does not occur because of sleep disruption or sleep fragmentation, cognitive and physiologic disturbances will result. Across the spectrum of sleep-related breathing disorders, different physiologic outcomes may be seen. With primary snoring, the degree of airway resistance is such that vibration of the parapharyngeal soft tissues is the only result. No sleep fragmentation or disruption occurs, and no other impairment of airflow or oxygenation is noted. Generally accepted thought has been that primary snoring has no significant adverse health effects, but evidence now suggests that primary snoring may be a risk factor for type 2 diabetes, hypertension, carotid atherosclerosis, and stroke.
With OSA, increasing resistance to airflow occurs as a result of partial (hypopnea) collapse or complete (apnea) collapse of the airway with the cessation of breathing despite continuing efforts to breathe. Depending on the degree and duration of the collapse, hypoxia, anoxia, and hypercarbia may occur. These changes lead to CNS arousal and transition to a lighter stage of sleep (stage 1 or 2), stimulating partial awakening, relief of the obstruction, and resumption of breathing. Depending on the frequency and duration of arousals during the night, sleep can be fragmented ( Fig. 9.5 ). Sleep quality is poor, and the restorative benefits of sleep are not achieved, leading to a variety of cognitive and physiologic abnormalities.

Neurocognitive effects of OSA include sleepiness, decreased alertness, irritability, poor concentration, lack of libido, and memory loss. These deficits can lead to poor job performance, marital discord, interpersonal conflicts, and driving impairment. Up to 30% of traffic accidents involve sleepy drivers. A systematic review investigating the relationship of crash risk and OSA found that drivers with OSA have a mean crash risk–to–OSA ratio of between 1.21 and 4.89.
In addition to neurocognitive impairment, OSA is associated with numerous cardiovascular effects, including hypertension, stroke, congestive heart failure, pulmonary hypertension, and cardiac arrhythmia. OSA, which is now recognized as one of the treatable causes of hypertension, also has been shown to significantly increase the risk of stroke and death. Patients with OSA have two- to fourfold greater odds of experiencing complex arrhythmias over those without the sleep disorder. It also is thought that treatment of OSA may increase the survival rate among patients with heart failure. In addition, a relationship between OSA, obesity, and metabolic syndrome has been noted. Recent data from the Sleep Heart Health Study provide evidence for an independent relationship among sleep apnea, glucose intolerance, and insulin resistance that may lead to type 2 diabetes. Overall, the mortality rate from all causes is significantly increased among people with untreated OSA and is proportional to the severity.
Epidemiology
Snoring is extremely common in both genders and in all age groups. It is reported to occur in nearly 50% of the adult population, with a higher prevalence among men. Estimates of its prevalence vary widely because detection methods rely heavily on subjective reports by bed partners or parents. Reported prevalence rates for snoring range between 5% and 86% in men and between 2% and 57% in women. Evidence suggests that the frequency of snoring increases with age until about age 60 years, at which time a decrease occurs. In children, snoring is common, with a reported prevalence of 10%. It typically is associated with enlarged tonsils and adenoids, as well as obesity. Snoring also has been reported to increase markedly during pregnancy.
The reported prevalence of OSA varies primarily because of differences in assessment methods and in the number of abnormal respiratory events per hour used to define abnormality. It is estimated that about 2% to 4% of the adult population 30 to 60 years of age is affected by OSA; however, 9% of women and 24% of men have signs or symptoms suggestive of sleep-disordered breathing. Different rates of occurrence have been reported for males and for females, with males affected more often. Variation among racial groups may be due to genetic differences. African Americans, Hispanics, and Asian Americans tend to have a somewhat higher prevalence than whites. About 3% of children are affected with OSA, with the highest prevalence reported between the ages of 2 and 5 years.
Etiology and Pathophysiology
The underlying defect in sleep-related breathing disorders is an anatomically narrowed upper airway combined with pharyngeal dilator muscle collapsibility. The exact pathogenesis, however, is not well understood. Depending on the extent of narrowing, increased resistance to airflow may be clinically expressed as vibration of soft tissues (snoring), reduced ventilation (hypopnea), or complete obstruction (apnea).
Anatomic narrowing may occur at any site in the upper airway from the nasal cavity to the larynx. Within the nasal cavity, septal deviation and enlarged turbinates may cause narrowing. In the nasopharynx, hypertrophic adenoids and tonsils, an elongated soft palate, and an elongated and edematous uvula may be the cause. In the oropharynx, narrowing may be caused by an enlarged tongue, retrognathia, excessive lymphoid tissue, palatine tonsils, or redundant parapharyngeal folds. The most common sites of airway narrowing or closure during sleep are the retropalatal and retroglossal regions. Most patients with OSA have more than one site of narrowing. It also has been demonstrated that the volume of the upper airway soft tissue structures (i.e., tongue, lateral pharyngeal walls, soft palate, parapharyngeal fat pads) is significantly greater in patients with OSA than in normal control participants. Factors that are thought to contribute to enlargement of the upper airway soft tissues in apneic patients include obesity, edema secondary to negative pressures, vibration trauma of the uvula, male gender, and possibly genetics. Other anatomic risk factors for narrowing of the upper airway include retrognathia; a large tongue; a long soft palate; and enlarged uvula, tonsils, and adenoids.
In addition to anatomic narrowing of the airway, an abnormal degree of collapsibility is observed in the pharyngeal dilator muscles surrounding the airway. Patency of the airway depends on a balance between air pressure within the airway and pressure outside of the airway exerted by the parapharyngeal musculature. Muscles that surround the airway receive phasic activation during inspiration and tend to promote a patent pharyngeal lumen by dilating the airway and stiffening the airway walls. Normally, the intraluminal pressure exceeds the external pressure, and the airway remains patent during inhalation and exhalation. Normal function requires coordinated timing and activity of agonists and antagonists and of individual muscles or groups of muscles. The cause of abnormal pharyngeal airway collapse is complex, involving both dynamic and static factors. These factors may include tissue volume, changes in the adhesive character of mucosal surfaces, changes in neck and jaw posture, decreased tracheal tug, effects of gravity, autonomic and catecholamine dysfunction, and decreased intraluminal pressure resulting from increased upstream resistance in the nasal cavity or pharynx.
Clinical Presentation
Signs and Symptoms
The signs and symptoms of sleep-related breathing disorders are those most often described by the bed partner or parent of a patient; they include snoring, snorting, gasping, and breath holding. Snoring is very common, as was previously indicated, and is the most common symptom in patients with OSA. However, most people who snore do not have OSA, but almost all patients with OSA snore. In the Wisconsin Sleep Cohort Study of participants aged 30 to 60 years, 44% of men and 28% of women were habitual snorers, but only 4% of the men and 2% of the women had OSA.
Snoring may be very loud and disruptive to other members of the household. When snoring is the only complaint, the problem most often is primary snoring. If snoring is accompanied by daytime sleepiness with no breathing changes during sleep, UARS must be considered. Snoring accompanied by snorting, choking, gasping, or a complete cessation of breathing is likely to be a sign of OSA. Of note, however, definitive diagnosis of sleep-related breathing disorders cannot be made on the basis of clinical signs and symptoms alone.
Complaints of excessive daytime sleepiness are common in patients with OSA but are not specific, and the problem may be multifactorial. A commonly used subjective measure of sleepiness is the Epworth Sleepiness Scale ( Fig. 9.6 ). This assessment tool has been validated in clinical studies and correlates with objective measures of sleepiness. It is composed of eight questions or situations in which patients are asked how likely they are to fall asleep. Each question is answered on a scale of 0 to 3, with 0 meaning no likelihood of falling asleep and 3 indicating 100% likelihood of falling asleep in that situation. The maximum possible score is 24. A score greater than 10 is indicative of significant daytime sleepiness but is not specific for sleep-related breathing disorders. Other complaints that may be associated with OSA are nocturia or enuresis, mood changes, memory or learning difficulties, erectile dysfunction, morning headache, and dry mouth noted upon awakening.



